

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Subepithelial tumors (SETs) of the gastrointestinal (GI) tract are sometimes encountered during routine esophagogastroduodenoscopy. It is essential to biopsy these lesions because there is always the possibility that some of it has malignant potential. Biopsy is especially important to differentiate GI stromal tumors (GISTs) from other tumors. Although endoscopic ultrasonography (EUS) is the best imaging modality for the evaluation of various SETs, pathological diagnosis is still necessary for an accurate diagnosis.
There are several potential techniques for making a tissue diagnosis, including EUS-guided fine-needle aspiration (EUS-FNA) biopsy, EUS-guided trucut biopsy (EUS-TCB), and stacked biopsy. However, these techniques have limited diagnostic efficacy. Although EUS-FNA is currently considered the standard diagnostic technique for GI SETs, its diagnostic yield varies in the literature between 38% and 82% (123). The diagnostic yields of EUS-TCB are reported to be similar to those of EUS-FNA because of the high rate of technical failure of TCB (45). In contrast, stacked “bite-on-bite” forceps biopsy has a lower diagnostic yield than do EUS-TCB and EUS-FNA (roughly 17% to 38%) (67). Endoscopic resection by snaring and submucosal dissection provides both pathological diagnosis and treatment for the tumor. However, this procedure can be technically difficult and demands a long procedure time, with a risk of perforation (8910111213). SET ligation with bands and loops has been proposed to reduce the risk of perforation during endoscopic removal. However, ligating these lesions is also technically demanding and does not provide an en bloc specimen for surgical pathology and margin evaluation (1415161718). Ultimately, it is not necessary to remove the entire lesion through endoscopic resection for diagnostic purposes alone.
The goal of this study was to evaluate the diagnostic yield and safety of forceps biopsies after small endoscopic submucosal dissection (SESD biopsies) in the diagnosis of gastric SETs and compare it with EUS-FNA.
MATERIALS AND METHODS
This was a study conducted at a tertiary referral center in Korea (Kangbuk Samsung Hospital). Patients who underwent SESD biopsies were prospectively enrolled between May 2013 and October 2014 if they had intramural gastric SETs > 10 mm on EUS. Exclusion criteria included age < 18 years, thrombocytopenia (platelet count < 100,000 cells/μL), and lesions with typical sonographic features of a lipoma, varix, or cyst. Patients were also excluded if they had EUS features suggestive of a malignancy. Such features included tumors > 30 mm in diameter and those with heterogeneous echo, cystic spaces, hyperechogenic foci, irregular margins, or adjacent malignant-appearing lymph nodes. These patients were recommended to have surgery for removal of a SET (19). Antithrombotic agents were stopped five days prior to the procedure, and were restarted on the day after.
To compare SESD biopsies with EUS-FNA, we used the retrospective data of 30 EUS-FNA cases which was performed for the diagnosis of gastric SETs between April 2012 and February 2014 in the two centers (Kangbuk Samsung Hospital and Samsung Medical Center).
SESD biopsies were performed by two experienced endoscopists (J.H.P. and Y.S.J.), with patients under conscious sedation. SETs were initially characterized with a radial scanning echoendoscope (GF UE260 & UM-3R Miniprobe; Olympus, Tokyo, Japan). EUS was used to measure SET size by the maximum cross-section of the lesion. If EUS confirmed that the intramural SETs were > 10 mm, then SESD biopsies was performed immediately after EUS by the same endoscopist who perform EUS. Therefore, SESD biopsies required only one anesthesia and only needed to change out endoscopes (echoendoscope to conventional endoscope).
