

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The United States Institute of Medicine defined primary care as "the provision of integrated, accessible health care services by clinicians who are accountable for addressing a large majority of personal health needs, developing a sustained partnership with patients, and practicing in the context of family and community" in 1996 report (1). In Korea, primary care is defined as "the delivery of health care services first encountered by people". It refers to "a discipline in which physicians being well-aware of patients in the context of their family and community, resolve common health care needs of people by maintaining a patient-doctor relationship over time and coordinating health care resources appropriately" (2). Primary care is important in the sense that it is the first and most frequently sought official health care by people in order to deal with their health issues. By establishing the foundation of the health care delivery system, primary care is an efficient health care channel meeting 75%-85% of all medical needs. It also affects the public views regarding doctors and medical service as well as the performance of the overall health care systems (3, 4). In particular, effective primary care can minimize unnecessary expenditure of resources and thus lead to positive health outcomes at lower cost. As patients can access quality health care service through the primary care system regardless of their income level, primary care contributes to the overall health care system by ensuring efficiency, effectiveness, and fairness in care (5, 6).
Despite the aforementioned advantages of primary care, Korea has a weak primary care system which has continued to deteriorate over the years, mainly due to the following reasons: 1) undifferentiated health care delivery system which creates competitive rather than cooperative or complementing relationships between hospitals and clinics; and 2) virtual freedom of choice regarding the medical institution through the availability of multiple channels for patients to directly access hospitals without having to obtain referrals from clinics (7, 8, 9, 10). Moreover, as health care providers in Korea are reimbursed according to the fee-for-service system (8), there is a structural barrier to ensuring key attributes of primary care, i.e. comprehensiveness, coordination, and continuity, and it is, therefore, difficult to maintain ideal patient-doctor relationships (11). Nevertheless, in order to deal with the current health care issues in Korea, including an aging society, increase of chronic diseases, growing demands for health care and the rising cost associated with the advancement of medical technologies, dissatisfaction regarding health care among the general public, including patients, and the difficulties encountered by physicians in operating clinics, it is imperative to take an entirely new approach that veers away from that of previous actions. In fact, other countries have undertaken various initiatives to strengthen their primary care in order to deal with the same issues faced in Korea (3, 11). To this end, the OECD has indicated the problems related to Korea's primary care system, including not being able to effectively deal with the challenges of an aging population and chronic diseases, and has stressed the need for a completely new strategy to improve Korea's primary care system by shifting the focus away from acute care services (12, 13).
From a global perspective, the Korean primary care system falls at the bottom among comparable OECD countries, and the public trust of its quality is also low (3, 14, 15). Therefore, to actively respond to these issues, an effective action plan must be established to improve the existing primary care system of Korea. Previous studies have examined various aspects of primary care including its concept and relevant perception and have reviewed the best practices abroad to benchmark (2, 3, 17). However, most of these studies have simply introduced the best practices from countries abroad to Korea or have made some suggestions for areas of improvement in the Korean health care system, and very few have addressed the feasibility or specific strategies for benchmarking cases from other countries. Furthermore, little or no attempt has been made to receive the opinions of those directly engaged in primary care and to then provide solutions.
Given these issues, our study was intended to understanding the current state, issues, perceptions, and solutions regarding primary care in Korea. The survey was conducted with private practice internists who are specialists and who have been leading Korea's primary care system by representing the largest number of all clinics in Korea.
MATERIALS AND METHODS
Study population
This study was conducted on 3,658 physicians who are members of the Korean Physicians' Association, representing general internists. During the four-week period between October 29 and November 22, 2013, we sent out emails using a web-based survey program offered by a professional research site. A total of 606 (16.6%) subjects in the sample responded, although the actual analysis was performed on 466 (12.7%) individuals after excluding incomplete responses.
