

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Despite advances in healthcare, anemia and iron deficiency (ID) remain the most common disorders in women (123). Globally, the prevalence of anemia increased to 30% in non-pregnant women of reproductive age (15 to 49 yr) (4).
The Korea National Health and Nutrition Examination Survey (KNHANES) was established in 1998 by the Korea Centers for Disease Control and Prevention to evaluate the health and nutritional status of the Korean people. This survey is intended to determine the prevalence of chronic diseases and their risk factors (5). KNHANES IV-2 data (2008) showed that the prevalence of anemia in females was 13% in 15 to 17 yr olds, 17.9% in 18 to 49-yr olds, 10.9% in 60 to 69-yr olds, and 18.2% in women of 70 or older (67). Recently, Lee et al. (8) analyzed KNHANES V-1 (2010) data and found prevalence of 10.1% in 15 to 17-yr olds, 14.7% in 18 to 49-yr olds, 7.7% in 60 to 69-yr olds, and 20.7% in women 70 or older.
Anemia is an independent risk factor of increased morbidity and mortality and of diminished quality of life (910). The main causes of anemia worldwide are; ID, hemoglobinopathy, and malaria. However, in Korea, anemia is caused by ID, because hemoglobinopathy and malaria are extremely rare.
Iron deficiency anemia (IDA) can cause fatigue, reduce work capacity and resistance to infection. Furthermore, IDA has been shown to be correlated with reduced cognitive performance and mental development in children and adolescents (1112); and detrimental findings have even been reported for those with non-anemic ID (13). Too little iron in diet causes anemia and the non-hematologic effects of iron depletion, whereas too much dietary iron initiates excessive free radical activity and causes oxidative injury to cells. The study performed by Lee et al. (8) on KNHANES V-1 (2010) data showed the prevalence of ID in females was 34.7% among 15-17-yr olds and 31.1% among 18-49-yr olds, and that prevalence of IDA was 9.0% among 15-17-yr olds and 11.7% among 18-49-yr olds. In addition, premenopausal status, pregnancy, low income, underweightedness, and iron- or vitamin C-poor diets were found to be associated with IDA.
It is known that the mechanisms of iron absorption are closely related with levels of heavy metals in blood (14). ID is associated with elevated blood levels of divalent heavy metals, such as, cadmium, lead, and manganese (1415161718). In addition, vitamin D deficiency has been shown to be associated with an increased risk of IDA in children and adolescents (1920). However, relationships between IDA, blood heavy metals and vitamin D levels have not been simultaneously examined.
In the present study, we aimed at determining the prevalence of anemia, iron depletion, and IDA in a female population aged 10 yr or older, and to compare how this prevalence has changed over years. In addition, we sought to verify associations between IDA, heavy metals in blood, vitamin D levels, and nutritional intakes by path analysis.
MATERIALS AND METHODS
Design and study population
This study was performed using data obtained during the KNHANES V study (2010 to 2012), a cross-sectional and nationally representative survey conducted on non-institutionalized individuals by the Division of Chronic Disease Surveillance, Korea Centers for Disease Control and Prevention. KNHANES data is obtained from 10,000 individuals randomly chosen from the 192 regions in Korea on an annual basis using a stratified, multistage sampling procedure. KNHANES data is obtained using health interviews, health examinations, and a nutrition survey.
Women who were pregnant, less than 10 yr old, indefinable for anemia, ID or IDA (due to missing data) were excluded from the study, which was performed on 10,169 Korean women, which included 1,232 anemic, 2,030 ID, and 690 IDA subjects. Adolescents were divided into two groups (10 to 14-yr olds and 15 to 18-yr olds), because 98% of girls reach menarche at 15 yr of age (21). We considered subjects aged ≤ 18 yr old as adolescents in accordance with the guidelines issued by the Korea Centers for Disease Control and Prevention and the Korean Society of Pediatrics.
