

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Acute bronchitis is one of the most common illnesses in outpatient settings, and its annual incidence is about 5% among adults (1). Currently, viruses are the most common cause, and the illness is usually self-limited (2). However, the etiology is still poorly established and many patients are treated with antibiotics (3).
To date, although bacterial pathogens commonly implicated in community-acquired pneumonia (CAP) have been isolated from patients with acute bronchitis, there is no strong evidence to support their role in the pathogenesis of acute bronchitis (123). However, several atypical organisms including Bordetella pertussis have received considerable attention as important pathogens for acute bronchitis (45). In particular, Mycoplasma pneumoniae and Chlamydophila pneumoniae are associated with prolonged cough illness and outbreaks in young adults (67). Therefore, if such patients are identified and treated early, we might be able to expect some beneficial effect.
Evidence of beneficial effects of antibiotic treatments in acute bronchitis is still limited. A systematic review demonstrated that antibiotics did not influence the natural history of the symptoms, and any minor benefits were offset by their side effects (8). Macfarlane et al. (1) showed that antibiotic treatments or the presence of bacterial pathogens were not related to revisits to clinics. However, on contrary, several authors demonstrated that bacterial pathogens were more frequently isolated than viruses, and in clinical practice, more than 60%-70% of patients with acute bronchitis receive antibiotics (9).
To investigate the incidence of atypical pathogens in acute bronchitis, we performed a prospective, multi-center study in an outpatient setting. We used multiplex real-time polymerase chain reaction (RT-PCR), which facilitates the rapid and simultaneous detection of several pathogens, especially strains that are difficult to culture using standard methods (10). We also investigated the pattern of antibiotic prescription by participating physicians.
MATERIALS AND METHODS
Study population
This study was conducted during two periods (March-June and October-November 2013) at 22 hospitals (17 primary care clinics and 5 university hospitals) in Korea. Inclusion criteria were outpatients aged ≥18 yr who were previously healthy (or in a well-controlled state if the patient had a chronic lung disease), had an acute illness with a new cough and sputum, and had a duration of illness of 30 days or less. Exclusion criteria included a history of antibiotic treatment within 5 days before visiting the hospitals, a symptom duration of >30 days, a fever (>38.0℃), an acute exacerbation of chronic airway disease (e.g., bronchial asthma, chronic obstructive lung disease, or bronchiectasis), immunocompromised status (e.g., AIDS, leukemia, aplastic anemia, organ transplant, autoimmune diseases, or chemotherapy), pneumonia proven by chest radiography, or a confirmed alternative cause for cough illness (e.g., allergic rhinitis, acute pharyngitis, sinusitis, or gastro-esophageal reflux). When a patient had a focal sign (i.e., crackle) or was suspected to have pneumonia by the physician, the patient was defined as having "probable pneumonia" and was not included in the main analyses.
Data collection
Clinical information was collected by the participating investigators at outpatient departments. Data on age, sex, chronic respiratory diseases, comorbidities, history of smoking, cough (and sputum) duration, and other respiratory symptoms were collected. In addition, we investigated the nature of the cough (i.e., paroxysms, inspiratory whooping, or post-tussive vomiting) and the characteristics of sputum. We conducted multiplex RT-PCR tests for five atypical pathogens (M. pneumoniae, C. pneumoniae, Legionella pneumophila, B. pertussis, and B. parapertussis). Sputum specimens were collected and transferred at room temperature to a central laboratory (Seegene Medical Institute) and plated on culture media within 24 hr. In addition, we investigated the antibiotic prescriptions (i.e., beta-lactams, quinolones, macrolides, and others) by the participating physicians at the outpatient departments. The selection and prescription of antibiotics were at the physicians' discretion.
RT-PCR for atypical organisms
An Anyplex™ II RB5 detection kit was used to detect the five bacteria (1011). The assay was performed according to the manufacturer's instructions. PCR was performed with a CFX96™ real-time PCR detection system (Bio-Rad, Hercules, CA, USA) under the following conditions: denaturation at 95℃ for 15 min; 50 cycles at 95℃ for 30 sec; 60℃ for 1 min; and 72℃ for 30 sec. After reaction, Catcher Melting Temperature Analysis (CMTA) was performed at three PCR cyclic points (30, 40, and 50 cycles) by cooling the reaction mixture to 55℃, holding at 55℃ for 30 sec, and heating from 55℃ to 85℃. The fluorescence was measured continuously during the temperature rise. The melting peaks were derived from the initial fluorescence (F) versus temperature (T) curves by plotting the negative derivative of fluorescence over temperature versus temperature (-dF/dT vs. T). Table 1 shows the melting temperature for each target. The melting-temperature analysis was done by Seegene viewer software (11).
Data analyses
The primary outcomes were the prevalence of atypical organisms isolated from adults with acute bronchitis. Secondary outcomes were as follows: significant factors associated with positive results for atypical organisms, the frequency of antibiotic use, and factors associated with antibiotic prescription.