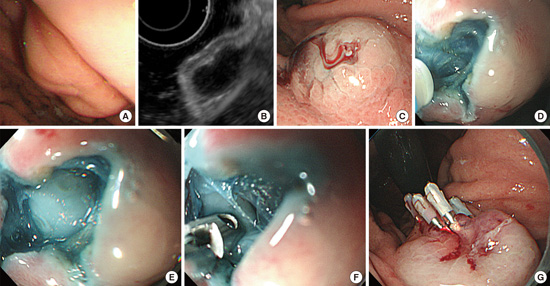
The process of SESD biopsies is shown in Fig. 1. A transparent cap (Distal Attachment [D-201-11304]; Olympus) was fitted to the endoscope tip (GIF-H260; Olympus). A TeleMed disposable sclerotherapy needle (TeleMed Systems, Inc., Hudson, MA, USA) was used to inject SETs with a mixed solution of normal saline + 0.016% indigo carmine + 0.01% epinephrine. A dual knife (Electrosurgical Knife [KD-650L]; Olympus) connected to an electrosurgical unit (ERBE Electromedizin, Tübingen, Germany) was used to incise the lesion using the “Endocut” mode (effect 3, cut duration 2, cut interval 3, and Upmax 550 Vp). A cross-shaped incision and dissection of 6 to 10 mm in size was made under direct endoscopic access over the lesion’s highest convexity zone. A dual knife was used to incise the mucosa and submucosa, and then we confirmed that the underlying tumor was exposed. Conventional biopsy forceps (oval spoon-shaped mouth, without spike [fenestrated, tapered]; MTW, Düsseldorf, Germany) were then introduced deep into the lesion, and 2–7 samples were obtained. Incisions were closed with 2–4 endoclips (Long Clip [HX-610-090L]; Olympus). The biopsy specimens obtained were immediately placed in formalin and were submitted for histopathologic and immunohistochemical examination. When conventional cytologic analysis revealed features of mesenchymal origin, further differentiation into GIST and non-GIST was performed by immunohistochemical analysis of CD117 (c-kit), CD34, smooth muscle actin, and S-100 markers.
Fig. 1
Forceps biopsy technique after small submucosal dissection. (A) Endoscopic view of a gastric subepithelial tumor (SET). (B) Endoscopic ultrasonography image of a gastric SET. (C) Submucosal saline injection. (D) Cross-shaped dissection of the mucosa and submucosa with a dual knife. (E) Confirming the exposure of the underlying tumor. (F) Biopsy forceps were introduced through the hole, taking multiple tissue samples from inside. (G) Prophylactic or hemostatic clipping.

All procedures of SESD biopsies were performed on an outpatient basis. The participants were closely monitored and discharged 1–2 hours after the procedure. The patients were contacted 24–48 hours after the procedure to assess any adverse events. The participants also returned to the hospital within 2–4 weeks of their endoscopy to be evaluated for post-procedural adverse events.
EUS-FNA was also performed by three experienced endoscopists. EUS-FNA was performed by using a linear echoendoscope (GF-UCT 260; Olympus) with a 19 or 22 gauge (EUSN3 EchoTip; Wilson-Cook Medical Inc., Winston-Salem, NC, USA) according to standard techniques, under real-time US guidance and color/pulsed Doppler control. Three to 5 (mean 3.3) passes were performed for each lesion. The patients who underwent EUS-FAN were hospitalized and carefully monitored for 24 hours after the EUS-FNA.
The software program SPSS Version 18 (SPSS, Inc., Chicago, IL, USA) was used for statistical analyses. Student’s t-test was used to compare numerical variables between the two groups and the χ2 or the Fisher’s exact test was used to compare categorical variables.
Ethics statement
The study protocol was approved by the institutional review board of Kangbuk Samsung Hospital (IRB No. KBC13042). All patients who agreed to participate in the study signed a written informed consent form. This study has been registered with the Clinical Research Information Service (CRIS), Republic of Korea (Clinical trial registration No. KCT0000730).
