

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The prevalence of prostatitis is 8.2% (range 2.2%–9.7%) and the National Institutes of Health (NIH) classified prostatitis into four categories: acute bacterial, chronic bacterial, chronic prostatitis/chronic pelvic pain syndrome, and asymptomatic (1). Acute bacterial prostatitis (ABP) is a rare disease accounting for only 5% of prostatitis cases (2). However, ABP requires immediate treatment because it can lead to complications such as urosepsis (3). Inadequate antibiotic use leads to treatment failure and can increase mortality (4). In patients with ABP, fluoroquinolones are commonly used as first empirical antibiotics because of the broad action spectrum, good bioavailability, and high concentrations in the prostatic tissue (5).
Unfortunately, antibiotic resistance in urinary tract infections (UTIs) has increased globally (6). For example, the rate of ciprofloxacin resistance in the United States increased from 3% in 2000 to 17.1% in 2010 (6). In Korea, the use of fluoroquinolones has also been increasing, and consumption doubled during 2001–2012 (7). With these trends, the incidence of ciprofloxacin-resistant microbes increased from 15.2% in 2002 to 22.5% in 2012 in patients with community-onset acute pyelonephritis (8). Based on a recent study, fluoroquinolones were not recommended as a first empirical antibiotic for complicated UTIs in the Asia-Pacific region due to the high rates of quinolone resistance (> 20%) (9). In addition, the increasing extended-spectrum beta-lactamase (ESBL) producing microbes have become a major concern. Generally, ESBL-producing organisms are also resistant to quinolones, aminoglycosides, and trimethoprim-sulfamethoxazole (10). In the 2010 Korean Antimicrobial Resistance Monitoring System report, the incidence of ESBL-producing Escherichia coli and Klebsiella pneumoniae in community-acquired infections was 9.5% and 12.8% and the incidence in hospital-acquired infections was 25% and 78.6%, respectively (11). Therefore, it is important to identify factors associated with antimicrobial resistance in order to choose an appropriate empiric antibiotic in patients with UTIs. Risk factors for ciprofloxacin resistance in E. coli have been reported in previous studies and include advanced age, male gender, diabetes mellitus, urinary tract abnormalities, recurrent UTIs, previous therapy with quinolones, urinary catheterization, and presence of complicated UTIs (12131415).
In patients with UTIs, the treatment depends on the sensitivity of the microbes to the concentrations of the antibiotics in the urine rather than in the blood (16). This suggests that it is important to examine the clinical impact of antimicrobial resistance on treatment outcomes in UTIs. In this study, we describe the etiologic pathogens and risk factors for ciprofloxacin-resistant E. coli and ESBL-producing microbes, susceptibility to ciprofloxacin, and the incidence of ESBL in patients with ABP. The results of this study provide useful information for prescribing appropriate antibiotics and better ABP management, particularly for its association with increased incidence in patients that previously underwent urologic manipulation.
MATERIALS AND METHODS
Medical records of patients with ABP were retrospectively reviewed to determine risk factors for and the incidence of ciprofloxacin-resistant and ESBL in pathogens. We included patients who were diagnosed with acute prostatitis at the Kyung Hee University Hospital at Gangdong from January 2006 to December 2015. Acute prostatitis was diagnosed by a body temperature > 38°C, painful prostate on digital rectal examination, and leukocytes in urine sediments (17).
We investigated the known factors associated with ciprofloxacin-resistant E.coli or ESBL-producing microbes such as age greater than 60 years, history of prior urologic manipulation, hospital-acquired infection, history of operation in the preceding 180 days, diabetes mellitus, hypertension, antibiotic exposure during the preceding 90 days, history of UTI, prostate volume over 40 mL, and alpha-blocker medication. We classified patients into two groups based on patient records. Patients who had undergone prior urologic manipulation such as urethral catheterization, transrectal prostate biopsy, urodynamic study, or urethral dilation were defined as the manipulation group. Patients who did not experience urologic procedures were defined as the non-manipulation group. Standard blood biochemistry, urine examination by the dipstick method, and urinary sediment were performed for all patients. The identification and antimicrobial susceptibility of isolates were confirmed with the Vitek 2 system (bioMérieux, Marcy L′Ètoile, France) or disk diffusion susceptibility tests.
Data was analyzed using SPSS, version 18.0. Proportion comparisons for categorical variables were performed using χ2 tests. P value and odds ratio were calculated for risk factors. A P value of < 0.05 was considered statistically significant. In addition, multivariate model analysis was performed to determine independent risk factors for ciprofloxacin resistance and ESBL-producing microbes. The resistance to ciprofloxacin and ESBL-producing microbes were the dependent variables in binary logistic regression.
