

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The worldwide prevalence of obesity is rapidly increasing (1). In 2014, about four in ten adults were overweight, and about one in ten was obese in the world (2). It has been repeatedly reported that excessive body weight—being overweight or obese—is associated with an increased risk of various diseases such as diabetes mellitus, coronary heart disease, and certain forms of cancer (3). However, the effects of overweight on psychiatric disorders are still debated. Many studies have observed that overweight has a negative effect on psychosocial functioning (456), but several others have failed to find such associations (7), and some studies even reported opposite relationships (8).
Interestingly, studies carried out in Asia tended to support the negative association between obesity and depression (9) or did not show a significant association between obesity and mental disorders (710). Some other studies reported mixed results of both negative and absent associations according to gender (1112). They attributed these findings to differences in race/ethnicity, especially as traditional cultures consider an obese body image as a symbol of affluence (910). However, most of these Asian studies included only elderly populations (91112), and few have investigated general populations including young and old adults (10). Recently, young people in Asia have been increasingly exposed to Western culture, wherein slim bodies are admired and overweight individuals are stigmatized as lazy or lacking in self-discipline (1314). Several recent Asian studies have reported increased suicidal ideation in overweight and obese adolescents (15) and an association between obesity and depressive symptoms even in adult populations (16). However, few studies have used valid and reliable diagnostic measures to evaluate the presence of psychiatric disorders according to the criteria of the Diagnostic and Statistical Manual of Mental Disorders Fourth Edition (DSM-IV), and none of these studies included representative samples of the general population. Moreover, most previous studies investigated the association between overweight and depressive disorders, but little is known about the association between overweight and other mental disorders such as anxiety disorders, alcohol use disorders, and nicotine use disorders.
In this study, we explored the association of overweight with psychiatric disorders and suicidality using data from the 2011 Korean Epidemiologic Catchment Area study (KECA-2011), in which a structured diagnostic interview was employed for psychiatric diagnoses and the sample was representative of Korea. We had the following research questions: First, what are the relationships between overweight and various psychiatric disorders and suicidality in the general population of Korea? Second, do age and gender influence these relationships?
MATERIALS AND METHODS
Participants
We used data from the KECA-2011, which is a nationally representative survey on psychiatric disorders in Korea. The study was conducted from July of 2011 to November of 2011. A multistage cluster sampling design was adopted, and the sample was drawn from respondents to the 2010 population census of the community registry office in Korea. Of the 7,650 eligible respondents between the ages of 18 and 74, 6,022 completed face-to-face interviews (response rate: 78.7%). Detailed methods of the KECA-2011 have been described elsewhere (17). All participants were fully informed about the aims and methods of the study, and written informed consent was obtained prior to participation.
Assessment of demographic variables
Data on the following sociodemographic variables were collected during the interview: gender, age (18–29/30–39/40–49/50–59/60–74 years), years of education (less than 6/7–9/10–12/more than 12 years), marital status (married/never married/separated, divorced, or widowed), and employment status (full-time job/part-time job/unemployed).
Assessment of psychiatric disorders
To assess psychiatric disorders on the basis of DSM-IV criteria, all KECA-2011 respondents completed an interview using the Korean version of the Composite International Diagnostic Interview 2.1 (K-CIDI) (18). The CIDI is a structured diagnostic interview based on the DSM-IV. It has been translated into Korean according to the guidelines for CIDI translation. A study comparing the K-CIDI with the Korean version of the SCID-IV demonstrated that the K-CIDI has acceptably high validity and reliability scores (19). Diagnoses considered in this article include depressive disorders (major depressive disorder and dysthymic disorder), anxiety disorders (obsessive compulsive disorder, post-traumatic stress disorder, panic disorder, agoraphobia, social phobia, specific phobia, and generalized anxiety disorder), alcohol use disorders (alcohol abuse and alcohol dependence), and nicotine use disorders (nicotine dependence and nicotine withdrawal). Lifetime diagnoses of these disorders were assessed by trained interviewers.
Assessment of suicidality
We evaluated lifetime suicidality using the modified Suicide Prevention Multisite Intervention Study on Suicidal Behaviors, which was employed in a suicide survey by the World Health Organization (WHO) (20). Among the items, three main questions were used in the present study assessing lifetime suicidal ideation (“Have you ever seriously thought about committing suicide?”), lifetime suicide plan (“Have you ever made a plan for committing suicide?”), and lifetime suicide attempt (“Have you ever attempted suicide?”).