RESULTS
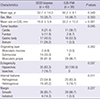
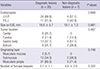
SESD biopsies, as described, was attempted in 42 patients (mean age 53 years) and EUS-FNA was performed in 30 patients (mean age 50 years). Table 1 summarizes the demographic characteristics of patients and endoscopic characteristics of the gastric SETs. The average lesion size measured with EUS in SESD biopsies group was smaller than that in EUS-FNA group (mean 18.8 ± 5.9 mm vs. 32.2 ± 12.0 mm, P < 0.001). The SET locations in SESD biopsies group included: cardia (n = 9, 21.4%), fundus (n = 5, 11.9%), gastric body (n = 17, 40.5%), and antrum (n = 11, 26.2%). The SET locations in EUS-FNA group included: cardia (n = 11, 36.7%), fundus (n = 2, 6.7%), gastric body (n = 16, 53.3%), and antrum (n = 1, 3.3%). In SESD biopsies group, 2 patients (4.8%) had lesions that arose from the muscularis mucosa, 14 (33.3%) from the submucosa, and 26 (61.9%) from the muscularis propria, whereas in EUS-FNA group, only one patient (3.3%) had lesion that arose from the muscularis mucosa and all the other (96.7%) from the muscularis propria (P = 0.002). Hypoechoic and homogenous lesions were more frequent in EUS-FNA group than in SESD biopsies group.
Table 1
Demographic characteristics of patients and endoscopic characteristics of subepithelial lesions
The diagnostic yield of SESD biopsies was comparable to that of EUS-FNA (35 of 42, 83.3% vs. 24 of 30, 80.0%, P = 0.717) (Table 2). In addition, the diagnostic yield of SESD biopsies was comparable to that of EUS-FNA among lesions originated from muscularis propria layer (21 of 26, 80.8% vs. 24 of 29, 82.8%, P = 1.000). In SESD biopsies group, the diagnostic lesions included 15 leiomyomas, 7 GISTs, 10 heterotopic pancreases, 2 lipomas, and one other lesion. The other lesion was an 18-mm isoechoic, heterogeneous mass that originated from the submucosal layer. Pathological analysis of this lesion revealed tiny pieces of fibrovascular tissue with mucinous material suggestive of mucin containing benign lesions or mucinous adenocarcinoma. Given the possibility of mucinous adenocarcinoma in this case, ESD was performed. ESD confirmed the pathological diagnosis of mucinous adenocarcinoma with invasion into the submucosa (SM 3). The deep resection margin of the ESD specimen also had carcinomatous tissue. Therefore, the patient underwent a gastrectomy. In EUS-FNA group, the diagnostic lesions included 11 leiomyomas, 14 GISTs, and 1 neuroendocrine tumor.
Table 2
Outcomes of SESD biopsies group versus EUS-FUA group
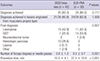
The mean numbers of forceps biopsies in SESD biopsies group was 3.9 and needle passes in EUS-FNA group were 3.3 (P = 0.021). The mean procedure time of SESD biopsies was shorter than that of EUS-FNA (10 vs. 37 minutes, P < 0.001). In SESD biopsies group, all incisions were closed with clips. In some cases, there was a small amount of bleeding from the cut surface immediately after incision of the overlying mucosa and submucosa or from the tumor surface after biopsy. The bleeding was controlled by clipping. There were no procedure-related adverse events including perforation or massive bleeding in both groups.
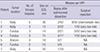
The results of seven GIST cases in SESD biopsies group are shown in Table 3. The forceps biopsy specimens obtained from these cases were not large enough to evaluate the mitotic index in 50 consecutive high power fields (HPFs) (range 5–42 HPFs). Of the seven patients with GIST, four underwent a surgical resection. According to Fletcher’s classification, three of these four patients were classified to be at very low risk for a malignancy and only one patient was at intermediate risk (20).
Table 3
Results of the seven patients with GIST in SESD biopsies group
Among SESD biopsies group, there was no significant difference in the diagnostic yield between the endoscopists. In addition, there were no significant differences between the diagnostic and nondiagnostic cases with regard to SET size, location, originating layer, and the number of forceps biopsies obtained (Table 4).
Table 4
Comparison between diagnostic and non-diagnostic lesions in SESD biopsies group
DISCUSSION
It is important to differentiate the various types of SETs because these lesions have different prognoses and require different management or therapeutic options. EUS findings alone have limited specificity for the diverse subtypes of SETs and fail to distinguish between benign and malignant lesions. Our study demonstrated that the diagnostic yield of SESD biopsies was comparable to that of EUS-FNA (83% vs. 80%).
