

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Gastric cancer (GC) is one of the most common cancers affecting people worldwide. In the past few decades, the incidence and mortality rates of GC have steadily declined in several countries. However, these rates continue to be high in Asian countries. Particularly, in Korea, GC is the third-most common cancer, with 34,478 new cases and 7,876 deaths recorded in 2014, as per the report of the Korea National Cancer Center (123).
Until date, several studies have reported that genetic alteration including single nucleotide polymorphisms (SNPs) in tumor suppressor genes such as those encoding adenomatous polyposis coli, tumor protein p53, tumor protein p73, deleted in colon cancer, and fragile histidine triad may play an important role in defining susceptibility to GC (45678910111213).
In addition, trefoil factor 1 (TFF1) is a tumor suppressor gene (14) belonging to the TFF family. The TFF protein family consists of TFF1, TFF2, and TFF3, which are expressed and secreted in the mucous cells of the human stomach and protect the gastrointestinal epithelium (151617). TFF are clustered in a 50-kb region of the chromosome 21q22.3 (1819). The abnormal expression levels of TFF proteins have been reported to be associated with the progression and development of several cancers such as colon cancer (2021), breast cancer (2223), prostate cancer (2425), and lung cancer (26). Some evidence suggests that TFF expression is involved in GC progression. TFF1-knockout mice developed antral adenomas, and 30% of them further developed multiple gastric carcinomas (27). TFF1 was normally expressed in gastric mucosa, but the expression of TFF1 and TFF2 was significantly lower in carcinomas than in normal tissues (2829). Both decreased TFF1 and TFF2 expression and increased TFF3 expression have been reported in gastric carcinoma (30). Furthermore, downregulation of TFF1 expression and upregulation of TFF3 expression have also been reported in GC (31). Recently, association studies between polymorphisms of TFF and GC susceptibility were reported in two different ethnic groups: a polymorphism in the promoter region of TFF1 was associated with GC development in an Iranian population, and promoter polymorphisms of TFF2 and TFF3 were associated with GC susceptibility in a Chinese population (3233). Therefore, we hypothesized that the polymorphisms in TFF play a critical role in GC progression and development.
In the present study, we elucidated the relevance of polymorphisms in the coding and promoter regions of the TFF family to the risk of GC and GC subgroups in order to clarify our hypothesis in the Korean population.
MATERIALS AND METHODS
Subjects
This case-control study group included 377 patients with GC (267 men, 110 women) with a mean age of 60.1±11.8 yr and 396 healthy controls (132 men, 264 women) with a mean age of 58.7±9.0 yr. The blood samples used in this study were provided by the Chungnam National Hospital Biobank, which is a member of the National Biobank of Korea and is supported and audited by the Ministry of Health and Welfare of Korea. GC patients were recruited from the outpatient clinic at the Chungnam National University Hospital and classified according to Lauren's classification (34). The healthy controls were randomly selected from among healthy volunteers visiting the Chungnam National University Hospital medical center for their annual physical examinations and who had no history of cancer.
DNA preparation and SNP identification
Genomic DNA was extracted from the peripheral blood by using the QIAamp DNA Blood Mini Kit (Qiagen GmbH, Hilden, Germany) according to the manufacturer's instructions. To identify polymorphic sites in TFF1, TFF2, and TFF3, all exons including intron-exon boundaries, 1.5 kb of the 5'-flanking region, and the 3'-untranslated region (UTR) were amplified by polymerase chain reaction (PCR) with genomic DNA in 24 GC patients and 24 healthy controls. PCR was performed with 50 ng of genomic DNA, Taq DNA polymerase (EF Taq, SolGent, Daejon, Korea), and 0.5 pM of each primer under the following conditions: 30 cycles of denaturation for 10 sec at 98℃, annealing for 30 sec at 65℃, extension for 2 min at 72℃, and a final extension for 10 min at 72℃ in a thermocycler (Gene Amp PCR System 9700; Applied Biosystems, Foster, CA, USA). The PCR product was used as a template for sequencing. The SNPs of TFF1, TFF2, and TFF3 were detected by a sequence analysis based on the reference sequence of human chromosome 21 (GenBank accession number: NT_011512.12).
Genotyping
Genotyping for the SNPs in TFF1 (rs184432, rs35448902, rs225359, and rs2156310), TFF2 (rs3814896, rs13052596, and rs225334), and TFF3 (rs225362) was performed by using the Applied Biosystems TaqMan SNP Genotyping Assay with the StepOnePlus Real-time PCR System (Applied Biosystems).
