

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Bladder augmentation remains one of the greatest surgical challenges in the field of urology. Conventional bladder reconstruction using gastrointestinal tissue is associated with a series of complications (mucus production, bacterial colonization, electrolyte imbalances, or malignancy), significant morbidity, and functional alterations (1). Tissue engineering technique can circumvent many of these limitations and therefore has become considered as a potential alternative for bladder reconstruction.
The chief obstacle over the years to reconstructing the bladder through regeneration has been the absence of an ideal biomaterial that can provide a structurally intact low-pressure reservoir, serve as a scaffold for the healing and regeneration of the bladder wall, and retain normal function until it is replaced by host tissues (23). Until recently, three classes of biomaterials have been extensively investigated for bladder tissue engineering. Naturally derived materials, e.g. collagen (4) and alginate (5), acellular tissue matrices, e.g., bladder submucosa (BSM) (6) and small intestinal submucosa (7), and synthetic polymers, e.g., polyglycolic acid (PGA) (8), polylactic acid (PLA) (9), and polylactic- co-glycolic acid (PLGA) (10). However, none of them could provide required results for ideal biomaterials. In an effort to fabricate a scaffold that can be applied to morphological and functional bladder reconstruction, we have been worked to develop a composite scaffold composed with synthetic and natural derived biomaterial. As a synthetic biomaterial, polycaprolactone (PCL) was investigated as a potential substitute for bladder tissue reconstruction because of its flexibility, biocompatibility, stability, and resistance to resorption (11). We could fabricate a blend of PCL with Pluronic F127 (F127) and bladder submucosa matrix (BSM), which has been shown to be a non-immunogenic, non-cytotoxic collagen-rich membrane that can be rapidly replaced by native tissues (12).
In our previous work, the PCL/F127/3 wt% BSM composite scaffold exhibited significantly enhanced hydrophilicity, the surface was easily immobilized, and there was no evidence of teratoma formation in vivo (12). Based on our previous results, we fabricated an advanced scaffold containing a specific growth factor to enhance proliferation of smooth muscle cells and urothelial cells, which are the two essential cell types for functional bladder regeneration. Basic fibroblast growth factor (bFGF) has been shown to stimulate the proliferation and survival of both smooth muscle and urothelial cells (13), thus suggesting the benefits of bFGF-loaded scaffolds for urological tissue engineering applications. Therefore, to fabricate a scaffold for bFGF delivery, we covalently conjugated heparin to the surface of a scaffold to form a heparin-immobilized scaffold, which was then loaded with bFGF (scaffoldheparin-bFGF) (14).
Tissue engineering of bladder also requires ideal cell source. Autologous cells are one of the most popularly used cells with the advantages including, decreased infection, require no immunosuppression reagents, and do not require histocompatibility matching (15). However, autologous bladder cell harvest procedures are surgically invasive, and the prolonged cell expansion methods are expensive, subject to contamination, and unrealistic for routine clinical use. Alternative sources of healthy and abundant bladder tissue are desired for optimal bladder engineering and bladder regeneration. Skeletal muscle cells, bone marrow stromal cells, embryonic, and parthenogenetic stem cells are all currently under investigation as potential future alternatives, however these modalities are in their infancy. For the purpose of this study, we turned to a stem cell source from urine, i.e., urine-derived stem cells (USCs). USCs have been proposed as an alternative stem cell source for urological tissue reconstruction since they have mesenchymal stem cell characteristics and have demonstrated the capacity to differentiate into a variety of urological cell lineages (16).
In this study, we hypothesized that a USC-seeded scaffoldheparin-bFGF graft would promote regeneration of the bladder wall. To investigate the synergic effect of the USC-scaffoldheparin-bFGF in terms of smooth muscle and urothelial layer regeneration, the scaffoldheparin-bFGF was characterized by quantifying the amounts of immobilized heparin and loaded bFGF released, and assessing the biocompatibility and differentiation of USCs in vitro. In addition, the potential of the USC-scaffoldheparin-bFGF for bladder reconstruction was evaluated in vivo using a rat model.