Assessment of overweight
Body mass index (BMI, weight in kilograms divided by height in meters squared) was calculated using participants’ self-reported height and weight. The participants were classified as underweight (BMI < 18.5), normal weight (BMI 18.5–24.9), and overweight (BMI ≥ 25.0) based on WHO criteria (21). In most studies carried out in Western countries, the overweight category was subdivided into overweight (BMI 25.0–29.9) and obesity (BMI ≥ 30.0), and in some studies, obesity was subdivided into obesity I, II, and III (BMI 30.0–34.9, BMI 35.0–39.9, and BMI ≥ 40.0). However, in the current study sample, only 2.2% of the sample had a BMI over 30, which limited statistical power for analyses in this group. Thus, in this study, we did not subdivide the overweight group but instead compared the overweight group (BMI ≥ 25.0) with the normal weight group with regard to the lifetime prevalence of mental disorders and suicidality.
Statistical analysis
All statistical analyses were based on respondent data, which were weighted to approximate the national population with regard to age and sex as defined by the 2010 census of the Korean National Statistical Office. We performed logistic regression analyses to determine odds ratios (ORs) and 95% confidence intervals (CIs), using DSM-IV psychiatric disorders and suicidality as the main outcome variables and the presence of overweight as the principal predictor with the normal weight group treated as the reference group. Adjustments for age, gender, educational attainment, marital status, and employment status was carried out. ORs for mental disorders and suicidality among the overweight group in subgroups defined by age (18–44 years old vs. 45–74 years old) and gender were also estimated. We also tested the interaction between the overweight group and age or gender in predicting the odds of mental disorders and suicidality. Analyses were conducted using IBM SPSS Statistics for Windows (Version 18.0, Armonk, NY, USA). For all tests, P values below 0.05 were considered statistically significant.
RESULTS
Sample characteristics
This sample consisted of 5,872 KECA-2011 respondents (of 6,022 possible) who provided valid data on height and weight. Demographic characteristics are presented in Table 1. The proportion of overweight was higher in men (28.1%) than in women (16.1%). Table 2 shows the demographic characteristics according to the body weight groups. The proportion of people with male gender, old age, and low education level was higher in the overweight than in the normal weight group.
Table 1
Demographic characteristics of the study participants
Table 2
Demographic characteristics of the study participants by the weight groups (the weighted proportions)

Association of overweight with psychiatric disorders
The lifetime prevalence of mental disorders is shown in Table 3. Overweight was associated with increase in the lifetime prevalence of depressive disorders (adjusted OR [AOR] 1.38; 95% CI, 1.07–1.77), controlling for age, gender, educational attainment, marital status, and employment status.
Table 3
Lifetime prevalence of mental disorders and suicidality
BMI, body mass index (kg/m2); CI, confidence intervals; OR, odds ratio; AOR, adjusted odds ratio; OW, overweight; NW, normal weight.
*Overweight was defined as BMI ≥ 25, and normal weight was defined as BMI 18.5–24.9; †Adjusted by age, gender, educational attainment, marital status, and employment status; Bold indicates significant associations (P < 0.05).
Subgroup analyses showed that a formal test for interaction found no significant difference by gender (P = 0.545) or age (P = 0.855). Subgroup analyses for the association between overweight and anxiety disorders also showed no significant difference in ORs according to gender (P = 0.073) or age (P = 0.448). A formal test for interaction found significant variation by gender for the association between overweight and alcohol use disorders (P = 0.018), but the association itself was not statistically significant in either gender. The association between overweight and alcohol use disorders did not vary significantly according to age (P = 0.123). The association between overweight and nicotine use disorders did not vary significantly according to gender (P = 0.155), but ORs differed according to age (P = 0.011).