RESULTS
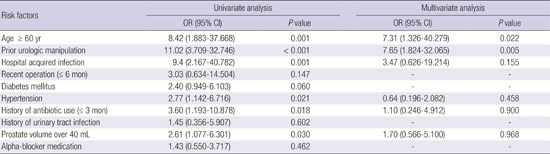
ABP was diagnosed in 307 patients over the entire time period. Of those, 123/307 patients (40.1%) had positive urine cultures and their bacterial strains were identified, and 26/123 patients (21.1%) showed ciprofloxacin resistance. ESBL-producing microbes were found in 10 patients: 7 were associated with E. coli and 3 were associated with K. pneumoniae (Table 1). The distribution of ciprofloxacin-resistant and ESBL-producing microbes in relation with risk factors is shown in Table 2. In univariate analysis, age greater than 60 years (P = 0.001), history of prior urologic manipulation (P < 0.001), hospital acquired infection (P = 0.001), hypertension (P = 0.021), previous antibiotic use (P = 0.018), and prostate volume over 40 mL (P = 0.030) were found to be significant factors associated with ciprofloxacin resistance in E. coli infections. In multivariate analysis, age greater than 60 years (Odds ratio [OR], 7.31; confidence interval [CI], 1.326–40.279; P = 0.022) and history of prior urologic manipulation (OR, 7.65; CI, 1.824–32.065; P = 0.005) were associated with ciprofloxacin resistance in E. coli strains infections (Table 3). In addition, prior urologic manipulation (P < 0.001), history of recent operation (P = 0.030), and hypertension (P = 0.031) were risk factors for ESBL-producing microbes in univariate analysis. In multivariate analysis, presence of urologic manipulation (OR, 13.640; CI, 2.159–86.167; P = 0.005) was found to be associated with ESBL-producing microbes (Table 4).
Table 1
Urine culture results in patients with ABP (n = 123)
Table 2
Antibiotic resistant and ESBL-producing microbes and risk factor associations (n = 123)

Table 3
Univariate and multivariate analysis of ciprofloxacin-resistant microbes
Table 4
Univariate and multivariate analysis of ESBL-producing microbes
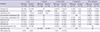
The non-manipulation group consisted of 104/123 (84.6%) patients and the manipulation group consisted of 19/123 (15.4%) patients; 12 had urethral catheterization (63.2%), 5 (26.2%) had transrectal prostate biopsy, 1 had urethral dilation (5.3%), and 1 had a urodynamic study (5.3%). Significant differences of microbial spectrum between two groups were observed. The most frequent microbe was E. coli (67.3% in the manipulation group vs. 52.6% in the non-manipulation group), followed by E. faecalis (19.2% vs. 10.5%), K. pneumoniae (4.8% vs. 31.6%), and Pseudomonas aeruginosa (2.9% vs. 0%). K. pneumoniae counted for a far higher proportion in the prior manipulation group than in the non-manipulation group. The antimicrobial susceptibility profiles are displayed in Table 5. The incidence of E. coli that was susceptible to ciprofloxacin was 60/70 (85.7%) in the non-manipulation group and 1/10 (10.0%) in the manipulation group. Susceptibility to amikacin, imipenem, and piperacillin/tazobactam showed a high sensitivity in both groups. The antimicrobial susceptibilities of E. coli in the non-manipulation group compared to the manipulation groups were as follows: amikacin, 100% vs. 100%; ampicillin, 57.1% vs. 0%; 2nd generation cephalosporin, 100% vs. 80.0%; 3rd generation cephalosporin, 97.1% vs. 60.0%; gentamicin 85.7% vs. 70.0%; imipenem, 100% vs. 100%; and TMP/SMX, 78.6% vs. 50.0%. ESBL-producing microbes were found in 10 patients (8.1%); 7 were E. coli (5.7%) and 3 were K. pneumoniae (2.4%). All ESBL-producing pathogens were resistant to quinolone.
Table 5
Antibiotic susceptibility of pathogens isolated from patients with ABP (n = 123)
DISCUSSION
ABP is a serious condition that can cause septicemia and urosepsis and is characterized by common symptoms including dysuria, lower urinary tract symptoms, urinary retention, fever, and malaise (18). In terms of microbiological characteristics, E. coli is the most prevalent pathogen occurring in 67% of cases, with P. aeruginosa in 13%, Klebsiella spp. in 6%, Gram-positive species in 5% and others in 9% (19). Several studies reported the different distribution of pathogen according to the prior manipulation. In the manipulation group, relatively fewer E. coli were detected. Regarding Pseudomonas spp. were counted for higher proportion in the manipulation group (2021). In our study, relatively fewer E. coli was detected in the group with prior manipulation and K. pneumoniae was significantly higher in the manipulation group compared with the non-manipulation group.