MATERIALS AND METHODS
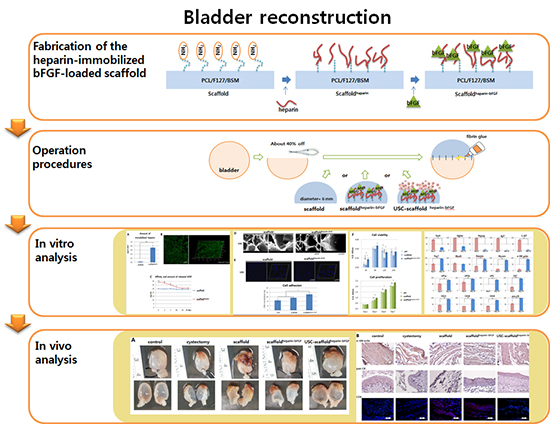
Fabrication of the heparin-immobilized bFGF-loaded scaffold (scaffoldheparin-bFGF)
PCL (MW 80,000 Da; Sigma-Aldrich, St. Louis, MO, USA), tetraglycol (glycofurol; Sigma-Aldrich), Pluronic F127 (MW 12,500 Da; BASF, Ludwigshafen, Germany), and BSM were used for scaffold fabrication. BSM was prepared as described in our previous report, and the formulation consisting of 3 wt% BSM of the polymer base was chosen (12). The PCL/F127/BSM scaffold was prepared using an immersion precipitation method (17). A PCL pellet/Pluronic F127 powder mixture (95/5 [w/w]) was dissolved in tetraglycol (12 wt%), and BSM powder was evenly mixed with the polymer solution. The mixed solutions were poured into a polytetrafluoroethylene mold (70×70×0.4 µL) and then directly immersed in water for 1 hr at room temperature. After additional washing and vacuum drying, the PCL/F127/BSM composite scaffold was sterilized using ethanol.
Heparin (MW 18,000 Da; Sigma-Aldrich) was immobilized to the scaffold to bind bFGF to the scaffold. The scaffold was pre-wet with 70% (v/v) ethanol, washed with deionized water, and hydrated with a 0.1 M 2-(N-morpholino) ethanesulfonic acid (MES) buffer (pH 5.5). The carboxylic acid groups of heparin were activated using 1-ethyl-3-(3-dimethylaminopropyl) carbodiimide hydrochloride (EDC) and N-hydroxylsuccinimide (NHS) for 4 hrs. The scaffold was soaked in 10 mL of the heparin solution with gentle agitation at 48℃ for 6 hr. The heparin-immobilized scaffold was rinsed with the 0.1 M MES buffer (pH 5.5) solution and phosphate buffered saline (PBS, pH 7.4) (18). The heparin-immobilized scaffold was soaked in PBS containing 100 ng/mL of bFGF (Peprotech, Rocky Hill, NJ, USA) and 1 mg/mL of bovine serum albumin (Sigma-Aldrich) for 4 hr with gentle agitation, and then the scaffold was washed with PBS (Fig. 1).
Determination of heparin and bFGF content
Heparin content on the scaffold surface was determined by the toluidine blue colorimetric method (1920). The scaffold was placed in 1 mL of 0.2% NaCl solution, then 1 mL of toluidine blue solution was added, and inner air was removed. After 10 min of vibration, 2 mL of hexane was added and mixed by vortexing. The absorbance of the aqueous layers at 631 nm was determined by a UV spectrophotometer. Immobilized heparin was visualized by labeling with fluorescein isothiocyanate (FITC, 1 mg/mL) at 4℃ for 3 hr. The FITC-labeled scaffold was cryosectioned (20 µm) and observed under a confocal laser-scanning microscope (LSM510, Carl Zeiss, Oberkochen, Germany).
For the bFGF affinity and release test, the scaffoldheparin-bFGF was immersed in 1 mL of PBS containing 1% bovine serum albumin at 37℃ for 28 days. The solution was collected and replaced with fresh medium. The amount of bFGF was determined using a Quantikine Immunoassay kit, according to the manufacturer's instructions (Human bFGF Quantikine ELISA kit, R&D Systems, Minneapolis, MN, USA). An unmodified heparin scaffold was used as a control (n=3).