Items of the questionnaire
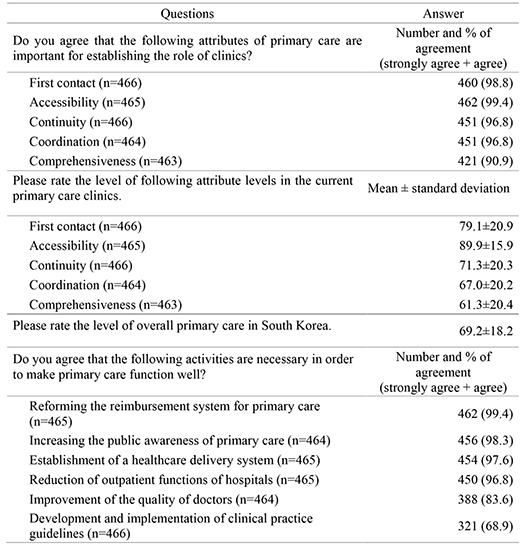
We first prepared a draft questionnaire based on domestic and international literature and after consulting with primary care experts, the questionnaire was finalized (18,19,20). The questionnaire broadly covered five topics. The items in the first section on general characteristics included gender, age, duration of running clinic, and the level of satisfaction in the surgical clinic. The second topic contained items regarding the importance of the role of primary care clinics, the current level of primary care in Korea, and the areas for future improvements. In the third section, we identified five, key attributes of primary care and asked about perceptions regarding the reason why hospitals are preferred over clinics in case of patient illness (Contact), issues regarding accessing care during the night or on weekends and holidays (Accessibility), issues regarding referrals and coordination by primary care (Coordination), issues regarding providing comprehensive patient education (Comprehensiveness), and issues regarding managing patients with chronic diseases (Continuity). The last section of the questionnaire covered items regarding opinions about the current management system of chronic diseases and the new management system of chronic diseases led by the clinic (Table 1).
RESULTS
General characteristics of the study participants
Out of the 466 respondents, 426 were males (91.4%) and only 40 were females (8.6%). The average age of the respondents was 49.6 yr, and with the 213 respondents in the age group of 40-49 comprising the largest share (45.7%). The average number of years since opening a clinic was 13.7 yr, and the opening period of 11-20 yr received the most responses with 221 respondents (47.4%). As for the clinic type, solo practitioner (1 doctor) was the most common type with 347 respondents (74.5%), and 57.3% of the respondents indicated they were dissatisfied with the running clinic (very dissatisfied: 8.6%, dissatisfied: 48.7%). Regarding the reasons for their dissatisfaction, respondents answered increased government regulation (92.5%), excessive working hours (55.8%), difficulty in human resources management (53.6%), economic difficulty (51.7%), and increased patient demands (39.0%) (Table 2).
The importance of the role of primary care clinics, the current level of primary care, and future improvements
When asked about the importance of the role of primary-care clinics in order for primary care to perform well for each of its five key attributes, the overwhelming majority of respondents replied in favor of the importance of the role of primary-care clinics regarding all five attributes (response rates of strongly agree + agree). In particular, Accessibility (99.4%) was rated to be the most important attribute, followed by First Contact (98.8%), Continuity (96.8%), Coordination (96.4%), and Comprehensiveness (90.3%). However, the overall level of primary care in Korea was rated only 69.5, with each attribute of primary care scoring in the order of Accessibility (89.9%), First Contact (79.1%), Continuity (71.3%), Coordination (67.0%), and Comprehensiveness (61.3%). When asked about the agreement of the six activities necessary to be carried out by clinics in order for primary care to function well (response rates of strongly agree + agree), 'Reforming the reimbursement system for primary care' received the highest response (99.4%), followed by 'Increasing the public awareness of primary care' (98.3%), 'Establishment of a healthcare delivery system' (97.6%), 'Reduction of outpatient functions in hospitals' (96.8%), 'Improvement of the quality of doctors' (83.6%), and 'Development and implementation of clinical practice guidelines (68.9%)' (Table 3).
Perception on the five key attributes of primary care
Regarding preferring hospitals over clinics in case of a patient illness, the most usual response was, 'Better facilities and equipment of hospitals (97.4%)', followed by 'Problem of the healthcare delivery system allowing patients to freely choose hospitals or clinics (86.9%)', 'Confidence in a hospital's medical staff (85.0%)', 'Promotion of hospitals through media (83.7%)', 'Organized care system of hospitals (82.4%)', 'Lack of facilities and equipment in clinics (77.7%)', 'Lack of an organized care system in clinics (66.4%)' and 'Lack of trust of clinics (62.2%)'. However, when asked about the quality difference between doctors at hospitals and those in clinics, the highest response was, 'There is no difference (69.5%)'.
When asked about whether night, weekend, and holiday office hours are needed for primary care, the vast majority (89.5%) responded the need for 'Saturday morning (before 12:00 pm)', while over half of the respondents did not agree with the need for office hours during non-business hours. In the question regarding the reasons why providing care is difficult during non-business hours, the highest response was 'Hope to have more personal time (97.2%)', followed by the following responses in order: 'Shortage of manpower during the night and on weekends and holidays (94.2%)', 'Low reimbursement rate for night, weekend, and holiday patient treatment (91.4%)', 'Small numbers of patients (86.7%)', 'Risks that may occur in the absence of systems for handling emergency situations (82.6%)', and 'Ease of use of a nearby hospital's emergency system (78.7%)'.
