

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Endovascular aneurysm repair (EVAR) for abdominal aortic aneurysm (AAA) now becomes widely accepted as primary choice for aortic aneurysm repair. Main obstacles for this less invasive procedure lies in proximal hostile neck anatomy which leads to aneurismal exclusion failure by causing type-I endoleak (1, 2). Although distal iliac stenotic lesion causes access difficulty to deliver the system, smaller profile and lubricant sheath offers more chance to overcome this limitation (3). The other important iliac artery related issue is combined common iliac artery (CIA) aneurysm which occurred up to 20% with AAA (4). In such cases, EVAR requires distal extension to external iliac artery with occlusion of hypogastric artery to prevent type II endoleak via patent hypogastric artery.
Unfortunately, sudden blockage of the hypogastric artery caused variable degree of pelvic ischemia. Predominantly this will cause buttock claudication and erectile dysfunction, but sometimes more serious consequences such as colon ischemia or spinal cord ischemia could happen (5,6,7,8). To prevent this complication, surgical bypass to hypogastric artery via retroperitoneal approach has been performed (9). However this hybrid procedure sometimes offsets the benefit of less invasiveness of EVAR by causing complication such as retroperitoneal hematoma. The iliac branch device (IBD) (Cook Inc., Bloominton, IN, USA) introduced for pure endovascular approach. Technical success and clinical results showed feasibility with desirable outcome (10,11). However, in many countries including Korea, the commercialized IBD is not available yet. Hence we report four cases using surgeon custom made IBD which could be used for substitute technique of endovascular salvage for hypogastric artery. This is not an original concept, already many experiences have been reported in terms of branched stent graft (12). We also customized the IBD procedure to make it more cost effective.
MATERIALS AND METHODS
Device customization
IBD is created making short cuff to TFLE Zenith iliac limb (Cook Inc.). Making branch portion is done with partial proximal deployed state. For this, peel-away the system of limb needed to be removed, but to keep it in stable status, the main keeping wire should not be removed. Although the diameter of TFLE limb is fixed as 12 mm, the length of limb used for IBD will be dependent on iliac artery anatomy. This would be another benefit of custom-made devices compared to fixed length of factory ready-made devices. We used 73 mm in three cases and 56 mm in one case. First step, deploy proximal two stent (Fig. 1A). Sometimes second stent row is not fully expanded because of distal confined portion, we found that making a cuff was not hindered. To make an accurate hole for cuff, electric coagulator is used (Fig. 1B). The hole should be made at the site of stent, not between stents. We usually use a 7 mm thin walled PTFE (Gore Inc., Flagstaff, AZ, USA) graft for making cuff, but 8 mm graft also will work. The length of cuff is decided between 15 mm to 20 mm based on working distance between cuff and hypogastric artery orifice. The orientation of cuff can be decided in any direction using reference of knob at the handling portion. The configuration of cuff should be downward shaped usually 45 degree. Using 5-0 Prolene, running suture as vascular anastomosis is done (Fig. 1C). The cuff located under the stent, we put three sutures including top to fix stent with cuff. So this outside stent could offer supporting skeleton at the overlap zone. We put one gold marker at the outside of distal portion of cuff (Fig. 1D). For the proximal marker of cuff, second stent will be used as the reference. This whole "making device" procedure usually takes less than 10 min (Fig. 1E). In our first case, we made the device before operation to avoid unnecessary anesthetic time, but after that we did during the operation. For the preload catheter, it could be decided by the configuration of aortic bifurcation (Fig. 1F). For the sharp angle, Cobra 2 or RIM catheter will be proper other than we usually choose KMP catheter with Terumo 035 inch 260 cm glide wire.