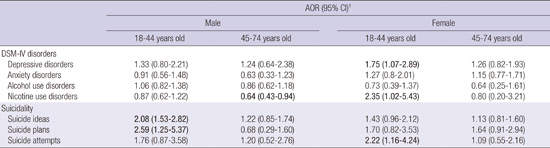
When we divided the participants into four groups according to gender and age (18–44 years old vs. 45–74 years old) (Table 4), the association between overweight and depressive disorders existed only in women aged 18–44 years (AOR, 1.75; 95% CI, 1.07–2.89). Overweight was associated with increased odds of nicotine use disorders in women aged 18–44 years (AOR, 2.35; 95% CI, 1.02–5.43), but the association was in the opposite direction in men aged 45–74 years (AOR, 0.64; 95% CI, 0.43–0.94).
Table 4
Associations between overweight* and psychiatric disorders/suicidality by gender and age
Association of overweight and suicidality
Lifetime prevalences of suicidal ideation, suicide plans, and suicide attempts are shown in Table 2. Overweight was associated with an increase in the lifetime prevalence of suicidal ideation (AOR, 1.42; 95% CI, 1.20–1.68) and suicide plans (AOR, 1.44; 95% CI, 1.02–2.03), controlling for age, gender, educational attainment, marital status, and employment status. The association between overweight and suicide attempts showed an increased OR (AOR, 1.38; 95% CI, 0.97–1.96) with borderline significance (P = 0.072), controlling for demographic variables.
In the subgroup analyses, the associations of overweight with suicidal ideation (P = 0.093), suicide plans (P = 0.527), and suicide attempts (P = 0.835) did not vary significantly according to gender. The associations of overweight with suicidal ideation (P = 0.103), suicide plans (P = 0.416), and suicide attempts (P = 0.420) also did not vary significantly according to age.
When we divided the participants into four groups according to gender and age, the associations of overweight with suicidal ideation (AOR, 2.08; 95% CI, 1.53–2.82) and suicide plans (AOR, 2.59; 95% CI, 1.25–5.37) existed only in men aged 18–44 years while the association between overweight and suicide attempts existed only in women aged 18–44 years.
DISCUSSION
We explored the association of overweight with psychiatric disorders and suicidality among the general population of Korea. We found that overweight was associated with an increase in the lifetime prevalence of depressive disorders, suicidal ideation, and suicidal plans. Although we could not find any significant association between overweight and other mental disorders such as anxiety disorders, alcohol use disorders, and nicotine use disorders, the associations varied according to gender and age.
The association of overweight and depressive disorders existed only in women, a finding consistent with many large epidemiological studies (2223). However, as Simon et al. (6) indicated, considering that a formal test for interaction did not find a significant variation with gender, the lower prevalence of depression in men may have led to a wider CI and a statistically nonsignificant result. Nevertheless, we regarded this gender-specific association between overweight and depressive disorders as a meaningful finding rather than an artifact due to differences in statistical power, because not only did the association between overweight and depressive disorders exist in women aged 18–44 years but also the magnitude of the OR between overweight and depressive disorders was largest in this group. Weight-related stigma, discrimination, and body image disturbances are more pronounced among women than among men (1424). The fact that 63% of high school girls, as compared with 16% of boys, are trying to lose weight demonstrates the difference in norms for ideal body shape between genders and stronger pressure for women to be slim (25). Especially young women who are looking for a partner for a romantic or sexual relationship are more susceptible to obesity stigma (1425). Previous studies carried out in the general population of Korea did not show an association between overweight and depressive disorders in either the whole sample (710) or in women (10). However, in the study of Sunwoo et al. (10), the magnitude of the OR between obesity and depressive disorders was about two times higher in women (OR = 1.13) than in men (OR = 0.6), and it was also about two times higher in the 18–29 years old group (OR = 1.6) than in other age groups (OR 0.65–0.83). Thus, if they had performed subgroup analyses for young women separately, they might have had results similar to ours. The time gap between the studies can be another reason for the differences in results as the young generation in Asia is rapidly absorbing Western norms for body image through movies, TV dramas, and popular songs. The proportion of young individuals who have Westernized norms for body image may be higher in the current study than in previous studies, and this difference may have influenced the results of the association between overweight and psychiatric disorders. In addition, higher prevalence of overweight (BMI > 25) (28.1% vs. 27.5% in men, 16.1% vs. 14.7% in women) in the current study than in the 2006 study using the same methodology could be another reason for the discrepancy (10).