Statistical analysis
Chi-square tests were used to estimate the Hardy-Weinberg equilibrium (HWE) of each SNP and to detect age and gender in the GC and control groups. The association between the GC and control groups was analyzed by chi-square test. We used binary logistic regression to estimate the GC risk by odds ratios (OR) and 95% confidence intervals (CI). All statistical analyses were performed by using the SPSS (SPSS Inc., Chicago, IL, USA), version 20.0 for windows. P<0.05 was considered statistically significant.
RESULTS
The characteristics of the 377 GC cases and 396 controls are shown in Table 1. No significant difference was noted between GC cases and controls in the distribution of age (P=0.063), whereas the distribution of gender of GC case differed from that of controls (P<0.001). Of the 377 GC cases, 194 (51.5%) were classified as intestinal type, 138 (36.6 %) as diffuse-type, 39 (10.3%) as mixed-type, and 6 (1.6%) were unclassified. GC cases comprised of 264 (30.0%) negative cases and 113 (70%) positive cases for lymph node metastasis.
We conducted sequencing to detect SNPs with a minor allele frequency greater than 5% in 24 GC patients and 24 healthy controls (35). We identified 4 SNPs in TFF1 (rs184432, rs35448902, and rs225359 in the promoter region and rs2156310 in the 5'UTR), 3 SNPs in TFF2 (rs3814896 and rs13052596 in the promoter region and rs225334 in the 3'UTR), and 1 SNP in TFF3 (rs225362 in the promoter region) through gene sequencing. The genotype frequencies of 8 SNPs (rs184432, rs35448902, rs22535, rs2156310, rs3814896, rs13052596, rs225334, and rs225362) were in the HWE in both GC cases and controls (P> 0.05; data not shown).
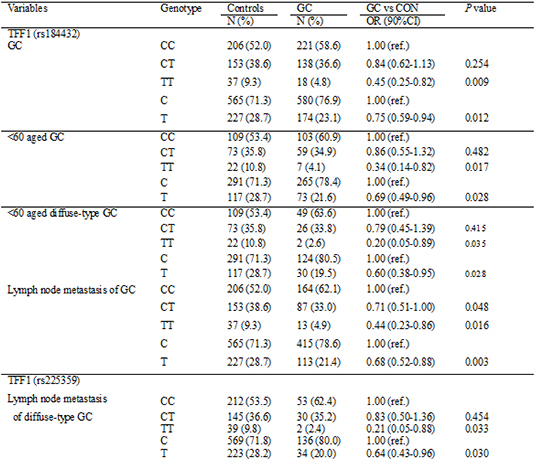
To determine whether TFF1, TFF2, and TFF3 variations were associated with the risk of GC or GC subgroups, we analyzed the genotypes and allele frequencies of TFF SNPs. The genotype and allele frequencies of rs184432 in TFF1 were significantly associated with a decreased GC risk (OR=0.45, 95% CI=0.25-0.82, P= 0.009 and OR=0.75, 95% CI=0.59-0.94, P=0.012, respectively), whereas the remaining SNPs showed no association (Table 2, Supplementary Table 1).
Furthermore, stratification analyses were performed to evaluate the possible correlation of genetic variations of TFF1, TFF2, and TFF3 with the risk of GC or GC subgroups according to the age. Stratified analysis revealed that the genotype and allele frequencies of TFF1 rs184432 were significantly associated with a decreased risk of GC among subjects aged <60 yr (OR=0.34, 95% CI=0.14-0.82, P=0.017 and OR=0.69, 95% CI=0.49-0.96, P=0.028, respectively), but not in subjects aged ≥60 yr. In addition, we found that the genotype and allele frequencies of TFF1 rs184432 were related to a reduced risk of the development of diffuse-type GC in subjects aged <60 yr (OR=0.20, 95% CI=0.05-0.89, P=0.035 and OR=0.60, 95% CI=0.38-0.95, P=0.028, respectively), but not in subjects aged ≥60 yr (Table 3). We observed the lack of association between TFF2 (rs3814896, rs13052596, and rs225334) and TFF3 (rs225362) SNPs, GC risk, and age (data not shown).