Data are expressed as means±standard deviations (or medians and interquartile ranges [IQRs]) for continuous variables and as percentages for categorical variables, unless otherwise indicated. Student's t-test was performed for continuous data, whereas chi-square or Fisher's exact tests were used for categorical data. A multivariate analysis by logistic regression was performed with covariates significant in univariate analysis. All reported P values were two-sided, and P<0.05 indicated statistical significance. All analyses were conducted using SPSS statistical software (IBM SPSS Statistics version 21, Standard for Medical Network).
Ethics statement
All patients provided written informed consent, and the protocol of this study was approved by the institutional review board of Hallym University Sacred Heart Hospital (IRB No. 2013-S009) and each participating hospital. The authors assert that all procedures contributing to this work comply with the Helsinki Declaration of 1975 and its later amendments.
RESULTS
Demographics and clinical symptoms
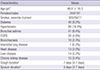
Among the 536 patients that were initially enrolled, 26 were excluded due to incomplete clinical data, and 435 were diagnosed as having acute bronchitis (vs. probable pneumonia, n=75; Fig. 1). The mean age of the patients with acute bronchitis was 48.6±16.5 yr, and 56.1% were female (Table 2). Median cough and sputum durations were 7 days (3-7 days) and 5 days (3-7 days), respectively, and among the accompanying symptoms, rhinorrhea (41.4%), and sore throat (44.1%) were the most common (Fig. 2). Hypertension was the most common co-morbidity reported, and 14.0% of patients had a chronic airway disease (i.e., bronchial asthma or chronic obstructive pulmonary disease).
Microbiologic data and clinical characteristics
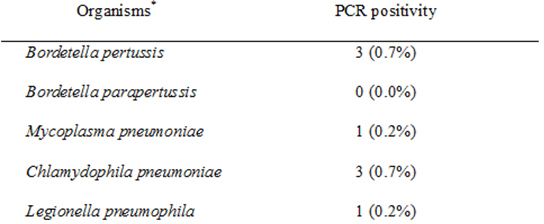
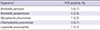
Among 435 patients with acute bronchitis, a total of 8 (1.8%) were PCR positive, and of these, C. pneumoniae (3/435) and B. pertussis (3/435) were the most common pathogens (Table 3). There were no significant differences in most symptoms and signs between patients with and without atypical organisms (data not shown). Only post-tussive vomiting was more frequent in patients with a positive PCR result than those with negative results (P=0.024). Among 75 patients with probable pneumonia, only 1 patient was positive for C. pneumoniae.
Antibiotic prescription
Antibiotic agents were prescribed in 72.2% of patients with acute bronchitis (vs. 100.0% in those with probable pneumonia) at their first visits to outpatient departments. Among the antibiotics prescribed, β-lactams were the most common (29.4%), and the proportion of patients who received quinolones (20.5%) was similar to that in those with probable pneumonia (Fig. 3).
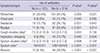
Patients with rhinorrhea, headache, chest pain, myalgia, a shorter duration of cough and/or sputum, inspiratory whooping, dark sputum, or rhonchi were more likely to receive antibiotics (Table 4); however, there were no significant differences in the prescription rate between primary care clinics and university hospitals. In multivariate analysis (Hosmer-Lemeshow test, χ2=7.128 and P=0.523), rhinorrhea, myalgia, inspiratory whooping, dark sputum, and rhonchi were independent factors for antibiotic prescription.
DISCUSSION
Our study revealed several interesting findings. First, the incidence of atypical pathogens was 1.8% in patients with acute bronchitis who presented to outpatient clinics. Second, only post-tussive vomiting was associated with atypical infection. Finally, more than 70% of patients received antibiotics at their first visits.
To date, the etiology of acute bronchitis (or acute lower respiratory tract illness) has not been well established, either due to the inadequate definition or the low microbiological yield (i.e., 20%-40%) (12). However, approximately 90% of cases of acute bronchitis are caused by viruses (e.g., rhinovirus, influenza, and parainfluenza viruses), and routine culture or serologic tests are not recommended in clinical practice (31314). Although there is no definite evidence suggesting that bacterial pathogens cause acute bronchitis in healthy adults, several atypical pathogens have received attention as causes of acute bronchitis in previous studies (215).