Scaffoldheparin-bFGF surface morphology, biocompatibility, and effects on cell differentiation
Urine samples from the upper urinary tract were obtained from a 52-yr-old female patient. A volume of 100 mL of each urine sample was centrifuged, and the cell pellets were washed with PBS. The cells were cultured in mixed medium consisting of keratinocyte serum-free medium and progenitor cell medium (Gibco-Invitrogen, Grand Island, NY, USA) in a 1:1 ratio (21).
The surface morphology of the scaffolds and adherent cells on the scaffolds were assessed using a field emission scanning electron microscope (FE-SEM, S-4300, Hitachi, Hitachi-shi, Japan). The USC-loaded scaffolds were fixed in a 4% paraformaldehyde (PFA, Sigma-Aldrich) solution at 30℃ for 45 min, followed by washing with dH2O, drying, and coating with gold. The specimens were examined by FE-SEM at an acceleration voltage of 10 kV.
To analyze the cell adherence efficiency for the scaffoldheparin-bFGF, USCs (1×104 cells) were seeded on the scaffold (6 mm diameter, 0.4 mm thickness) and incubated overnight at 37℃ and 50 rpm. After one day, the scaffolds were treated with DNA lysis buffer consisting of 0.1% sodium dodecyl sulfate (SDS, v/v), 1 mM ethylenediaminetetraacetic acid (EDTA), and 100 mM Tris-HCl (pH 7.4). The unmodified scaffold (not loaded with bFGF) was used as a control. Samples were frozen and thawed repeatedly, and then incubated overnight. Total DNA in the samples was measured using a fluorescent DNA quantitation kit (Bio-Rad, Richmond, VA, USA), according to the manufacturer's instructions. DNA concentration measurements were confirmed using confocal microscopy (Axio Observer. Z1, Carl Zeiss).
To measure cell viability and proliferation, 5×103 cells were seeded on the scaffolds (10 mm diameter, 0.4 mm thickness), and a CCK-8 assay (Dojindo, Tokyo, Japan) was performed, according to the manufacturer's instructions. The unmodified scaffold was used as a control. For myogenic differentiation, USCs were seeded on the scaffoldheparin-bFGF in Dulbecco's modified Eagle medium (DMEM) containing non-essential amino acids, glutamine, and 15% fetal bovine serum (FBS, Gibco-Invitrogen). At approximately 95% confluence, 3 µM 5-aza-2'-deoxycytidine (Sigma-Aldrich) and 5 ng/mL of transforming growth factor β (TGF-β, Peprotech) were added to the culture medium for 24 hr and the cells were cultured up to 14 days. For urothelial cell differentiation, USCs were cultured with supernatant medium collected from human bladder urothelial cell cultures (Lonza, Walkersville, MD, USA) and cultured for 14 days.
Flow cytometric evaluation of cells (passage 3) was performed for mesenchymal stem cell markers (CD44, CD90, and CD105), smooth muscle cell markers (α-SM actin, Capponin I), and urothelium markers (pan-CK, CK19) (BD Biosciences, San Jose, CA, USA), according to the manufacturer's instructions. For real-time PCR, total RNA was extracted with an RNeasy kit (Qiagen, Hilden, Germany), according to the manufacturer's instructions. A total of 2 µg of RNA was used for cDNA synthesis using cDNA Reverse Transcription kits (Applied Biosystems, Warrington, UK). The primers were designed with Primer Express Software (Applied Biosystems), and were listed in Table 1. To analyze the data, the 2-△△Ct method of relative quantification was adapted to estimate the copy numbers.
Urodynamic study, histology, and immunohistochemistry of reconstructed bladders
Twenty-five rats were divided to 5 groups: 1) control group, sham operated; 2) partial cystectomy group, approximately 40% defect was created in the dome of the bladder wall; 3) scaffold group, the unmodified scaffold was attached after partial cystectomy; 4) scaffoldheparin-bFGF group, the heparin-immobilized bFGF-loaded scaffold was attached after partial cystectomy; and 5) USC-scaffoldheparin-bFGF group, scaffoldheparin-bFGF combined with 1×104 USCs was attached after partial cystectomy. The single-layer scaffold (disk form, diameter 6 mm) was sutured as a patch onto the defect of the bladder with 7-0 Vicryl sutures. Omentum was loosely wrapped over the graft and fixed with fibrin glue (Greenplast, Greencross, Seoul, Korea) (Fig. 1B).