Laboratory measurements and definition
Blood samples were obtained from an antecubital vein after obtaining informed consent and collected in BD Vacutainer tubes containing EDTA for trace element determinations. Serum hemoglobin (Hgb) levels were measured using the sodium lauryl sulfate hemoglobin detection method using a XE-2100D hematology analyzer (Sysmex, Tokyo, Japan). Serum ferritin, a surrogate of dietary iron, has been evaluated since 2007. Iron and total iron binding capacity (TIBC) were added in 2010. Serum ferritin and serum 25 (OH) vitamin D levels were measured using an immunoradiometric assay and a 1470 WIZARD gamma-counter (PerkinElmer, Turku, Finland). Reference materials were used for quality assurance and control (Lyphochek® Whole Blood Metals Control; Bio-Rad, Hercules, CA, USA). Nutritional intakes were determined using Dietary Reference Intakes for Koreans by the Korean Nutrition Society (8).
To assess heavy metals in blood, 3 mL blood samples were drawn into standard evacuated tubes for trace element EDTA (K2 EDTS tube, Vacutainers). Blood cadmium and lead levels were measured by graphite furnace atomic absorption spectrometry (GF-AAS) using the Zeeman background correction (PerkinElmer AAS800, PerkinElmer). Blood cadmium and lead levels were analyzed by the Neodin Medical Institute (a laboratory certified by the Korea Ministry of Health and Welfare). Three commercial reference materials were used for internal quality assurance and control (Lyphochek® Whole Blood Metals Control; Bio-Rad, Hercules, CA, USA). The Neodin Medical Institute had been certified with respect to quality assurance and control by the German External Quality Assessment Scheme operated by Friedrich-Alexander University and the Quality Assurance Program operated by the Korea Occupational Safety and Health Agency. The limits of detection were 0.062, 0.081 and 0.088 µg/L (for blood cadmium), and 0.142, 0.148, and 0.172 µg/dL (for blood lead) in 2010, 2011, and 2012, respectively.
Anemia was defined according to the WHO criteria as: Hgb < 11.5 g/dL at 10-11 yr and < 12 g/dL at ≥ 12 yr. ID was defined as either a serum ferritin level of < 15 µg/mL or a transferrin saturation (TS) value of < 10%. IDA was defined as anemia with ID.
Statistical analysis and model hypotheses
Prevalence and 95% confidence intervals (CI) were estimated using the SAS survey procedures. Weighted results were estimated using survey sample weight variables for associations between health interview, health examination, and nutrition survey. Associations between IDA and clinical factors (such as age, body mass index [BMI] and menstruation status), heavy metals in blood (e.g., blood lead and cadmium levels), vitamin D levels in blood, nutritional intakes (e.g., protein, iron, and calcium intakes), and year were identified using SAS surveyreg procedure (for continuous variables) or surveyfreq procedure (for categorical variables). For blood lead and cadmium levels, values were log transformed due to non-normality. The statistical analysis was performed using SAS version 9.3 (SAS Institute, Cary, NC, USA). Statistical significance was accepted for P < 0.05 (two-tailed).
The maximum likelihood (ML) based structural equation model (SEM) was used to analyze predicted paths between variables in the model. Relationships between IDA, clinical factors, heavy metals in blood, blood vitamin D levels, and nutritional intakes were explored. To measure goodness of fit of the path analysis model, normed fit index (NFI), incremental fit index (IFI), comparative fit index (CFI), and root mean squared error of approximation (RMSEA) were calculated. CFI is the indicator most commonly used to evaluate model fit versus a null model. A value of > 0.90 was considered a good fit. The RMSEA was investigated for lack of fit to avoid problems of sample size when we use chi-square statistics; a RMSEA value of ≤ 0.08 is generally taken to be acceptable. Path analysis was performed using AMOS version 18.0 (SPSS Inc.) software.
The main research hypotheses for path analysis were:
Hypothesis 1. Vitamin D level negatively influences IDA.
Hypothesis 2. IDA is positively associated with divalent heavy metal levels in blood.