Currently, there is no consensus regarding the optimal management strategy for small (< 3 cm in diameter) asymptomatic SETs. Therefore, endosonographic clinical practice patterns in surveillance and management are highly variable. A recent update in the National Comprehensive Cancer Network Guidelines on the management of GISTs recommended that incidentally encountered small GISTs (< 2 cm in diameter) be followed endoscopically until they grow or become symptomatic (21). Another study reported that GIST lesions (diagnosed by EUS) that are < 3 cm in size with low malignant potential can be observed with EUS rather than cytohistologically diagnosed or removed (19). However, current literature suggests that all GIST lesions have malignant potential, even those just 1 cm in size (22). Therefore, optimal pathologic examination of tumor tissue is mandatory, especially for lesions that are hypoechoic, located in the muscularis propria of the stomach, or are > 2 cm.
Several diagnostic methods have been proposed for the tissue diagnosis of GI SETs. EUS-FNA is currently considered the standard method for GI SETs samples; however, it has limited value for the cytologic diagnosis of nonmesenchymal lesions (with nondiagnostic samples up to 100%) (3). In addition, EUS-FNA has a high failure rate in immunostaining with regard to mesenchymal tumors; this limitation decreases its diagnostic yield from 70%–74% to 34%–53% after immunohistochemical analysis (34). Unfortunately, immunohistochemical analysis is not always feasible with EUS-FNA samples because there is insufficient material obtained by aspiration. EUS-TCB emerged as a method to solve the limitations of EUS-FNA. Theoretically, this procedure provides core-tissue specimens that would increase the diagnostic yield with thicker samples. Despite this prediction, the diagnostic yield of TCB in GI SETs is not superior to that of EUS-FNA (47%–63%) (4523). There is a high rate of technical failure with TCB because the device is very stiff, which hinders the needle from obtaining tissue (24). In addition, there are safety concerns regarding TCB. A previous study reported that among 52 TCB procedures performed for gastric SETs, there were two cases of sepsis (5).
This study presents several reasons why SESD biopsies may be preferable to EUS-FNA or EUS-TCB. First, SESD biopsies provide a high diagnostic yield. Although its diagnostic yield was compared to the retrospective data of EUS-FNA cases, our results show that its diagnostic yield is not inferior to that of EUS-FNA. Second, SESD biopsies also provide sufficient tissue for accurate diagnosis in a cost-effective manner, while avoiding unnecessary follow-up examinations or repeated exploratory surgeries. According to our data, the pathological diagnoses of 35 included 7 GISTs, 15 leiomyomata, and 10 heterotopic pancreases. Since GISTs have malignant potential, they necessitate lifelong follow-up or resection. Patients who were diagnosed with benign lesions such as a leiomyoma or heterotopic pancreas do not require annual EUS examinations or surgical resection. Third, another advantage to SESD biopsies is that it can be easily performed regardless of the lesion’s anatomic location. In contrast, EUS-FNA and EUS-TCB have high failure rates with regard to tissue acquisition when the SET lesion is in the cardia or fundus because the stiff device has difficulty accessing these areas. The diagnostic yield of SESD biopsies is high, even when SETs are in the cardia or fundus (13 of 14, 93%). Fourth, SESD biopsies can be easily performed regardless of the lesion’s size. Our results showed that the average lesion size in SESD biopsies group was smaller than that in EUS-FNA group (19 vs. 32 mm). EUS-FNA has difficulty in needle passing and aspiration of small sized SETs. Fifth, SESD biopsy is a safe procedure. There were no procedure-related adverse events in this study including perforation, bleeding, or sepsis. Finally, the procedure time of SESD biopsies was shorter than that of EUS-FNA (10 vs. 39 minutes) and thus it can save time.
Similarly to EUS-FNA and EUS-TCB, the main limitation of the SESD biopsies is that it does not provide sufficient tissue (with at least 50 HPFs) to evaluate the malignant potential of GISTs. If more forceps biopsies are performed, it is possible to obtain 50 consecutive HPFs in order to evaluate the mitotic index. However, biopsy-obtained tissue is unlikely to represent the mitotic activity of the entire tumor. The mitotic index measured over 50 HPFs may actually be inaccurate because of the heterogeneous distribution of mitotic activity. In addition, the mitotic index should be measured from the most mitotically active area.