Deploy procedure (Fig. 2)
The first step is to insert a large diameter sheath enough to introduce cuffed IBD, into CIA. Since the sheath size for 12 mm diameter Zenith is 14 Fr, we often choose 20 Fr, 35 cm length sheath (Saint Jude, Inc., St. Paul, MN, USA) for this purpose. Even though 5Fr angio catheter comes together for preload catheter, we found 20 Fr sheath is enough size for IBD procedure. After the tip of the sheath is located CIA orifice level, the custom-made IBD needs to be loaded. This step would be the bustle up without experiences, because of back bleeding via sheath. Variable techniques in terms of reloading procedure can be used according to operator's experiences. We use umbilical tape to confine the stent-graft to reload into sheath. This is two person's work and both should be familiar with loading procedure to avoid inadvertent injury to stent of cuff component. Since the hypogastric artery direction is always posterior, the cuff should be loaded with facing posterior, too. After introducing IBD at the level of CIA proximal site, contralateral selection to make through-through guidewire needs to be started. With proper shape of preload catheter, passing guidewire to opposite iliac artery is simple without much difficulty. However if there is severe tortuosity in contralateral external iliac artery (EIA) with sharp aortic bifurcation angle, this step would be very hard without snare. Commercial IBD devices include snare device for this purpose. However sometimes snaring also can be difficult with hairpin shape bended EIA anatomy. We do not use a snare device for this step. Instead of using preload catheter, we can do cross over guide wire first from any side of femoral artery and using this preplaced guidewire as through-through guidewire during IBD loading procedure. By avoiding snare procedure, it offers huge medical costs saving effect. This is another merit of custom-made IBD. After using this technique we could overcome any difficulties related to this step. The proper diameter sheath to introduce bridging covered stent is inserted with holding through-through guidewire. The tip should be placed beyond cuff to prevent inadvertent fall off during inserting covered stent, especially sharp aortic bifurcation angled anatomy. Before this step, proximal IBD portion needs to be deployed to cuff level. If there is limited working distance between cuff and hypogastric artery, bridging procedure would be failed or kinking could happen. So this must be kept in mind. Cannulation for hypogastric artery can be easy with proper catheter. We change to stiff guidewire to introduce covered stent. Measuring the distance between cuff and hypogastric artery is important to decide proper covered stent. Preplaced gold marker with stent row used as reference marker for this step. If there is some aneurismal change with hypogastric artery, we prefer balloon expandable stent-graft, V12 (Atrium, Inc., Hudson, NH, USA) because diameter adjustment with bigger balloon is capable. After introducing covered stent to proper site, the through-through wire needs to be removed. It will offer natural configuration of cuff to direction of hypogastric artery. Careful balloon for covered stent with proper diameter is important to prevent distal type I endoleak. After completing this procedure, the rest of IBD part will be deployed without pressure to hypogastric artery. The main body of Zenith stent graft will be introduced via contralateral side and deployed as regular EVAR procedure. To bridge the gap between contralateral limb and proximal stent of IBD, also sizing catheter introduced after contralateral gate selection. Since only 22 mm length of stent in limb graft offers overlapping zone, operator should be careful during bridging procedure. It should not cover the orifice of IBD internal opening which could lead to hypogastric artery occlusion. For this step, proper oblique C-arm angle, with caudal-cranial view is recommended.
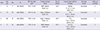
RESULTS
We have done four custom-made IBD cases. The technical success for all cases was 100%. Each step of procedure for IBD loading, hypogastric artery cannulation, bridging procedure with covered stent was done uneventfully. All iliac artery aneurysm was excluded without type I endoleak which was confirmed in early post operative CT scans. The indication of IBD were Bilateral CIAA combined with AAA in all patients (Table 1). For the bridging procedure, V12 (Atrium, Inc.) was used in three patients and one Viabahn (Gore, Inc.) was used for the other patient. In all three V12 using cases, flaring of distal V12 with bigger balloon to adjust aneurismal portion of hypogastric artery was achieved. In three patients, opposite hypogastric artery was simultaneously occluded with coil. In the other forth patient, contralateral hypogastric artery was already occluded by disease progression and single hypogastric artery was saved by IBD. The 4th patient (case 4 in Table 1) has severely angled aortoiliac anatomy and the operation was relatively challenging (Fig. 3). The acute angle over aorta and left CIA hindered the advancing of limb stent graft which offered a bridge between contralateral limb and IBD. During the pushing up of the limb stent graft, pre-deployed IBD device was moved upward, too. Since V12 was already deployed and fixed to hypogastric artery, the cuff portion of IBD could have been fallen off and lead to disconnection. To overcome this situation we have used 24 French big sheath (Cook, Inc.) to offer paving. We have used Endurant (Medtronic, Inc., Minneapolis, MN, USA) limb stent graft for flexibility.
