

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Glioblastoma multiforme (GBM), the most common and aggressive primary intracranial malignant neoplasm, presents with a dismal prognosis: a median overall survival (OS) of 15 months and a median progression-free survival (PFS) of 7 months. Despite various treatment modalities such as surgery, chemotherapy, and radiotherapy, most of patients diagnosed with primary GBMs die within 2 yr even in the most favorable situations (123).
In 2005, Stupp et al. reported the results of the first prospective multi-institutional randomized controlled trial of concurrent chemoradiotherapy (CCRT) temozolomide followed by adjuvant chemotherapy with temozolomide against primary GBMs, a treatment that prolonged the OS and PFS of patients compared to those of the previous standard treatment (radiotherapy alone) (4). Since the report, surgery followed by CCRT with temozolomide and adjuvant chemotherapy with temozolomide has been recognized as the primary treatment for newly diagnosed glioblastoma and temozolomide has been recognized as an essential chemotherapeutic drug for primary GBM treatment.
The protocol of Stupp et al. has been used by the authors since July 2004 and has been accepted as a standard protocol in Korea since September 2006 with the government insurance system covering the procedure for newly diagnosed GBM patients (4567). As this study shows the longest period of use and follow up in Korea, we report the outcome of CCRT and adjuvant chemotherapy with temozolomide in primary GBM patients at a single center for reappraisal of its effectiveness and safety.
MATERIALS AND METHODS
Patients and treatment protocols
A total of 145 patients were identified to have the age over 17 yr with a newly diagnosed, pathology-proven supratentorial GBM and complete clinical and radiological follow-up data. Among these patients, there were 71 patients who started postoperative treatment with the Stupp's protocol (CCRT and adjuvant chemotherapy with temozolomide) between 2004 and 2011. The patients received fractionated focal irradiation in daily fractions of 2 Gy, given 5 days per week for 6 weeks for a total of 61.2 Gy, with continuous daily temozolomide (75 mg/m2/day, 7 days per week from the first to the last day of radiotherapy) for no longer than 49 days. After a 4-week break, 6 cycles of adjuvant temozolomide (150-200 mg/m2 for 5 days during each 28-day cycle) were administered.
Evaluations
The baseline evaluations included a detailed patient history, physical and neurological examinations, Karnofsky Performance Scale (KPS) determination, hematological and serological evaluations, and brain magnetic resonance (MR) images. The extent of resection and tumor progression were evaluated using a serial of MR images taken within 72 hr after surgery, 4 weeks after CCRT with temozolomide, at the 3rd and 6th cycles of adjuvant chemotherapy, and every 3 to 4 months thereafter. Gross total removal (GTR) was defined as >99% removal of the initial tumor, subtotal removal (STR) was defined as 50%-99%, and partial removal (PAR) was defined as <50%.
Tumor progression was defined as not less than a 25% increase in the maximal tumor area, the appearance of new lesions, and an increased corticosteroid need as previously reported (89). When tumor progression occurred, the patients were managed at the discretion of the surgeon and then second-line treatment protocol was continued. The patient's response to the treatment was categorized into four groups using the modified WHO criteria as follows: complete remission (CR), partial remission (PR), stable disease (SD), and progressive disease (PD) (1011).
The toxic effects of the treatment were graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events (version 3.0), with a score of 1 indicating mild adverse effects, a score of 2 indicating moderate adverse effects, a score of 3 indicating severe adverse effects, a score of 4 indicating life-threatening adverse effects, and a score of 5 denoting death related to adverse effects.
The methylation status of the O6-methylguanine-DNA methyltransferase (MGMT) promoter was evaluated using methylation-specific polymerase chain reaction. The primary endpoint was OS, and the secondary endpoints were PFS and safety. OS was measured from the date of diagnosis to the date of death or the last follow-up examination. PFS was defined as the time from diagnosis to documented disease progression or death from any cause, whichever occurred first.
Statistical analysis
OS and PFS were estimated using the Kaplan-Meier survival analysis method. Differences with regard to survival and disease progression were tested for significance using the two-sided log rank test. All of these analyses were performed using the SPSS statistical software package (release 17.0.1, 2008; SPSS, Chicago, IL, USA). The toxicities of temozolomide were reported separately for the radiotherapy period and the adjuvant chemotherapy period.
RESULTS
Patient characteristics and delivery of treatments
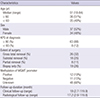
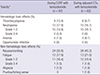
Among the 145 patients newly diagnosed with GBM from July 2004 to December 2011, 71 patients (49%) consisted of 37 male and 34 female were identified according to aforementioned inclusion criteria. Their characteristics and treatments are summarized in Tables 1 and 2. At diagnosis, 63 patients (88%) and 8 patients (12%) had a KPS score of ≥80 and <80, respectively. In total, 26 patients (32%) underwent GTR, 18 patients (25%) underwent STR, 8 patients (11%) underwent PAR and biopsy only was performed in 19 patients (26%). The methylation status of the MGMT promoter was positive in 19 patients (27%), negative in 26 patients (37%) and unknown in 26 patients (36%). The median clinical and radiological follow-up duration were 19 months (range, 2.7-119.9) and 17.2 months (range, 2.9-119.8), respectively.