RESULTS
The overall prevalence of anemia was 12.4% during the 2-yr study period (2010 to 2012) in Korean women and adolescents, as presented in Table 1. The prevalence was greatest among those aged ≥70 yr (17.8%) and this was followed by 19-49-yr olds (15.0%). The prevalence of anemia in the other age groups was; 2.9% in 10 to 14-yr olds, 11.9% in 15 to 18-yr olds, 7.0% in 50 to 59-yr olds, and 7.8% in 60 to 69-yr olds.
The overall prevalence of ID between 2010 and 2012 was 23.11% (Table 2). The prevalence of ID for 3 yr in 15-18 and 19-49-yr olds was 36.5% and 32.7%, respectively, and for 10 to 14, 50 to 59, 60 to 69, and ≥70-yr olds were 18.2%, 9.4%, 3.8%, and 7.1%, respectively.
The overall prevalence of IDA during the study period was 7.7% (Table 3), and was most prevalent in 15-18 (10.7%) and 19-49 (11.3%)-yr olds. The prevalence of IDA was 2.3% among 10 to 14-yr olds, 3.3% among 50 to 59-yr olds, 1.0% among 60 to 69-yr olds, and 3.2% in ≥70-yr olds. The prevalence of ID was approximately three times greater than that of IDA.
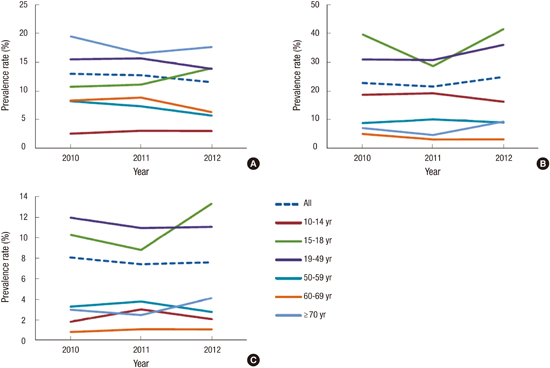
For 15-18-yr olds, the prevalence of anemia, ID, and IDA increased in 2012 as compared with 2010 or 2011, and for 19-49-yr olds the prevalence of ID tended to increase in 2012 as compared with 2010 or 2011 (Fig. 1). Although the prevalence rates of anemia (P=0.322), ID (P=0.086), and IDA (P=0.748) showed slight changes as determined by surveys conducted for 3 yr, there was no statistical significance.
Table 4 shows the distributions of clinical factors stratified by IDA. Subjects with IDA group were younger than those without (P<0.001). Furthermore, menstruation status differed in the IDA and non-IDA groups (P<0.001), and blood cadmium (log-transformed) and vitamin D levels were significantly different in these two groups (P<0.001). However, BMIs, blood lead levels, nutritional intakes, and survey years were no different in these groups at the α=0.05 level.
The theoretical path model based on our hypotheses was tested (Fig. 2). The hypothesis path model fitted data well with NFI, IFI and CFI values of 0.90-0.91 (Table 5).
The model had a RMSEA value of 0.084, indicating model acceptability. Results obtained showed vitamin D level (β=-0.002, SE=0.0004, P<0.001), menstruation (β=0.13, SE=0.007, P< 0.001), age (β=0.001, SE=0.0001, P<0.001), and BMI (β=-0.001, SE=0.001, P=0.036) significantly associated with IDA, but that protein (P=0.261), iron (P=0.233), and calcium intakes (P= 0.325) did not.
Moderately positive correlations were observed between protein, iron and calcium intake (range from 0.44 to 0.52), and significant relationships were found for age, BMI, and menstruation. Path analyses also showed IDA was significantly associated with an elevated blood cadmium level (log-transformed) after adjusting for age and BMI (β=0.48, SE=0.04, P<0.001) (R2=0.54). However, IDA was not associated with blood lead levels (P=0.625).