An urodynamic study (filling cystometry) was performed on 5 animals from each group, at 8 weeks post-operation. Two animals with bladder calculi (scaffold group; n=1, scaffoldheparin-bFGF; n=1) were excluded from the urodynamic data collection. The bladder was filled with PBS, and maximal capacity was defined as the volume of infusion that triggered the first leakage of urine. Compliance was defined as maximal capacity/(pressure which triggered the first leakage) - (baseline pressure). Then, the entire bladder was removed, fixed in formalin, and the cross-sectional area of bladders divided in half was measured using ImageJ (http://imagej.net/). The bladder samples were embedded in paraffin and cut into 5 µm sec-tions that were stained using hematoxylin and eosin (H&E) and for immunohistochemical (IHC) staining. The regenerated smooth muscle and urothelial cell layers were identified by α-SM actin and pan-cytokeratin antibodies (Sigma-Aldrich), immune reaction was analyzed with cytotoxic T cell marker (CD8), and seeded human USCs on the scaffold were detected with human nuclei-specific antibody (HuNu, BD Biosciences).
Statistical analysis
All experiments were performed at least in triplicate on separate days. A t-test and a one-way analysis of variance (ANOVA) of Tukey's test were used for statistical analysis. All values are expressed as the mean±SD. Results are representative of at least three experiments.
Ethics statement
The study protocol using the cells from human urine was reviewed and approved by the institutional review board of Kyungpook National University Hospital (IRB No. KNUH 2012-10-018). Informed consent was obtained from the patient regarding urine sampling and use of cells. All experimental procedures using rats were reviewed and approved by the institutional animal care and use committee of Yeungnam University College of Medicine (YUMC-AEC2013-003).
RESULTS
Characteristics of the heparin-immobilized scaffold
Fig. 1A illustrates the procedures followed to functionalize the scaffold surface with primary amine groups and the subsequent heparin immobilization, followed by bFGF loading. The carboxylic acids exposed on the surface were used to produce surface amine groups, and the heparin was immobilized to the surface via covalent conjugation (22). A toluidine blue assay was used to determine the amount of immobilized heparin, which was shown to be 0.72±0.11 µg/6 mm2 (Fig. 2A). The fabricated scaffold had different sized pores on the surface at front and rear side, small and large; the pore sizes were -100 and -200 µm, respectively, and the heparin distribution was homogeneous when visualized with FITC-conjugated heparin (Fig. 2B).
Affinity and release of loaded bFGF
The amount of bFGF loaded into the scaffoldheparin-bFGF at days 1, 3, 7, 14, 21, and 28 was 33.68±0.29, 32.80±0.39, 30.39±0.33, 27.31±0.25, 25.67±0.24, and 26.03±0.30 pg/mL, and for the heparin unmodified scaffold was 25.02±0.29, 24.49±0.07, 25.14±0.40, 24.19±0.23, 23.89±0.12, and 24.19±0.30 pg/mL, respectively (Fig. 2C). The initial concentration of bFGF on the heparin-immobilized scaffold revealed a high affinity and time-dependent release compared to the unmodified scaffold, and from day 21, the bFGF concentration became a basal level around 25.0 pg/mL. The unmodified scaffold showed rare affinity for bFGF, which means that heparin acts an effective liker to load of bFGF on the scaffold.
Scaffoldheparin-bFGF morphology and biocompatibility
The scaffolds exhibited a well-fabricated fibrous and porous structure, with large surface area (Fig. 2D). The pores had an average diameter of 50.8±8.4 µm. Analysis of cell adhesion based on DNA concentration showed that adhesion to the scaffoldheparin-bFGF was significantly higher than to the other surfaces (Fig. 2E). After culturing the cells for periods of 3, 6, 12, and 24 hr and 1, 3, 5, and 7 days, the viability and proliferation of USCs showed more viable cells present on the scaffoldheparin-bFGF (Fig. 2F); from day 3 of the culture, the absorbance value was significantly higher for the scaffoldheparin-bFGF than that of the other surfaces.