Meanwhile, the direction of the association between depression and overweight could be opposite. In other words, the presence of depressive disorders, especially with atypical features, could increase the appetite, resulting in overweight or obesity. In addition, several antidepressants such as amitriptyline, paroxetine, and mirtazapine also could increase the appetite as an adverse effect, causing weight gain. Unfortunately, we did not collect data for current medications, so we could not rule out the influence of drugs on body weight.
We could not find any significant relationship between overweight and anxiety disorders, a finding in line with previous reports (1026). However, some other studies reported an association between overweight and anxiety disorders (46). One explanation for this discrepancy is that anxiety disorders are composed of heterogeneous disorders, but each study included a different set of anxiety disorders; this resulted in different findings. Another explanation is that BMI cutoffs to define overweight or obesity differed across studies. In Asian populations, the mean or median BMI is lower than that observed for non-Asian populations; hence, the BMI distribution is shifted to the left (27). Thus, the WHO Western Pacific Region has suggested revised Asia-Pacific criteria in which individuals are classified as underweight (BMI < 18.5), normal weight (BMI 18.5–22.9), overweight (BMI 23.0–24.9), and obese (BMI ≥ 25.0) (28). Many Asian studies, including the current study, used 25.0 as the cutoff for overweight (which is actually the cutoff for obesity in the WHO Asia-Pacific criteria) and compared overweight individuals with either those with BMIs between 18.5 and 24.9 (which is normal weight plus overweight in the WHO Asia-Pacific criteria) (10) or those with BMIs between 18.5 and 22.9 (which is normal weight in the WHO Asian-Pacific criteria) (912). Meanwhile, most Western studies compared obese individuals (BMI ≥ 30) with either normal weight individuals (BMI 18.5–24.9) or non-obese individuals (BMI 18.5–29.9). In other words, the magnitude of BMI to define overweight/obesity was higher in Western than in Asian studies. Considering that the relationship between obesity and mental disorders is stronger among those with more severe obesity (423), the use of a relatively low BMI value to define overweight/obesity may be the reason the association between overweight/obesity and some mental disorders, including anxiety disorders, is not significant in Asian studies, contrary to the findings of Western studies.
There could be an argument that the revised criteria for the Asia-Pacific population has been suggested due not simply to left-shifted BMI distribution in Asian populations but also to biological reasons, such as body fat percentage and effect on metabolic disorders, so the negative finding in this study may not be related to low BMI cutoff value. We agree with the view that biological factors can partly contribute to the development or aggravation of a kind of mental disorders. However, the etiologies of most psychiatric disorders are based on the bio-psychosocial model in which not only biological factors but also psychosocial factors—often more importantly—contribute to the development of the disorders. Most of us would accept that social prejudice against obesity and low self-esteem in obese people are more strongly associated with body shape and appearance than with invisible body fat composition, and the former is more sensitively represented in absolute BMI score than revised Asian Pacific BMI criteria. Although people tend to compare themselves with the same race in the same country, most Korean people would not discriminate against a 175 cm tall man weighing 76.6 kg (BMI = 25) due to his appearance while the situation would be different for a man of the same height weighing 91.8 kg (BMI = 30). In some studies, obesity was defined as a BMI at or above the 95th percentile for age and sex, and overweight was defined as a BMI between the 85th and 94th percentiles using national standards derived from the National Institutes of Health and the WHO (25). If we used the same methodology in the current study sample, a BMI at the 85th percentile (cutoff value for overweight) would be 26.0, and a BMI at the 95th percentile (cutoff value for obesity) would be 28.4, showing that using a cutoff of 25 to define obesity is still too low in a Korean population. Thus, we used original WHO criteria instead of revised Asian-Pacific criteria for the analysis of the association between overweight/obesity and mental disorders.
We could not find any significant association between overweight and alcohol use disorders, a finding in agreement with the results of previous studies (410), although one study found a negative relationship between overweight and alcohol use disorders among men (29). This finding may warrant further research.