With respect to Coordination, when asked about why physicians refer patients to other healthcare providers, the most frequent response was, 'Necessity for special care or diagnosis (98.9%)' followed by 'No equipment available (96.3%)', 'Not an expert on it (94.6%)', 'Patients' wishes to be referred to a hospital or another clinic (83.9%)', and 'To avoid risks or claims (82.6%)'. As reasons for not referring patients to hospitals or other clinics, the respondents indicated 'Patients' wish to be treated in a clinic (52.7%)', 'All treatment required by the patient is possible (45.4%)', and 'Concerns that patients may go elsewhere (33.1%)'. When asked specifically about why patients are referred to community resources and other healthcare providers, the largest response was, 'For tuberculosis control' at 74.2% followed by 'For anti-smoking education (71.2%)', 'For nutrition counseling (55.8%)', and 'For psychological counseling (47.5%)'. Only 21.7% of the respondents indicated that they follow patients who are referred to hospitals, community resources or other healthcare providers.
Regarding Comprehensiveness of care in terms of patient education, i.e. illness prevention, improving lifestyle, when asked whether patient education is needed for lifestyle modification, the overwhelming majority (95.3%) indicated that it is necessary (Mostly: 28.1%, Relatively: 67.2%). However, alternatively, only 30.5% of the respondents indicated that they provide education regarding lifestyle modification to all patients who visit their clinics. Similarly, regarding the question, 'How many patients do you consult regarding cancer screening and cancer prevention', only 19% responded, 'All patients who visit '. As to why patient education is difficult, respondents chose, 'No reimbursement system with respect to patient education and consultation (95.7%)', 'Shortage of manpower for patient education and infrastructure (90.8%)', 'Busy due to the lack of time in the process of patient care (89.3%)', 'Would like to educate patients, but lack knowledge regarding patient education (14.4%)', and 'Patient education is not the duty of clinics (11.6%)'.
Lastly, regarding whether it is necessary to remind patients with chronic diseases, such as hypertension and diabetes, about their next visit by a phone call, short message service (SMS) or e-mail, 63.5% (Mostly: 11.8%, Relatively: 51.7%) of the respondents marked it as needed. On the other hand, 87.6% responded that they take no action if patients with chronic disease do not visit their clinic. Regarding the reasons why managing patients with chronic diseases is difficult, the responses were marked in the following order: 'Difficult to hire staff who are exclusively responsible for managing patients (95.7%)', 'Difficult to undergo procedure of consent to use personal information (92.9%)', 'Can be mistaken as touting (87.3%)', 'Can create anxiety in patients when contacting them by phone call or SMS (54.7%)', and 'Cannot assure if a patient will visit even though the reminder was given (47.6%)' (Table 4).
Opinions regarding the current management system of chronic diseases
When asked about the agreement with the current management system of chronic diseases, 52.6% indicated that they disagree and only 29.6% were in agreement. Regarding the reasons for opposing the current management system of chronic disease, 99.2% indicated their 'Concerns about the strengthened intervention of government in clinic', followed by 'Concerns about the low reimbursement rate (95.1%)', 'Concerns about the strategic move for reform of reimbursement system (95.1%)', 'Concerns that the demand of patients will be higher than level of compensation (83.1%)', and 'Concerns it could be a barrier to entry of new practitioners (81.4%)'. To effectively activate the current management system of chronic diseases, respondents marked that the following actions must be taken: 'Actions to limit public health center (96.8%)', Physician's direct involvement in health care policy allowed (93.8%)', 'Provide sufficient incentives (91.2%)', and 'Support manpower to be exclusively responsible for patient education and explanation' (81.1%).
To the question 'Do you agree with the new management system of chronic diseases led by clinic?', 56.9% were in agreement while 16.3% disagreed. And 26.6% were undecided. Regarding which organizations to co-work with if the new management system of chronic diseases led by a clinic is implemented, most respondents chose 'Korean Medical Association' (87.9%). Moreover, while 'Regional senior general hospital (69.6%)', 'Regional general hospital (63.5%)', and 'Regional hospital (57.3%)' were favored among the respondents, the following organizations received lower responses: 'Regional public health center (33.9%)', 'National Health Insurance Corporation (17.8%)', 'Third party non-profit organizations (except for hospitals) (16.8%)', 'Third party government organization (10.7%)' and 'Third party private profit organizations (8.0%)' (Table 5).