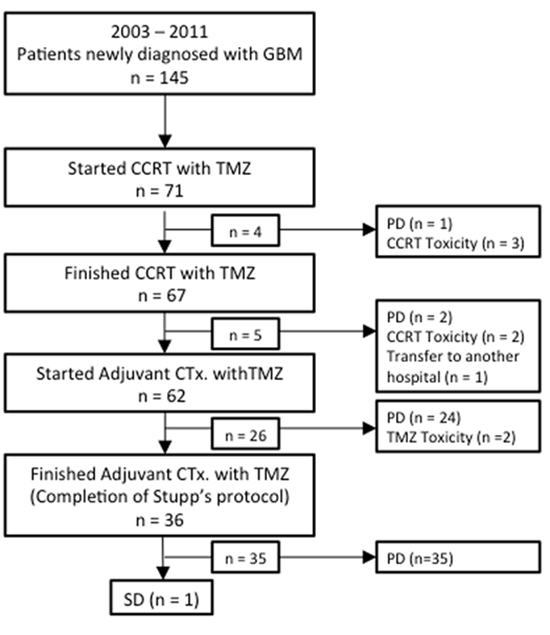
Out of the 71 enrolled patients, CCRT with temozolomide was completed in 67 patients (94%). It was discontinued in 4 patients, due to PD in one patient, and due to CCRT-associated toxicity in 3 patients during the CCRT period. During the break between CCRT and adjuvant temozolomide treatment, it was discontinued in 5 patients in which 2 patients showed PD, 2 patients developed toxicity due to CCRT with temozolomide and 1 patient moved to another hospital. Among total of 62 patients (87%) who started adjuvant chemotherapy, it was discontinued in 26 patients in which 24 and 2 patients showed PD and toxicity, respectively. Consequently, 36 patients (51%) completed the 6 cycles of adjuvant temozolomide chemotherapy, and 7 patients (10%) received more than 6 cycles. 35 among 36 patients eventually had PD. The median duration of CCRT was 47 days (range, 22-105) and the median number of cycles of adjuvant temozolomide chemotherapy was 5 (range, 1-15) (Fig. 1). There was no dose reduction in temozolomide or radiation throughout the entire study.
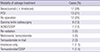
Among the 71 patients, 62 patients showed PD by the end of CCRT and adjuvant therapy with temozolomide. After recurrence, 21 patients received no further treatment and 41 patients received salvage treatment. Various salvage treatment modalities were used, including bevacizumab (±irinotecan), procarbazine/lomustine/vincristine (PCV), re-operation, gamma knife radiosurgery, nimustine/cisplatin, re-radiation, metronomic temozolomide protocol, retrial of temozolomide, Irinotecan only and temozolomide/cisplatin depending on the temozolomide responsiveness, surgical accessibility, and the socioeconomic status of the patients (Table 3). Surgery was the treatment of choice; however, for patients not eligible for surgery, bevacizumab, PCV and retrial temozolomide were the three major treatments used. Each patient was administered 1 to 5 treatments for a total of 61 treatments.
Survival and progression
The response to CCRT adjuvant chemotherapy with temozolomide followed by salvage treatment was CR in 12 (17%), PR in 17 (24%), SD in 28 (39%), and PD in 14 (20%) patients. The median OS was 22.6 months (range, 15.3-29.9). The OS at 12 months and 24 months was 80.2% (range, 70.6-89.8) and 47.1% (range, 29.8-60.3), respectively. The median PFS was 8.8 months (range, 8.1-9.5), and the PFS at 12 months and 24 months was 34.0% (range, 22.6-45.4) and 10.6% (3.0-18.4), respectively.
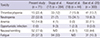
Prognostic factors, including the age at diagnosis, sex, tumor location, preoperative KPS, postoperative KPS, extent of surgical resection and MGMT promoter methylation were analyzed in these patients. Among these factors, the only significant OS and PFS prognostic factor was the extent of surgical resection. The median OS and PFS of the GTR group (21.7 and 11.0 months respectively) were longer than those of the STR, PAR and biopsy group; this difference was statistically significant in OS analysis (hazard ratio, 2.09; 95% CI, 1.003-4.353) but not in PFS analysis. The PFS and OS values are summarized in Table 4, and the Kaplan-Meier survival curves of the patients with newly diagnosed GBMs are illustrated in Fig. 2.