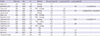
Atypical pathogens are a frequent cause of CAP, accounting for 6%-20% in ambulatory patients and ~40% in hospitalized patients (16). In particular, children and young adults are more likely to be infected by C. pneumoniae and M. pneumoniae (17), and elderly patients with cardiopulmonary comorbidities are at high risk for severe CAP caused by C. pneumoniae (18). L. pneumophila is also an important cause of severe CAP, with an incidence of 1.9%-7.9% (19). However, the incidence of these atypical organisms is much lower in patients with acute bronchitis. Some authors have also insisted that atypical pathogens have no role in acute bronchitis (3). When considering the results of previous studies conducted since 1990 (Table 5), although several studies showed an incidence of >10.0% for both M. pneumoniae and C. pneumoniae, other studies with only PCR tests showed a lower incidence for atypical pathogens in acute bronchitis (M. pneumoniae, 0.8%-4.1%; C. pneumoniae, 0.0%-2.3%). With regard to L. pneumophila, Lieberman et al. (2021) showed an incidence of 6.8% and 10.9%, respectively, in their two studies where serological tests were used, but other studies demonstrated an incidence of 0% (3142223). These low incidence rates of atypical pathogens are not much different from those of our study. Therefore, we can say that there is still a lack of evidence supporting the role of atypical pathogens in acute bronchitis.
Pertussis is a well-known infectious disease with a high attack rate. Although it is a vaccine-preventable disease, its incidence has increased substantially in adults since 1980, and a large outbreak occurred in the United States in 2012 (24). However, in Korea, there have been three prospective studies performed on adults in outpatient settings (42526). Among them, two multi-center studies, which used a PCR method, showed incidence rates of 0.5% and 6.9%, respectively. However, the rate can vary by the length of cough illness. Among adults with subacute or chronic cough illnesses (a duration of ≥3 weeks) (27), the incidence rate is 26%-31%, but among adults with acute cough illnesses, it is 7% (28). In the present study, most patients had an acute cough illness (cough duration, 3-7 days) but the incidence (i.e., 0.7%) might have been underestimated because we did not perform other methods of sampling. Nonetheless, physicians should acknowledge that pertussis can still be an important cause of acute bronchitis in non-epidemic settings.
With regard to clinical symptoms and signs, only post-tussive vomiting was associated with PCR positivity for atypical bacteria in the present study. Although this result can be partly due to patients with B. pertussis, it should be further clarified in future studies. However, atypical pathogens are often associated with persistent cough, headache, and pharyngitis (29), and C. pneumoniae infection is associated with wheezing or asthmatic bronchitis. Therefore, taking into consideration these clinical findings together might be helpful for suspecting atypical origin.
Currently, antibiotic treatment is not recommended for routine use in patients with acute bronchitis (2). A randomized controlled study and two meta-analyses demonstrated no significant beneficial effects of antibiotics in patients with acute bronchitis (303132). However, despite these results, more than 60%-70% of patients receive antibiotics at outpatient clinics (9). This may be partly because of patient expectations. A survey by Wilson et al. (33) showed that more than half of patients believed that antibiotic treatments were effective for upper respiratory infections. In the present study, although all of the physicians were aware of the current guidelines, 72.2% of patients received antibiotics. Among the antibiotics used, beta-lactams were the most frequently prescribed, and 20.5% of patients received quinolones, which are mostly broad-spectrum agents. As many physicians know, inappropriate antibiotic use can be associated with an increased risk of adverse effects, including Clostridium difficile infection and increasing antibiotic resistance (34). In contrast, interestingly, several studies have reported results in favor of the role of bacterial pathogens. Some authors demonstrated epithelial cell injury by atypical pathogens (15), and other authors showed an increasing hospitalization rate with a decreasing antibiotic prescription rate (35). In particular, Macfarlane et al. (123) demonstrated a higher incidence of bacterial pathogens than viruses, which contrasts with the results of other studies. Nonetheless, the evidences supporting antibiotic use are still limited and the current guidelines recommend against it in acute bronchitis. Our study also is in concordance with the current guidelines. Therefore, physicians need to refrain from injudicious use of antibiotics in patients with acute bronchitis without any evidence of pneumonia.
The present study has several limitations. First, we did not investigate viruses and other bacterial pathogens. This can limit the scope of our results. Second, there is a possibility that some patients with upper respiratory infections might have been included. Third, we did not use nasopharyngeal or throat swabs for sampling or serological or culture tests for identification. This could be associated with the low incidence of atypical pathogens. Fourth, although we used multiplex RT-PCR, which has high sensitivity, there is still no standardized PCR method for the detection of atypical pathogens. Finally, follow-up data were not available in the present study, which could have provided interesting results about the effectiveness of antibiotics. However, this is one of the few studies on the etiology of acute bronchitis in Korea, and our study was a prospective, multi-center one. In particular, we also found that many physicians are prescribing antibiotics for cough illnesses. This could be valuable information for future measures for antibiotic use.
In conclusion, our study demonstrates that the incidence of atypical pathogens is low in patients with acute bronchitis in an outpatient setting, and the frequency of post-tussive vomiting is high in patients with atypical infection. Importantly, the antibiotic prescription rate for acute bronchitis is still high. Therefore, physicians should take into account the low incidence of atypical pathogens and the currently high prescription rate of antibiotics in acute bronchitis.




 XML Download
XML Download