DISCUSSION
This study was conducted using clinical internists of Korea in order to understand the current status and issues of primary care in this country. It is essential to survey the opinions of private-practice internists as they are the most representative group of specialists as they comprise the largest share of clinical doctors in Korea and are considered to be the usual primary care providers. Moreover, primary care policies are subject to great struggle regarding their implementation in Korea if they are strongly opposed by internal-medicine practitioners. However, no attempt has been made at the national level by this group to collect their perceptions or opinions regarding primary care, and, therefore, our study is unique and the results of great significance to this field of study.
Our findings show that clinics are perceived to have a very important role in primary care among clinical internists. However, their evaluation of the overall status of Korea's primary care was low and with coordination and comprehensiveness considered to be the two weakest attributes of primary care. Such views closely reflect other study results that evaluated the overall quality of primary care in Korea (3, 14, 15, 16). Coordination and comprehensiveness of primary care have been particularly criticized to be very weak in Korea (21), and our study found that internal-medicine practitioners also shared similar views. Such results may positively contribute to improving the primary-care system in Korea. In other words, given the facts that clinical internists, in principle, agree with the importance of primary care and that they are exactly aware of which areas of primary care need improvement, eliminating the factors that cause their opposition to the primary-care policies may help to alleviate their negative perception regarding these policies.
Our respondents strongly supported the policies intended to help local clinics become effective primary-care providers, such as revising the fee-for-service system, enhancing patients' perception, establishing a strong foundation for the healthcare delivery system, and reducing outpatient services in hospitals, although they showed relatively little support regarding improving the quality of doctors or developing (and making use of) standard, clinical-practice guidelines. In particular, private-practice internists generally believed the distortions of the existing, fee-for-service system to be the greatest deterrent to effective primary care. Under the current low-fee structure, clinical doctors are forced to extend their office hours in order to increase their income and consequently reduce the time they spend treating each patient. Therefore, practitioners are pressed for the time required to provide comprehensive and continuous service and adequate consultation which are critical components of primary care, and both doctors and patients may experience dissatisfaction (16). In addition, given the fact that the fee for identical treatment is the same across the type of medical institution, while the fixed rate applied to hospital-size medical institutions is greater than that of clinics, hospitals may be attracted to expanding their primary-care-based, outpatient service. Therefore, some could argue that the current fee schedule needs to be amended so that outpatient treatment fees for clinics and inpatient treatment fees for hospitals are set higher.
In order to enhance the patient perception, the most crucial step is to redeem their trust in primary care. This problem is directly linked to the first contact among the five attributes of primary care in which patients tend to prefer secondary or tertiary healthcare institutions over clinics. If we blame the phenomenon in Korea where patients prefer to visit hospitals rather than clinics, despite the higher cost, longer waiting and additional travel time, to inappropriate use of medical service, the real problem is overlooked. In fact, from the patient's point of view, visiting a university hospital may be a more economical and efficient choice as it solves all of the healthcare issues at one stop. In other words, the preference for hospitals among patients is derived from widespread distrust in clinical service. Our results showed that internal-medicine practitioners believe that there is no quality difference between hospital doctors and clinicians, not accounting for the facility and its equipment, yet patients had rather strong doubt regarding the quality of care provided in clinics (16).
Therefore, it is imperative to find ways to guarantee the quality of primary care. These measures should include offering various training activities to enhance the quality of doctors as well as developing and making use of standard, clinical-practice guidelines, although this method may be subject to the opposition of clinicians as in the past such initiatives have often been coupled with the government's regulatory strengthening or healthcare fee reduction moves (21). Nevertheless, if the quality of primary care can be raised through the aforementioned measures or if patients and the general public can be well-informed that there is no quality difference between clinics and hospitals in terms of primary-care service and that only discrepancy is the fee for treatment.
In terms of accessibility, the compelling majority of private-practice internists agreed on the need for office hours on Saturday mornings, although regarding other non-business hours, less than 50% agreed. However, as both physical and economic accessibilities to primary care have greatly improved over time in Korea, there is a strong desire among Koreans to see better accessibility in terms of time such as extended office hours on nights, weekends, and holidays (16). Such a demand for improved accessibility in terms of office hours is supported by the fact that non-emergency visits to emergency rooms comprise almost 40% of these visits (22). Yet, respondents indicated that the main reason for their being unable to offer primary care during non-business hours is due to their need to set aside personal time rather than for manpower or economic issues. This implies that clinical internists want to be assured regarding the quality of their personal lives. Therefore, simply increasing the fee schedule for primary care during off-business hours may not improve hourly accessibility, however, a more appropriate and practical policy would be to provide support in favor of joint practices where office hours can be flexibly shared between partners.