Another group recently developed US-guided single-incision with needle knife (SINK) and deep forceps biopsy for the histologic diagnosis of upper GI SETs (25). They found that the diagnostic yield of the SINK biopsy was 92.8% (13 of 14). Of eight GIST cases, the SINK specimens were sufficient for immunohistochemical analysis in seven cases and for measurement of the mitotic index in five cases. The diagnostic yield of our method was not superior to that of the SINK biopsy (83.3% vs. 92.8%). However, our study included a larger number of patients than did the SINK biopsy study (42 vs.14 cases). In addition, our study was prospective, while the SINK study was retrospective. Our methods involved a cross-shaped dissection of mucosa and submucosa, exposure of the underlying tumor, and then tissue extraction through the forceps biopsy. In contrast, the SINK biopsy involves a linear incision without confirming the exposure of the underlying tumor. Although SINK specimens allowed the evaluation of the mitotic index in some of GIST cases, this index may not represent the entire tumor, as described previously. More similar to our study, Lee et al. (26) performed endoscopic biopsy of nine gastric SETs using the ESD technique. Their procedure involved making a 5-mm-diameter hole with a flex knife and then a 15-mm-diameter round incision. Next, they used an IT2 knife to make a submucosal dissection and performed multiple endoscopic biopsies. This technique is somewhat inconvenient because it employs both a flex knife and an IT2 knife, as opposed to our method, which only required a dual knife. Their study population was also very small.
Recently, several diagnostic methods using the unroofing technique have been proposed to obtain a sufficient amount of GI SET tissue. These techniques include partial resection (27), retract-ligate-unroof-biopsy with loop (17), and suck-ligate-unroof-biopsy by using loop (18). These methods have high diagnostic yields (94%, 81%, and 100%, respectively) and provide sufficient tumor tissue for immunohistochemical analysis and mitotic index calculation. However, incomplete endoscopic resection of a GIST tumor can allow for peritoneal dissemination of disease (11). Furthermore, the retract-ligate-unroof-biopsy and suck-ligate-unroof-biopsy with loop techniques cannot provide an en bloc specimen of the entire tumor or negative margin assessment; therefore, any neoplastic lesion with malignant potential needs close serial follow-up by expensive EUS.
An unexpected finding in our study is that leiomyoma was the most common gastric SET (although non-diagnostic lesions were considered). GIST is known to be the most frequent SET in the stomach, whereas leiomyoma is the most frequent SET in the esophagus (28). In our study, among SESD biopsies group, most SETs (8 of 9) in the cardia were leiomyomas and only one case was heterotopic pancreas. Leiomyoma seems to be frequently found in the upper stomach near the esophagogastric junction. If a SET > 20 mm is incidentally found during routine endoscopy in the cardia of the stomach, there is high probability that it is a leiomyoma. After immunohistochemical confirmation, this lesion would not require surgery.
This study has several limitations. First, the sample size was small and SESD biopsies were performed at a single center by only two endoscopists. It is possible that the operator-related factors influenced our results and that the diagnostic yields may be lower than those in an average practice. Future investigation at multiple centers with more endoscopists is needed to clarify the efficacy of SESD biopsies. Another limitation to this study is that the diagnostic yield of SESD biopsies was compared to the retrospective data of EUS-FNA cases. Finally, SESD biopsies specimens were not large enough to evaluate mitotic index in 50 consecutive HPFs.
This study focused on the acquisition of tissue specimens with SESD biopsies for diagnostic purposes. SESD biopsies was found to be an effective, easy, and safe technique for the histologic diagnosis of gastric SETs and its diagnostic yield is comparable to that of EUS-FNA. It may be a reliable alternative to conventional EUS-FNA and TCB. However, further prospective comparative studies with larger sample sizes are needed to confirm this method’s efficacy.
 XML Download
XML Download