Overweight was not significantly associated with nicotine use disorders. However, subgroup analyses found a significant interaction with age, and overweight was associated with a decrease in nicotine use disorders in older men but an increase in nicotine use disorders in younger women. The association of smoking with body weight is complicated by current smoking status. It has been reported that current smokers were less likely to be obese than never smokers while former smokers were more likely to be obese than both current smokers and never smokers (30). In this study, we considered persons with lifetime nicotine use disorder, which is a heterogeneous group of current and former smokers, so it is difficult to interpret the results. However, the high proportion of current smokers in persons with lifetime nicotine use disorder (80.3%) in the current sample suggests that the negative association between overweight and nicotine use disorders in older men is consistent with epidemiological findings that current smokers have a lower BMI than do nonsmokers, and body leanness increases with the duration of smoking (30). Nicotine is known to suppress appetite in animals (31) and to impair glucose tolerance and insulin sensitivity (32). The absence of a significant association in older women may be due to the lack of statistical power (because fewer women have nicotine dependence). However, in spite of the small number of women with nicotine dependence, an increased association between overweight and nicotine use disorders was observed in young women. Higher pressure to lose weight makes women present for treatment of obesity more often than men (33), and unfortunately, many women start or continue smoking as a means to control their weight (34) despite the fact that smoking is a well-known risk factor for various cancers and cardiovascular diseases. The reason only young women showed an increased association between overweight and nicotine use disorders may be the stronger stigma for obesity and greater body dissatisfaction in this population (1425). Thus, policy makers and clinicians should pay more attention to preventing, identifying, and treating nicotine use disorders in overweight young women.
Overweight was associated with an increase in the lifetime prevalence of suicidality with ORs around 1.4. Although the strength of the associations is modest, they are very important for public health, considering the high prevalence of overweight (about 22%) in the Korean population and the fact that Korea has the highest suicide rate among the OECD member states (35). The association between overweight and suicidal tendency was more prominent with larger ORs among the younger population. This finding shows that more attention and effort are critical for the prevention of suicide among overweight young individuals. It is noteworthy that the association between overweight and suicidality was not limited to women, contrary to the association between overweight and depressive disorders. Generally, it is well known that men have a higher prevalence of suicide mortality than women (35), although the prevalence of depressive disorder is usually higher in women than in men. In addition, the findings that obesity has a negative effect on employment (36) and that the impact of economic crises on suicide rates is greater among men (37) suggest that obese men are very susceptible to suicidal risk in the environment of increasing unemployment in Korea (38).
Several limitations of this study must be acknowledged. First, height and weight data were self-reported. Although self-reported height and weight have been shown to be strongly correlated with measured values (39), individuals tend to overestimate height and underestimate weight; this leads to underestimation of BMI (40). Second, the cross-sectional study design does not allow us to determine the direction of causal relationships between overweight and psychiatric disorders or suicidality. A meta-analysis of longitudinal studies confirmed a reciprocal relationship between obesity and depression (5). However, for other psychiatric disorders and suicidality, further exploration is needed to confirm the causal relationship with overweight. Third, in this study, we used current BMI and lifetime psychiatric disorders, so the discrepancy in the time frame could have influenced the significance of the results. However, as noted by Simon et al., (6) assessment of lifetime diagnosis is preferable because an association between weight and psychiatric disorder would be expected to reflect long-term behavioral and/or biological mechanisms. Fourth, several pieces of demographic and clinical information including medical conditions and socio-economic status, which can confound the association between overweight and psychiatric disorders, were not considered in the analysis due to lack of data. Finally, we should be cautious in generalizing the current findings to other countries or ethnicities. The BMI distribution of the Korean population is shifted to the left compared to those of Western countries while the prevalence of suicide is much higher than in most other countries. The differences in prevalences of obesity, psychiatric disorders, and suicidality may influence the significance of the associations among these variables.
Notwithstanding these limitations, the findings of this study may provide valuable data for policy makers to implement health-related plans and for clinicians to evaluate and manage overweight patients.
In sum, we found that overweight was associated with an increase in depressive disorders and suicide tendencies in a representative sample of Korea. Sociodemographic factors like gender and age influenced the association, and especially young women showed an increased association of overweight with depressive disorders and with nicotine use disorders. Young individuals showed an increased association between overweight and suicidal tendencies. These findings demonstrate that substantial psychological burden is caused by overweight in Korea as in Western countries and suggest that the norms for an ideal body image and stigma against obesity may not be very different from those of Western cultures, especially in younger generations. Considering the paucity of data regarding the Asian population, further research on this issue may be warranted.
 XML Download
XML Download