DISCUSSION
The risk of hypogastric artery embolization during EVAR is well known but sometimes it is inevitable when AAA is combined with CIA aneurysm. The most disastrous complication such as ischemic colon necrosis reported with bilateral embolization (13). This life threatening complication needs instant abdominal exploration with bowel excision and colostomy. However even with unilateral hypogastric embolization, up to 50% of patients suffer from buttock claudication (14). Although this is not a critical complication and expected spontaneous improvement with time, many of these patients turn out to be in a disabled walking life style. Since the elective aneurysm repair is preventive surgery even without any symptom, postoperative life quality is severely affected. Surgical bypass such as hypogastric artery transposition or interposition graft could offer pelvic perfusion for such cases, but still need general anesthesia with increasing peri-operative risk to comorbid patients. There is some noble endovascular technique so called "sandwich" procedure. Separate covered stent insert to hypogastric artery in parallel configuration with main stent graft to salvage hypogastric perfusion (15). However still there is no constant consensus for this technique in terms of feasibility. Also there is high risk for endoleak through the gap between parallel covered stents, especially hostile anatomy. Iliac branch device was designed to pursue more stable procedure which could offers natural anatomic configuration. Commercial available IBD device becomes the solution for this circumstance without any more invasiveness. The clinical outcome of Cook Zenith IBD have showed prominent results with desirable longterm patency results (10). With 100 consecutive cases, the procedural success rate was 95% without mortality. The patency rate of hypogastric branch was 90% at 1 yr and 81.4% at 5 yr. There were no late ruptures. However, even with these highly acceptable results, the device availability in some countries are very limited. Because of health costs and reimbursement issues, many countries including Korea, this situation motivates vascular surgeons to customize conventional stent graft (16,17,18). Because the vascular surgeons are already getting used to manipulating graft, they have some privileges for customization such as suture cuff to iliac limb stent graft. Other authors reported using Dacron graft for cuff. We used PTFE graft to favor IBD loading into big sheath by reducing profile. Through our four cases of experiences, we found that the loading procedure is the most demanding step because of back-bleeding. The benefit of our procedural customization is revising the order of procedures and capable cross over guide wire without snare device. If the angle of aortic bifurcation is sharp with tortuous iliac arterial anatomy, crossing guide wire is not easy. Snaring is not directly related with IBD, but it is an expensive complement and another burden of medical cost. Even without snare, if the cross over guidewire is done at first and using this wire to insert preload catheter of IBD during loading procedure, hostile iliac anatomy could be surmounted. The other benefit is choosing the most proper size of IBD graft in terms of length and diameter. The size could be decided according to external iliac artery diameter and configuration. We chose the distal diameter 10 mm and the limb length 56 mm (TFLE-10-54) in three cases. This aspect offers more flexibility in case of tortuous anatomy as in our fourth case (Fig. 3). For bridging, we used balloon expandable covered stent, because of dilatation could be possible to adjust aneurismal change of hypogastric artery. There is some anatomical limitation for application of IBD procedure. The CIA lumen should be enough to allow cuff with limb stent graft which is more than 20 mm. If the lumen is smaller than this, the cuff could be compressed by arterial wall. The length of CIA is also an important factor for cross over introducing bridging covered stent. Based on configuration of limb stent graft and considering working distance for bridging, 50 mm length is the minimum requirement. Severe tortuosity of external iliac artery and acute angle between aorta and CIA could act as an obstacle for IBD, but it is not absolute contraindication. Careful planning based on CT workstation is a prerequisite with hostile anatomy as in our case. It is better to do IBD procedure in straight CIA side, because tortuous iliac artery may cause displacement of preplaced IBD during introduction of other components during EVAR.
In summary, we reported the first case of surgeon custom-made IBD in Korea. The procedure is feasible and useful to preserve pelvic perfusion especially in the situation of unavailability of device. Long-term follow-up is needed to evaluate stent graft patency and IBD-related complications.



 XML Download
XML Download