

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cardiac arrest and resuscitation causes multiple organ dysfunctions due to ischemia and reperfusion injury. Post-cardiac arrest syndrome comprises manifestations of various such organ dysfunctions including post-resuscitation brain encephalopathy, and myocardial dysfunction, as well as symptoms of the underlying disease which caused the cardiac arrest (1). After return of spontaneous circulation (ROSC), the systemic inflammatory response triggered by ischemia and reperfusion produces a post-arrest 'sepsis-like syndrome', where the release of cytokines, adhesion molecules, and plasma endotoxins can cause multi-organ failure and influence clinical outcome after cardiac arrest (2,3,4,5). The kidney is one of the organs susceptible to injuries from ischemia and reperfusion. Ischemia-reperfusion acute kidney injury (AKI) results from endothelial and vascular injuries from activation of various inflammatory cytokines, inflammation involving tubular epithelium and immune cell subgroups, and abnormal repair processes including incomplete repair of tubular cell and fibrosis formation (6, 7). In patients who experience cardiac arrest, AKI can be attributed to ischemia and reperfusion during cardiac arrest, resuscitation, and post-resuscitation phases. A few reports of AKI after cardiac arrest and resuscitation have raised concerns of post-cardiac arrest AKI (8, 9). However, only limited information is available regarding predisposing factors and outcome of AKI after cardiac arrest. This study was performed to investigate the clinical course and predisposing factors AKI, after cardiac arrest and resuscitation.
MATERIALS AND METHODS
Study design and population
This retrospective, observational study was conducted with consecutive patients aged over 18 yr who had survived for more than 24 hr after successful resuscitation from out-of hospital or in-hospital non-traumatic cardiac arrest and who had been admitted to an academic tertiary care center between March 2011 and February 2013. Patients who had any history of renal disease or malignancy were excluded.
Definition of AKI and groups of patients
According to the diagnostic criteria of The Kidney Disease/Improving Global Outcomes (KDIGO) Clinical Practice Guidelines for Acute Kidney Injury, AKI was defined as absolute increase in serum creatinine by ≥ 0.3 mg/dL from baseline within 48 hr, or increase in serum creatinine to ≥ 1.5 times baseline, or urine output of less than 0.5 mL/kg/hr for 6 hr. Stage 1 AKI was defined as increase in serum creatinine by ≥0.3 mg/dL, or increase in creatinine to between 1.5 and 1.9 times the baseline level, or reduction in urine output of <0.5 mL/kg/hr for 6 to 12 hr. Stage 2 AKI was defined as increase in serum creatinine to between 2.0 and 2.9 times the baseline level, or reduction in urine output to <0.5 mL/kg/hr for ≥12 hr. Stage 3 AKI was defined as increase in serum creatinine to 3.0 times baseline, or increase in serum creatinine to ≥4.0 mg/dL, or reduction in urine output of <0.3 mL/kg/hr for ≥24 hr, or anuria for ≥12 hr (10).
Patients' baseline creatinine levels were obtained from pre-existing laboratory data or the lowest steady-state creatinine reached 7 days after cardiac arrest. Peak creatinine level was defined as the highest creatinine measured during admission. Patients were divided into the AKI group (stage 1, 2, and 3) and the non-AKI group.
Data collection
During the study period, our institution provided comprehensive post-cardiac arrest care including maintaining end-organ perfusion, therapeutic hypothermia and general critical care to patients who had been resuscitated from cardiac arrest. Patient data including parameters associated with cardiac arrest and resuscitation during out-of-hospital and in-hospital care were recorded and entered into a cardiac arrest electronic database of our hospital according to Utstein's recommendation (11). Electronic medical records were reviewed to extract clinical data including total shock duration within the initial 24 hr, blood hemoglobin and serum lactate immediate after ROSC and daily peak, serum creatinine and hourly urine output during 2 weeks after ROSC, cumulative duration of vasoactive drug infusion during first 24 hr, and the need for continuous renal replacement therapy (RRT) or maintenance dialysis during admission. Shock was defined as systolic blood pressure lower than 90 mm Hg or mean arterial blood pressure lower than 65 mmHg.
Data analysis
We compared the study variables of the non-AKI and AKI groups. Univariate analysis was performed using chi-square or Fisher-exact tests for categorical variables and Mann-Whitney or Kruskal-Wallis tests for continuous variables. Logistic regression was used to test whether any single variable was associated with AKI. Continuous variables were described as median and interquartile range (IQR). A P value <0.05 was considered to indicate statistical significance. Analysis was performed using IBM SPSS software version 20.0 (SPSS, Inc., Chicago, IL, USA).