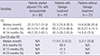
In addition to general OS and PFS of the all the 71 patients, the OS and PFS of 41 patients who had salvage treatment were analyzed separately. The median OS of the salvage treatment group was 23.3 months (range, 16.9-28.3) compared to 14.6 months (range, 8.86-20.4) in the 21 patients who did not receive salvage treatment. But due to the discrepancy in the number of patients, the difference of OS in the two groups proved to be statistically insignificant (Fig. 3). The mean duration of survival after PD in salvage treatment group was 11.9 months (1.3-53.2), which was twice as long as that of the non-salvage treatment group (5.2 months, 1-23.8). And the 6 month-, 12 month-, 24 month-survival rate were 68.3%, 41.5%, and 17.1%, respectively. In the same group, the median PFS after salvage treatment was 3.5 months (range, 2.5-4.5), and the 6 month- and 12 month-survival rate were 36.6% and 17.1%, respectively. The median OS after salvage treatment of patients who received salvage treatment was 11.9 months (range, 1.3-53.2) (Table 5).
Toxicity
The adverse events were analyzed distinctly for the periods of CCRT and adjuvant therapy with temozolomide. During the CCRT, 9 patients presented with thrombocytopenia, 12 presented with neutropenia, and 5 presented with anemia. Among the 12 patients showing neutropenia, 2 were above grade 2. During adjuvant therapy with temozolomide, 6 patients presented with thrombocytopenia, 10 presented with neutropenia and 5 presented with anemia. There were no opportunistic infections during either CCRT or adjuvant therapy. Most of the toxicities were under grade 2, and non-hematologic toxic effects such as nausea and vomiting were easily resolved with 5-HT3 receptor antagonists. The distribution of toxicities related to the CCRT and adjuvant therapy with temozolomide is shown in Table 6.
DISCUSSION
Temozolomide is a second-generation oral alkylating agent that methylates the guanine residues of tumor cell DNA, creating a mismatch that an enzyme repair system cannot fix (31213). In recent years, its antitumor activity in the treatment of malignant gliomas has been demonstrated, and temozolomide has been approved for the treatment of newly diagnosed GBMs and recurrent malignant gliomas (81014151617). In 2005, Stupp et al. reported a randomized prospective study showing that CCRT with temozolomide was more effective than radiotherapy alone in patients with newly diagnosed and histopathologically confirmed GBM. Since this report, most Korean institutions have started using CCRT with temozolomide as the standard protocol for primary GBM, and some single center and multicenter studies have reported treatment outcomes in Korean patients. As this study includes the longest period of use and follow up in Korea, we report the outcome of CCRT and adjuvant chemotherapy with temozolomide in primary GBM patients at a single center for reappraisal of its effectiveness and safety.
The percentage of patients who completed CCRT (94%) and adjuvant chemotherapy (51%) with temozolomide was similar to those of Stupp's study (85% and 47%, respectively) and the previous Korean multicenter study (93% and 52%, respectively) (613). This shows that the frequency of toxicities or disease progression during CCRT with temozolomide or adjuvant temozolomide chemotherapy is consistent.
Notably, the results of our study (median OS and PFS, 22.6 and 8.8 months, respectively) were more favorable than those of Stupp's study (median OS and PFS, 14.6 and 5.0 months, respectively) (617). The median OS of non-salvage treatment group (14.6 months) was very similar to total OS in Stupp's study. Thus the favorable result of whole enrolled patients seems to be arising from the increased OS (median OS, 23.3 months) of the salvage treatment group although it was not statistically insignificant. Unfortunately, this study revealed that prognostic factors including age, KPS score, and MGMT promoter methylation status, were not significant prognostic factors. The only statistically significant prognostic factor in this study was the extent of surgical resection. In regards of MGMT promotor methylation variable, this is probably because MGMT promoter methylation was hardly investigated in the early period of treatment that the case number is still insufficient to prove the statistical significance of the methylation state of MGMT promotor. To reach a definitive conclusion, future studies should include additional data regarding biological factors, such as methylation of the MGMT promoter, for all or most of the studied patient.
The toxicities in this study were similar to the toxicities of previous studies but differed in numbers (Table 7) (171819). The most common toxicity was nausea or vomiting (77.6%), followed by fatigue (37.3%). This is consistent with a previous study on the toxicity profile of temozolomide in Korean patients by Bae et al. (20). Overall, hematologic toxicities such as thrombocytopenia (22.4%), neutropenia (32.8%) or anemia (14.9%) were more common than in Bae's study (13.7%, 6.3%, 11%, respectively), most likely due to the smaller size of this study. Not any cases of opportunistic infections in this study seem to result from the same reason.
There are several limitations in this study. Direct comparison of a single center retrospective trial with multicenter randomized trials would be inappropriate because single-center studies tend to yield better results due to various factors including differences in study design and patient demographics (21). And the case number might be still not enough to statistically prove the effects of the well-known variables like KPS and salvage treatment. But giving certain significance to this data for its long-term period of use and follow-up, we can suggest that an active salvage treatment policy after recurrence may positively affect the survival outcome (92223). Further studies are needed to improve treatment results and minimize toxicity with this protocol.
In conclusion, the results of our study show that the current protocol of CCRT and adjuvant therapy using temozolomide may be both effective and safe and may be still appropriate as the standard protocol for GBM. After the progression of GBM, an active salvage treatment may help achieve a better prognosis with survival. Further research is needed to develop new, more efficient protocols involving the use of various antitumor agents in combination with temozolomide.





 XML Download
XML Download