Previous studies reported that the progression of chronic bacterial prostatitis and inflammatory chronic pelvic pain syndrome was 1.3% and 10.5% after ABP treatment (22). Therefore, appropriate therapeutic strategies for ABP are important for adequate treatment and prevention of progression to chronic infection. Fluoroquinolones are commonly used as first empirical antibiotics, however, recently, the increased use of fluoroquinolone has been associated with increased resistance (8). Additionally, to-date, only a limited number of studies have reported risk factors for ciprofloxacin-resistant E. coli. They concluded that advanced age, male gender, diabetes mellitus, urinary tract abnormalities, recurrent UTIs, previous therapy with quinolones, urinary catheterization, and presence of complicated UTIs were risk factors for ciprofloxacin-resistance among uropathogens (12131415). However, our study showed different results compared with previous studies. This study showed that presence of prior urologic manipulation, age greater than 60 years, hospital-acquired infection, hypertension, history of prior use of antibiotics, and prostate size over 40 mL were found to be risk factors for the developing ciprofloxacin resistance in univariate analysis. Multivariate analysis indicated that age and history of prior manipulation were independent risk factors that contributed to ciprofloxacin resistance. In addition, prior urologic manipulation, history of recent operation, and hypertension were associated with ESBL-producing microbes in univariate analysis. In multivariate analysis, presence of urologic manipulation was found to be associated with ESBL-producing microbes.
It is well known that quinolone resistance impairs the capacity of E. coli to invade local tissue of the prostate and kidney (2324). Some studies have reported that exposure to quinolone antibiotics results in the reduced production of certain factors that contribute to the virulence of bacteria (25). Indeed, quinolone resistant E. coli was less likely to produce invasive UTI such as pyelonephritis and prostatitis than is quinolone sensitive E. coli. They suggested that the physical disruption of mucosae and host factor alterations associated with urologic manipulation may increase invasiveness of quinolone resistant E. coli. Increased age may reflect the presence of age-related incontinence or other minor urologic abnormalities that are not considered to be structural abnormalities (26). Age-associated changes in immune function, exposure to nosocomial pathogens and an increasing number of comorbidities increased risk for developing infection (27).
This analysis confirmed a high rate of ciprofloxacin resistance in ABP. Overall, the susceptibility to ciprofloxacin of E. coli was 76.3%. This is similar to reported antibiotic resistance in previous study on patients with acute pyelonephritis (8). This warrants caution in selecting empiric treatment for ABP. In this study, each group showed different results, and we found that 85.7% of susceptibility was identified in the non-manipulation group, whereas the manipulation group showed 10.0% susceptibility. In addition to fluoroquinolone resistant E. coli, we examined ESBL-producing microbes. As mentioned earlier, the incidence of ESBL-producing E. coli and K. pneumoniae in community-acquired infections was 9.5% and 12.8% and in hospital-acquired infections the incidence was 25% and 78.6%, respectively (11). In this study, the incidence of ESBL-producing E. coli was 2.9% in the non-manipulation group and 21.1% in the manipulation group, respectively. In regards to K. pneumoniae, the incidence was 1.0% in the non-manipulation group and 10.5% in the manipulation group. The ESBL frequency was low compared with the results of a previous study because it was conducted by tertiary care centers (11). All ESBL-producing microbes showed fluoroquinolone resistance by cotransferring of quinolone resistance and ESBL genes (28). For these patients, intravenous carbapenems are recommended as first antibiotic treatments (29).
Recent guideline for treatment of ABP recommended the administration of a quinolone or cephalosporins alone or in combination with an aminoglycoside (30). However, our results showed that fluoroquinolones as a first empirical antibiotic may have limited effects in patients with prior urologic manipulation. In addition, incidence of ESBL was significantly higher in the group with prior manipulation. With this regard, cephalosporins with amikacin, or carbapenems, or extended-spectrum penicillin with beta lactamase inhibitor should be considered as the preferred empirical ABP treatment in the patients with history of prior urologic manipulation.
There were some limitations to this study, which included the small sample size and retrospective nature. Therefore, we verified the diagnosis of ABP with the patient’s final diagnosis in the medical records. In addition, patients with mild ABP cases with minimal fever may not have been included, which could have caused selection bias. Another limitation is that the data for previous antibiotic use before hospital visits might be underestimated, which could cause a higher culture negative rate. In this study, we found that only 16 patients had recorded use of antibiotics before hospital visit, and of these patients, 10 patients used fluoroquinolones. Therefore, the association between ciprofloxacin resistance and previous antibiotic use could be inaccurate. In order to overcome these limitations, a future prospective study with larger numbers of cases is necessary.
In conclusion, this study showed microbiological aspects of ABP in Korea. This may inform selection of appropriate empirical antibiotics. The results indicated that ABP with history of prior manipulation was associated with high resistance to fluoroquinolones and a high incidence of ESBL-producing bacteria. Therefore, initial treatments approaches for ABP should consider patients’ age and whether the patient have undergone prior urologic manipulation.
 XML Download
XML Download