RESULTS
Characteristics of the patients
During the study period, 113 adult patients who survived for longer than 24 hr after successful resuscitation following non-traumatic out-of-hospital or in-hospital cardiac arrest were admitted to our hospital. Among them, 31 cases were excluded because of a history of pre-existing renal disease (n=14), refusal of care (n=11), and terminal malignancy (n=6). Finally, 82 (72.6%) patients were enrolled in the study.
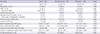
There were no statistical differences in age, sex, place of cardiac arrest, etiology of cardiac arrest, initial ECG rhythm during cardiac arrest, time from cardiac arrest to ROSC, duration of CPR, blood hemoglobin, and serum lactate after ROSC, duration of vasopressor infusion within initial 24 hr, and survival rate between the non-AKI group and the AKI group. Duration of shock within the initial 24 hr after resuscitation was longer in the AKI group than in the non-AKI group (median 130, IQR 48-250 min vs. median 10, IQR 2-59 min) (Table 1).
Incidence, severity and outcome of post-cardiac arrest AKI
AKI developed in 66 (80.5%) patients (AKI group) leaving 16 (19.5%) patients in the non-AKI group. Among the AKI group, 22 (33.3%) patients had stage 1 AKI, 25 (37.9%) patients had stage 2 AKI, and 19 (28.8%) patients had stage 3 AKI. In stage 3 AKI, 7 (36.8%) patients received RRT during admission. No patients needed to receive maintenance dialysis. The 30-day survival rate was lowest in patients with stage 3 AKI (P=0.024) (Table 2). In the AKI group, 90% of patients showed a peak creatinine concentration within 3 days after resuscitation and the creatinine concentration dropped quickly within 4 days to reach a steady-state within 9 days (Fig. 1). The duration of shock within the initial 24 hr after resuscitation increased with the stage of AKI (non-AKI group: median 10, IQR 2-59 min, stage 1 AKI: median 59, IQR 27-105 min, stage 2 AKI: median 134, IQR 57-187 min, stage 3 AKI: median 339, IQR 132-484 min, P<0.001) (Fig. 2).
Treatment for post-cardiac arrest AKI and the need for RRT
Seven patients were treated with RRT using the continuous veno-veno hemodiafiltration mode. RRT was indicated due to uremia with pulmonary edema in 5 cases, and hyperkalemia with metabolic acidosis in 2 cases. All patients were treated within 72 hr after ROSC. Accumulated duration of RRT did not exceed 220 hr (median 72, IQR 50-209 hr). Four of these seven patients (57.1%) survived.
Predictors of post-cardiac arrest AKI
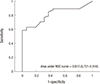
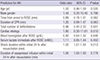
Multivariate analysis revealed that only duration of shock was related to post-cardiac arrest AKI (odds ratio 1.02; 95% confidence interval 1.01-1.04). Age, sex, etiology of cardiac arrest, time from arrest to ROSC, duration of CPR, total number of defibrillations, blood hemoglobin and serum lactate immediate after ROSC, and duration of vasopressor infusion were not associated with development of AKI (Table 3). The area under the receiver operating characteristic curve that described the sensitivity and specificity of shock duration for different cutoff levels was 0.815 (0.720-0.910) (Fig. 3). The optimum cutoff to predict AKI was identified as 57 min, with respective values of 70.8% for sensitivity and 75% for specificity.
DISCUSSION
Our study demonstrated that AKI was a frequent consequence after resuscitation, and the duration of shock after ROSC was related to the development of AKI in patients who experienced cardiac arrest. A longer duration of shock caused a more severe degree of AKI. Development of mild or moderate degree AKI (stage 1 or 2) was not associated with resuscitation outcome. However, patients who had stage 3 AKI after resuscitation had a worse prognosis than patients without AKI or those with a mild to moderate degree of AKI. Variables associated with cardiac arrest including etiology of cardiac arrest, duration of CPR, and duration of cardiac arrest were not associated with development of AKI.
AKI frequently occurs after cardiac arrest and resuscitation. The incidence of AKI in our study was much higher (80%) than in previous reports ranging from 12% to 40% (8, 9, 12). Difference in the incidence of post-cardiac arrest AKI may be attributed to two reasons. Firstly, previous reports applied the definition of acute renal failure as a 25% decrease of creatinine clearance within 24 hr after admission, by AKIN or RIFLE criteria (12,13,14,15). In this study, we applied the KDIGO criteria in defining AKI, resulting in a much higher incidence of AKI. In patients resuscitated from cardiac arrest, KDIGO criteria, which retain the increase in serum creatinine over a period of seven days, may be more suitable to define AKI than other definitions because baseline creatinine level is unknown in most cardiac arrest patients. The clinical course of AKI after resuscitation differed along with the severity of AKI. A significant proportion of patients with stage 3 AKI needed renal replacement therapy and had lower 30-day survival than patients with no AKI or milder degree AKI. This finding suggests that a severe degree of AKI can develop after resuscitation and may affect the clinical outcome.