DISCUSSION
Anemia affects an enormous number of women. In this study, the overall prevalence of anemia, ID and IDA was 12.4%, 23.1%, and 7.7%, respectively. In particular, anemia and ID were more common in late adolescent girls and women of reproductive age. The prevalence of anemia, ID, and IDA did not change appreciably over the period 2010 to 2012, although increases in the prevalence of ID and IDA occurred in females aged 15 to 18 yr. The overall prevalence of iron depletion (defined as serum ferritin level <15 ng/mL) was 23.8% during 2008-2012: 25.5%, 25.8%, 21.6%, 21.1%, and 24.6% in the year of 2008, 2009, 2010, 2011, and 2012, respectively.
The average woman has approximately 40 mg/kg of iron in body stores, which are maintained by the daily absorption of 1-2 mg of iron in the duodenum (22). Adolescence is characterized by the somatic growth spurt and an increased rate of development with commensurate expansion of total blood volume, which requires a greater supply of iron. Adolescents are highly susceptible to nutritional iron deficiency, not only because of their considerably increased nutritional requirements, but also because of poor dietary habits. The observed increase in the prevalence of ID in adolescents is worrisome from the perspectives of possible developmental and learning problems.
In non-pregnant females of reproductive age, the prevalence of anemia in this study was 15.0%, which was not very different from the 17.9% of the 2008 KNHANES data (7), the 12.2% of the Third National Health and Nutrition Examination Survey (NHANES III) (23), the 17.8% of studies conducted in America, and the 19.0% of European studies cited by WHO (4). In the present study, the prevalence of ID was 32.7% in 19 to 49-yr olds, which was similar to the 33.0% found using 2008 KNHANES data. It appears the additional loss of an average of 1 mg iron per day through menstruation tilts balance toward the development of IDA.
Despite of relatively high prevalence of anemia in elderly people (≥70 yr old; 17.8%), the prevalence of IDA was only 3.2%. One third of anemia cases in the elderly are attributable to nutritional (iron, folate, or vitamin B12 deficiency), one third due chronic inflammation or chronic kidney disease, and one-third to some idiopathic cause (2425). However, it should be noted no occult blood testing in stools or gastrointestinal examination was performed during the KNHANES V study. Anemia in the elderly is associated with frailty, increased mortality, poor cognition, and diminished physical performance (262728), and is especially harmful in the presence of heart disease or chronic kidney disease. In view of the rapid increase in the proportion of elderly, it is imperative that an intervention be made available to prevent and treat anemia.
The structural equation model (SEM) is a powerful multivariate analysis technique that was devised to analyze complex relationships among many observed or unobserved variables (29). The SEM enables the validity of empirical models to be tested using variable correlation or covariance matrices. Path analysis (a special type of SEM) has been used to evaluate direct dependencies among a set of observed variables as a form of multivariate regression analyses with focus on causality. In the present study, we examined relationship between IDA, blood cadmium levels, and vitamin D levels simultaneously by path analysis based on the following research hypotheses: Vitamin D negatively influences IDA (hypothesis 1), and the presence of IDA is positively associated with divalent heavy metals in blood (hypothesis 2).
Cadmium is a major environmental pollutant and a carcinogenic heavy metal (1530), and it has been shown cadmium exposure involves diet, particularly, in children and adults not subjected to occupational exposure (18). Blood cadmium concentrations are elevated as cadmium absorption increases through divalent metal transporter 1 (DMT1) in subjects with ID or IDA (31). That is, in those with ID or IDA blood cadmium concentrations are elevated, because such individuals absorb more heavy metals. Moreover, Meltzer et al. (32) showed that blood cadmium levels were associated with reduced serum ferritin levels in women; and in recent investigations of the association between blood cadmium and ID (1415161718), it was found that ID elevates blood cadmium levels in children and adolescents (1518) or adults (141617). Our proposed path model showed that IDA was associated with an increase in blood cadmium levels (log-transformed) in females aged 10 yr or older (β=0.48, SE=0.04, P<0.001). Here we focused on the association between IDA and blood cadmium level (standardized β= 0.16) after adjusting for age and BMI, even though the strength of association between age and blood cadmium level was higher (standardized β=0.71).