Differentiation into smooth muscle and urothelial cells on the scaffoldheparin-bFGF
When USCs were cultured on the scaffoldheparin-bFGF with smooth muscle and urothelium induction media, the cells were shown to express smooth muscle and urothelium surface markers at day 14 (Fig. 3A). The number of α-SM actin, Caponin I, pan-CK, and CK19-positive cells increased by 3.04, 2.20, 1.84, and 2.73 times, respectively, while, mesenchymal stem cell markers for CD44, CD90, and CD105 decreased by 0.63, 0.65, and 0.36 times, respectively.
The FACS results were confirmed with gene analysis through real-time PCR (Fig. 3B). At day 14 of differentiation, the cells exhibited significantly reduced expression of stem cell markers Oct4, SSEA4, Nanog, ALP, and c-Kit, while, markers indicative of smooth muscle cell (Pax7, MyoD, Desmin, Myosin, and α-SM actin) and urothelium cell (UP1a, UP1b, UP2, Ck7, Ck13, Ck18, Ck19, and pan-CK) differentiation were significantly increased.
Urodynamic study, histology, and immunohistochemistry
All rats for the in vivo study survived until the scheduled time of sacrifice, and there was no significant change in body weight or anastomosis problems observed during the experiment. The maximal bladder capacity and compliance at 8 weeks post operation was 2.60±0.23 mL and 56.14±9.00 µL/cm H2O for the control group, 1.46±0.18 mL and 34.27±4.42 µL/cm H2O for the partial cystectomy group, 1.76±0.22 mL and 35.62±6.69 µL/cm H2O for the scaffold group, 1.92±0.29 mL and 40.74±7.88 µL/cm H2O for the scaffoldheparin-bFGF group, and 2.34±0.25 mL and 55.09±11.81 µL/cm H2O for the USC-scaffoldheparin-bFGF group (Table 2).
There was no diverticulum on the implanted portions for any group, which were covered on the outer surface by connective tissue, and 2 animals (scaffold group; n=1, scaffoldheparin-bFGF group; n=1) were observed to have bladder calculi formation. Gross image analysis showed that the USC-scaffold combination resulted in a reconstructed bladder with better shape and volume. The mean cross-sectional area of the reconstructed bladders were 16.85±1.21, 7.87±1.37, 9.67±0.87, 11.19±0.87, and 15.71±1.34 mm2 for the control, partial cystectomy, scaffold, scaffoldheparin-bFGF, and USC-scaffoldheparin-bFGF groups, respectively (Table 2) (Fig. 4A).
H&E and IHC analysis (Fig. 4B) showed that the USC-scaffoldheparin-bFGF group exhibited pronounced, well-differentiated, and organized smooth muscle bundle formation, while other groups exhibited thin muscle layer regeneration consisting of fibroblasts and connective tissue. With regard to the urothelium, a multi-layered and pan-cytokeratin-positive urothelium was observed at the reconstructed area for most of the groups, except for the scaffold group. The condensation of submucosal area was notably high in the USC-scaffoldheparin-bFGF. The scaffold group showed enhanced CD8 lymphocyte accumulation, while the USC-scaffoldheparin-bFGF showed scant accumulation of CD8-positive cells. The seeded human USCs were not detected at the USC-scaffoldheparin-bFGF group at week 8.
DISCUSSION
Current research suggests that the use of biomaterial based scaffolds seeded with autologous urothelial and smooth muscle cells is the best option for bladder tissue engineering (23). But, biomaterial based scaffolds lead to a number of complications, and autologous cells are often difficult to obtain. Therefore, we investigated the synergistic effect of a combination of USCs and heparin-immobilized bFGF-loaded scaffolds. This approach would provide development of novel composite biomaterial based scaffold and cell source.