Several reports investigated the factors affecting development of AKI after cardiac arrest and resuscitation. These factors include variables from pre-cardiac arrest morbidity as well as variables during cardiac arrest and resuscitation such as pre-arrest renal impairment, history of hypertension or congestive heart failure, duration of cardiac arrest and CPR, and epinephrine dosage (8, 13). However, whether cardiac arrest is itself associated with development of AKI has remained unclear. Here we found that intra-arrest variables including duration of cardiac arrest were not associated with development of AKI after resuscitation. Previous analysis of 187 patients resuscitated from cardiac arrest revealed that duration of cardiac arrest was not independently associated with renal outcome (13). Chua et al. (16) reported that presence of post-resuscitation cardiogenic shock, higher serum lactate levels at 12 hr from cardiac arrest, pre-cardiac arrest renin-anigiotensin-aldosterone system blockade therapy, and higher baseline serum creatinine are independently associated with a higher increase in serum creatinine in patients resuscitated from cardiac arrest. Intra-arrest variables including duration of total down time were not associated with development of AKI. Their study suggested that significant AKI is related to post-resuscitation cardiogenic shock and post-cardiac arrest disease rather than cardiac arrest itself. Multivariate analysis of our data also revealed that duration of shock after resuscitation was the only factor related to development of AKI and that the severity of AKI was correlated with duration of shock. The temporal pattern of ischemic AKI, which is comprised of initiation, extension, maintenance, and recovery phases, can be substituted as a potential mechanism of post-cardiac arrest AKI (17). Potential insults of AKI developed after resuscitation are ischemic injuries of the kidney from a hypoperfusion state during cardiac arrest, CPR, and the post-resuscitation phase. The initial phase of post-cardiac arrest AKI begins with occurrence of cardiac arrest and resuscitation. Subsequent injuries to the kidney come from ischemia due to circulatory shock and inflammatory response during the post-resuscitation period. Ischemic injuries from circulatory shock after resuscitation may exert sustained insult to the kidney during the extension phase of AKI. A significant number of patients who have been resuscitated from cardiac arrest have circulatory shock resulting from various causes including post-cardiac arrest myocardial dysfunction or sepsis-like syndrome during the post-resuscitation period (2, 18, 19). Post-resuscitation circulatory shock can further injure the renal tubular cells. Therefore, the mechanism of AKI after resuscitation may be that initial ischemic exposure of the kidney during cardiac arrest and resuscitation causes sublethal injury to tubular cells in a transient, reversible process, but subsequent exposure to hypoperfusion from circulatory shock during the post-resuscitation period brings significant impairment of renal function. Current guidelines for CPR recommend hemodynamic optimization during the post-resuscitation period as a component of comprehensive post-cardiac arrest care to promote favorable neurologic recovery (20). In addition to neurologic recovery, it is expected that maintenance of optimal blood pressure and meticulous treatment of circulatory shock will help prevent occurrence of post-cardiac arrest AKI.
We note that our study had several limitations. We relied on a retrospective, observational study design at a single tertiary care center. Our institution has a cardiac arrest database system to keep medical records of cardiac arrest patients, including variables for pre-hospital and in-hospital events in the Utstein style. Therefore, variables associated with cardiac arrest and resuscitation could be extracted from the cardiac arrest database and clinical and laboratory findings including creatinine level could be extracted from the electronic medical records. Potential nephrotoxic substances or iodinated contrast agents that were administrated after resuscitation may have affected post-cardiac arrest renal function. We could not evaluate their effect on post-cardiac arrest AKI because there were too many substances that could have influenced the magnitude of renal toxicity, such as antibiotics, neuromuscular blocking agents, sedatives, cardiovascular drugs, and contrast agents. We could not know whether AKI was developed during cardiac arrest and resuscitation or post-cardiac arrest period in this study. AKI was developed within 3 days (median 1, IQR: 1, 2 days) from cardiac arrest in all patients. Therefore, AKI can be attributed to combined insults including ischemia and reperfusion during cardiac arrest and resuscitation and hemodynamic compromise during post-cardiac arrest period. Finally, baseline creatinine levels of patients who had no pre-existing laboratory data were obtained the lowest steady-state creatinine reached 7 days after cardiac arrest. However, the lowest steady state creatinine level might not be same as the creatinine level prior to cardiac arrest.
In conclusion, the occurrence and severity of post-cardiac arrest AKI is associated with the duration of shock after resuscitation. A significant proportion of patients with a severe degree (stage 3) of post-cardiac arrest AKI requires renal replacement therapy.



 XML Download
XML Download