Vitamin D has an effect on calcium absorption and bone metabolism, and its deficiency is viewed as a crucial nutritional problem (33). In the present study, blood vitamin D levels were found to have a significant negative effect on IDA in those aged ≥10 yr (β=-0.002, SE=0.0004, P<0.001). Studies have been performed recently on the association between vitamin D deficiency and IDA in children and adolescents (2033), and a significant association was found between vitamin D and IDA, possibly due to the suppressive effect of vitamin D on IDA via hepcidin (an iron-regulatory hormone) (20). Vitamin D supplementation might control IDA by decreasing hepcidin levels. These findings suggest that to prevent ID or IDA, women should consume diet with sufficient available iron and vitamin D to achieve recommended intakes.
Despite progress in nation-wide survey over the past decade, anemia remains a significant public health problem in Korea, which begs the question, 'Why has the prevalence of anemia and IDA not decreased?' The reason may be unbalanced nutrition, food restriction including dieting, public unawareness of anemia prevention, and no or ineffective feedback for anemia and IDA. Furthermore, it appears anemia and IDA are relatively neglected by health care personnel and policymakers. What is more, many clinicians do not consider IDA a real problem, and as a result they often overlook offering preventive nutritional guidance. Even when screening is conducted and ID is identified, appropriate and effective treatment is often overlooked or inadequate (34).
Strong advocacy is required to reduce the incidences of anemia and IDA. IDA is compromises physical and cognitive development and performance, especially in children and adolescents. In addition, IDA in adults contributes to low work productivity and has a negative impact on economy according to the WHO (35). Furthermore, treatment of IDA can improve quality of life and reduce associated morbidity and mortality
According as the 2013 WHO guidelines (35), optimizing nutrition with daily or intermittent (1 to 3 times per week) iron supplementation, should be considered a first-line intervention in high-risk or high-prevalence groups. Although it is probably less effective than daily iron supplementation, intermittent iron appears to be a useful and cost effective way of controlling anemia and IDA (36). Iron fortification with micronutrient powders and fortification of staple foods and condiments may be a useful option if the food concerned is widely consumed by at-risk individuals and if the fortificants do not have toxic effects (36). However, targeted anemia surveillance and intervention should be viewed as a priority in high-risk populations, such as, late adolescents and premenopausal females. On the other hand, anemia is also an important health concern in the elderly. In this population, anemia should be investigated from a different perspective, because it is usually multifactorial in origin.
This is the first study to be conducted on simultaneous associations between IDA and blood cadmium and vitamin D levels in a large population of females aged ≥10 yr. The results also provide that vitamin D level is one of possible determinants of IDA and of elevated blood cadmium level.
However, we acknowledge several limitations of our analysis. Preschool and school age children below 10 yr old were not included, although they are also known to exhibit high prevalence of anemia and iron deficiency. Furthermore, because the acute phase reactants, such as, C-reactive protein, were not included, ID may have been underestimated. In addition, regarding the diagnosis of ID, it would have been better that erythrocyte protoporphyrin (EPP), zinc protoporphyrin, or serum transferrin receptor levels had been measured. Also, since this study was based on the cross-sectional KNHANES study, the results obtained by path analyses did not demonstrate causal relationships between the variables.
In conclusion, this study shows that the prevalence of anemia, ID, and IDA was relatively high in late adolescents and in women of reproductive age. Furthermore, minimal improvements in the burdens of anemia and IDA were observed in the present study from the KNHANES V survey as compared with previous study from the KNHANES IV survey. Path analysis results showed low vitamin D levels enhance the risk of IDA, and that IDA increases cadmium concentrations in blood. Our findings indicate that systematic health surveillance systems including educational campaigns and well-balanced nutrition are needed to control anemia, ID, and IDA.



 XML Download
XML Download