This survey confirmed a number of problems related to the three attributes of primary care, i.e. coordination, continuity, and comprehensiveness. Coordination is an essential function of primary-care clinicians, although our study found that coordination among private-practice doctors is quite weak. In fact, 33.1% of our respondents had incidents where they did not make referrals for their patients to other providers for fear of losing their patient business. Also, only 21.7% replied that they contact patients regarding follow-up based on referrals. With regard to comprehensiveness, private-practice internists were well-aware of the need for patient education and consultation regarding disease-prevention efforts and life-style modification, although they did not actively carry out these activities. The main barriers to keeping up with patient education were issues related to the reimbursement system, shortage of manpower and infrastructure, and limited time available for providing care. There were responses, although few, that the reasons patient education is difficult are due to a lack of knowledge regarding patient education and that it is not the duty of clinicians to offer patient education. In answer to the questions regarding continuity, clinical internists agreed on the need to remind patients of their appointment date in order to provide continuous care for patients with chronic illness, i.e. high blood pressure, diabetes, etc., although 87.6% of the respondents said that they do not take any action if patients do not show up for appointments and which indicates insufficient continuous patient monitoring.
When asked about the current management system of chronic disease, the majority of internal-medicine practitioners opposed it, mainly due to stronger government intervention in clinics. Introduced in April, 2012, the current management system of chronic disease provides patient education, standard clinical-practice guidelines, and reminder service to patients with chronic illness for whom it is essential to keep monitoring themselves. Doctors are provided with the health history of patients in order to ensure that they can improve the patients' health and prevent complications. The long-term goal of this management system is to reduce the healthcare expenditure (23). The objective of the program, itself, is straightforward and indisputable. However, given the past government policies that had left out providers and where enforced, lopsided, clinical internists tended to view the current management system of chronic diseases to be aimed at lowering their fees for patient care or amending the reimbursement system. Such a perception has created a strong sense of opposition among clinicians to the chronic-illness care system. In the end, private practice internists still distrust of the government.
As an option for resolving the current tension, this study asked clinicians' views regarding the chronic illness care system led by clinics. The concept is grounded in the fact that private-practice internists are the most appropriate care providers to patients with chronic illness as they actually provide primary care. A clinic-led, chronic disease management system would be by and large identical to the existing system in terms of its context, although the main difference would be that the system will be run by doctors instead of the government. In other words, doctors would be in charge of the entire process of the chronic-illness management system, including planning, implementation, and evaluation, and thus encouraging their active involvement as well as giving them a share of responsibility. The fact that the majority of respondents were in favor of the new management system of chronic disease shows a positive change in attitude in contrast to their previous stance. Therefore, the government should adopt a different set of policies to accommodate such change in attitude among doctors and to regain their trust. The government should learn from past experience in which government-led programs resulted in various, unforeseen side effects and misunderstandings, and in turn introduce a new management system for chronic illness which would directly involve doctors in the program design and implementation as well as its evaluation. Therefore, it is notable to recognize the recent shift in policy direction, namely the 'Health Platform' project launched by the Ministry of Health and Welfare in 2014, which puts emphasis on the autonomy of doctors (24).
This study has some limitations. First, there is a possibility of respondent bias due to the low response rate. This bias might cause problem of generalizability from our study. Second, there is a potential for a selection bias to happen, because the study population in this study was only the member of the Korean Physicians' Association. However, the chances of that happening would not be great, regarding the most of the general internists (3,658/3,967=92.2%), who are opening a clinic, belong to Korean Physicians' Association (25). Third, as our study was only conducted interviewing internal-medicine practitioners, we did not take into account the views of other primary-care providers such as family practitioners and general practitioners. Nevertheless, the reason we particularly surveyed private-practice internists for this research is that, whereas in Europe general practitioners or family practitioners take charge of primary care and specialists treat patients with referrals, such a distinction is not apparent in Korea. It will be meaningful to expand survey target population to other primary-care providers such as family practitioners in the research of future.
The significance of this study is that it is the first attempt to collect the views of private-practice internists at the national level who are the actual primary-care providers and comprise the largest proportion of clinicians in Korea. Internal-medicine practitioners strongly agreed on the importance of clinics for primary care, although their evaluation of the level of primary care in Korea was found to be somewhat low. As identified in a previous qualitative study (16), coordination and comprehensiveness, both of which are essential in managing chronic illness, were considered as the weak attributes of primary care in Korea. Given the strong inclination toward a new management system for chronic illness that gives autonomy to doctors, it is recommended that policy changes should be adopted in such a way that clinical internists are drawn to actively participate in primary-care policies.





 XML Download
XML Download