Previously, we fabricated a scaffold containing BSM that we reported to have amine groups on the surface (12), and heparin was covalently immobilized to the exposed amine groups on the scaffold surface. Heparin is a highly sulfated glycosaminoglycan, which has binding affinity and activity maintaining of various growth factors (24). Because of these specific interactions with growth factors, heparin has been widely used in fabrication of bioactive matrices for growth factor delivery (2526), and thus, we attempted bFGF-loading of our scaffold via heparin-immobilization. Comparison of a scaffold without surface modification to a heparin-immobilized scaffold showed higher bFGF loading for the modified scaffold, which was attributed to the ionic interactions that occurred between the positively charged bFGF protein (at physiological pH) and negatively charged heparin (2728). The observed sustained release pattern for the scaffoldheparin-bFGF was also likely caused by specifically bound bFGF on the heparin-immobilized surface (14).
In addition to a biocompatible scaffold, an appropriate cell source is also an essential requirement for tissue regeneration. USCs may play an important role in experimental research for urological organ regeneration and other urological-based applications, as they represent an optimal source due to their capacity for differentiation to myogenic and urothelial lineages (16). In the present study, the heparin-immobilized bFGF-loaded surface supported USC behavior, including attachment, viability, proliferation, and differentiation. To analyze the effects of the scaffoldheparin-bFGF on cell viability and proliferation, USCs were cultured with the two different types of scaffolds. The proliferation of USCs cultured on the scaffoldheparin-bFGF was significantly higher than on the unmodified scaffold. In addition, the USC-scaffoldheparin-bFGF was shown to enhance myogenic and urothelial differentiation rates, indicating that the scaffoldheparin-bFGF provides a suitable microenvironment for cell culture because bFGF promotes mesenchymal cell proliferation (29) and induces extracellular matrix production (13), which may improve the local microenvironment for supporting implanted cell proliferation and differentiation.
For the in vivo bladder regeneration study, the USC-scaffoldheparin-bFGF, scaffoldheparin-bFGF, and unmodified scaffold were implanted into the partially cystectomized bladders of rats to evaluate their potential for bladder tissue reconstruction. The images of the bladder specimens after dissection showed that the implanted scaffolds were attached in the bladder and covered with fibrous tissue. For the unmodified scaffold, the thick fibrous mass remained, and no expansion of the bladder volume was observed. The USC-scaffoldheparin-bFGF exhibited a thin fibrous mass and expanded bladder volume, which are indicative of bladder reconstruction. The scaffoldheparin-bFGF (without cells) yielded only a moderate result. The observed fibrous mass can also be used as an indicator of the inflammation caused by the scaffold, as previously described in a study reporting that fibrous tissue showed infiltration of neutrophils and macrophages (30). IHC analysis with the CD8 antibody showed that the unmodified scaffold exhibited an enhanced positive signal when compared to the other groups, indicating that the unmodified scaffold causes chronic inflammation, and surface modification and USCs could reduce this pathologic phenomenon.
The implanted scaffolds were not visible in the tissue sections because they were dissolved during the specimen-processing step using xylene. The histological features of the implanted grafts showed that the regenerated portions of the bladders in the USC-scaffoldheparin-bFGF group exhibited pronounced smooth muscle bundles, a multi-layered urothelium, condensed submucosa layer formation, and restored bladder volume. These anatomical reconstructions are essential for functional compliance. Other scaffold groups, however, showed only weak smooth muscle cell bundles, a thin urothelium, and loose submucosa regeneration at the graft. These results suggest that the seeded USCs contributed to the tissue regeneration. While the seeded cells were expected to survive for 2 weeks in vivo (31), we observed that the exogenous cells introduced in vivo were effective for bladder regeneration in comparison to the cells recruited from surrounding host tissues or circulating blood flow. The USC regenerative mechanism was not specifically identified in this paper, however, based on previous reports, it is presumed to result from the paracrine effects of tropic factors secreted from the USCs (31). Thus, the transplanted stem cells influenced the surrounding host cells, resulting in improved cell migration and differentiation into target cells.
In conclusion, the heparin-immobilized bFGF-loaded scaffold exhibits enhanced biocompatibility, and USCs seeded on the scaffoldheparin-bFGF induces a synergistic effect, as indicated by increased bladder capacity, compliance, and histological tissue reconstruction signified by smooth muscle, urothelium, submucosa layer regeneration, and reduced inflammation, in a partial cystectomy rat model. Therefore, we propose that USC-scaffoldheparin-bFGF would be an ideal strategy for bladder reconstruction.






 XML Download
XML Download