In the present study, we investigated whether TFF SNPs were related to lymph node metastasis of GC or GC subgroups. The frequencies of CT and TT genotypes and T allele were associated with a decreased risk of GC, indicating negative lymph node metastasis (OR=0.71, 95% CI=0.51-1.00, P=0.048; OR=0.44, 95% CI=0.23-0.86, P=0.016 and OR=0.68, 95% CI=0.52-0.88, P=0.003, respectively). In addition, an association of the TFF1 rs225359 TT genotype and T allele with a decreased risk of GC was noted, indicating negative lymph node metastasis, as compared to that of the TFF1 rs225359 CC genotype and C allele, respectively (OR=0.46, 95% CI=0.24-0.88, P=0.020 and OR=0.77, 95% CI=0.59-0.99, P=0.041, respectively) (Table 4). To estimate the relevance of TFF variations and lymph node metastasis in intestinal and diffuse-type GC, we conducted a logistic regression analysis. The TFF1 rs184432 TT genotype and T allele were related to a decreased risk of diffuse-type GC, indicating negative lymph node metastasis (OR=0.20, 95% CI= 0.05-0.87, P=0.031 and OR=0.58, 95% CI=0.38-0.87, P=0.01, respectively). Further analyses revealed a significant association of TFF1 rs225359 TT genotype and T allele with a decreased risk of diffuse-type GC, indicating negative lymph node metastasis (OR=0.21, 95% CI=0.05-0.88, P=0.033 and OR=0.64, 95% CI=0.43-0.96, P=0.030, respectively) (Table 5). No association was observed between TFF2 (rs3814896, rs13052596, and rs 225334) and TFF3 (rs225362) SNPs and lymph node metastasis of GC and GC subgroups (data not shown).
DISCUSSION
Until date, it has been implicated that alteration of TFF expression affects the development of several types of cancers. Recently, the association between polymorphisms of TFF and the development of GC was reported in Iranian and Chinese populations, but not in a Korean population (3233). In the present study, we focused on TFF polymorphisms. The aim of this study was to investigate whether polymorphisms in TFF were associated with the risk of GC or GC subgroups in the Korean population. We scanned a Korean-specific polymorphism by sequencing the functional region of TFF that directly affect the gene expression, such as an exon, an exon boundary, and a promoter region. However, we did not detect any Korean-specific novel SNP. We finally selected 8 SNPs, 6 SNPs in the promoter region, 1 SNP in 5'UTR, and 1 SNP in 3'UTR after eliminating the SNP in tight LD (|D'|=1 or r2=1) for genotyping. The proportion of men in the test cases was higher than that in the control cases, whereas the trend in women was reverse (Table 1). To evaluate whether the difference of the proportion of gender is associated with GC risk, we attempted stratified analysis by gender, but any association between TFF SNPs, GC risk, and gender was not observed (data not shown). This result represented that the correlation between TFF SNPs and GC risk is not affected by gender. In our study, TT genotype and T allele of rs184432 in the promoter region of TFF1 was significantly associated with a reduced risk of GC. In addition, in our age-stratified analysis, TT genotype and T allele of rs184432 were associated with a decreased risk of GC and diffuse-type GC in subjects aged <60 yr. This stratified analysis elucidated that rs184432 SNP is more protective against diffuse-type GC than GC in subjects aged <60 yr. Furthermore, our stratified study on lymph node metastasis revealed that CT or TT genotypes, and T allele of rs184432 SNP were associated with a reduced risk of lymph node metastasis-negative GC and negative diffuse-type GC. The TT genotype and T allele of rs225359 promoter SNP were associated with a decreased risk of lymph node metastasis-negative GC and negative diffuse-type GC. We demonstrated that the genetic variation at rs184432 and rs225359 may have a protective effect only on lymph node metastasis-negative GC and negative diffuse-type GC. More recently, a study reported that rs3814896 SNP of TFF2 and rs9981660 SNP of TFF3 selected from a meta-analysis of the Chinese Han Beijing ethnic group were associated with a decreased risk of GC in a Chinese population (33). Nevertheless, although a positive association of TFF2 and TFF3 has been reported in the Chinese population, we did not detect any association between TFF2 and TFF3 polymorphisms and the risk of GC in the studied Korean population (Supplementary Table 1). In our haplotype analysis of 8 SNPs of the TFF family, no statistical association between haplotypes and the risk of cancer was found (P>0.05) (data not shown).
Our study has some limitations. First, the sample size was inadequate for stratified analysis and for analyzing the association in mixed-type GC patients. Second, although Helicobacter pylori is an independent risk factor (3637), we did not investigate the relevance of TFF polymorphism for H. pylori in GC owing to some ethical considerations. Third, we did not investigate whether genetic factors influence smoking, drinking, and diet associated with GC risk due to the lack of data from the GC and control groups. In our future study, the effect of these factors on GC risk will need to be assessed.
In conclusion, our data suggest that single nucleotide change of the rs184432 and rs225359 promoter SNPs of TFF1 might be associated with the susceptibility of diffuse-type GC in the Korean population. However, further functional studies are necessary to clarify the effect of rs184432 and rs225359 polymorphisms on TFF1 gene expression and research in other ethnic groups with larger sample size is recommended to confirm our findings.


 XML Download
XML Download