

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Despite of increment of liver transplantation (LT), there are still growing numbers of accumulated patients in waiting list in Korea. Child-Turcotte-Pugh (CTP) score-based system has been used for deceased donor allocation in LT in Korea from 2002. Even though the donation rate after brain death was still relatively low, the absolute number and the proportion of deceased donor liver transplantation (DDLT) have been increasing recently. Therefore, adequate deceased donor allocation became important issue in Korea.
Ultimate goal of allocation system is balancing between justice and utility, which means to optimize the use of scarce donor organ resource and to reduce waiting list mortality and furthermore, to maximize long-term outcome. For this purpose, the model for end-stage liver disease (MELD) score system was adopted for deceased donor allocation in February 2002 in the United States, because it is objective, readily available data and highly predictive of short term mortality, on the other hand, CTP score-based system is partly subjective and empirical (1).
MELD score was introduced for the prediction of short term mortality of patients with cirrhotic liver after transjugular intrahepatic portosystemic shunt, using serum creatinine, bilirubin, prothrombin time international normalized ratio (INR) and etiology of liver disease (2). MELD allocation system has resulted in positive effects, i.e., 12% reduction in waiting list registration especially patients with MELD score less than 10 because of the very little chance of receiving deceased donor liver (3) and 3.5% reduction in drop out number, which caused the increase in transplantation rates on the contrary. MELD score based system have settled down to some extent in the United States and many other countries but still, is on the way of refinement, i.e., MELD-Na, MELD refit, additional point for patients with hepatocellular carcinoma (HCC) and so on (4-7).
However, it is not desirable to adopt the allocation system of the Western countries without verification because the medical environment of Korea may be quite different from that of the Western countries. However, there are very few data and reports about the feasibility of MELD score-based allocation system in Korea (8-10).
The aim of this study was to investigate the feasibility of the MELD score-based system compared with the current CTP score-based system and to suggest adequate cut-off to stratify waiting list mortality among Korean population.
MATERIALS AND METHODS
Nine hundred and one patients have registered for DDLT from January 2008 to May 2011 in Seoul National University Hospital. Seven hundred and eighty eight adult patients were included for analysis after excluding 113 patients who were status 1 or younger than 18 yr old, or patients whose laboratory data were not available for calculation of MELD score.
We collected the patients' data of age, sex, the Korean Network for Organ Sharing (KONOS) status, and laboratory data retrospectively. MELD scores were calculated using values acquired by test just before registration. Values of serum total bilirubin (mg/dL), prothrombin time INR, serum creatinine (mg/dL) less than 1.0 were changed to 1.0 to avoid negative value because they should be calculated in logarithmic function. Creatinine values higher than 4.0 were changed to 4.0 according to the previously proposed protocol (5).
MELD scores were calculated according to the following formula:
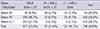
Median MELD score was 17 (range, 6-57). Patients were classified into three groups according to the MELD score, i.e., low MELD score group (MELD score<24), high MELD score group (24≤MELD score<31) and highest MELD score group (MLED score≥31). Patients were also classified as three groups according to KONOS status, i.e., 2A group, 2B group, and 3 & 7 group. KONOS classification is similar with previous UNOS classification (Table 1) (1).
Patients were observed for 6 month after registration. During follow up period, patients who underwent LT (DDLT or LDLT) or patients who were loss of follow up were considered as censored.
Statistical analysis was performed with the SPSS version 19 (SPSS, Inc., Chicago, IL, USA) and Medcalc for Windows version 12.4.0.0. (MedCalc Software, Mariakerke, Belgium). To identify adequate cut-off value, we performed c-statistics and the area under the curve (AUC) value was calculated. The short term (1, 3, and 6 months) survival was evaluated via Kaplan-Meier method according to current allocation system and MELD score. P<0.05 was defined as statistically significant.
RESULTS
Survival according to MELD score and adequate cut-off values to stratify waiting list mortality
Fig. 1A showed patient survival according to MELD score at an interval of 5 point. One month survival dropped at 30 point. And 3 month survival dropped at 25 point. According to c-statistics, the adequate cut-off value for 1-month mortality was 31 (sensitivity, 58.18; specificity, 89.50) and the area under the curve (AUC) value was 0.794 (95% CI, 0.764-0.822; P<0.001) (Fig. 1B).
The cut-off value for 3-month mortality was 24 (sensitivity, 65.22; specificity, 80.46) and AUC was 0.778 (95% CI, 0.747-0.806, P<0.001) (Fig. 1C).
We divided into three groups based on different cut-off values. Patients with higher MELD score (MELD≥31) has the lowest 1-month survival rate (65.2%, P<0.001) but the other two groups showed no difference (P=0.860) (Fig 1D). However, 3-month survival rates were significantly different between three groups.
The feasibility of MELD score-based system to predict waiting list mortality compared with the current CTP score-based system
One hundred sixty four patients were listed as Status 2A, 400 patients as Status 2B and 224 patients as Status 3 or 7 (Table 1). Among 164 patients in Status 2A, 47.6% of patients (78/164) was low MELD group (<24). However, 28.8% of patients in Status 2B (115/400) was high MELD group (≥24).
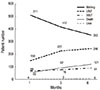
Fig. 2A shows 1, 3, and 6 month survival according to the current KONOS status. 3-months survival of Status 2A was 70.2%. However, among Status 2A patients, 82 patients with MELD <24 showed better survival (93.0% of 3-months survival) than current Status 2B group (82.3%) (Fig. 2A, B). However, patients with highest MELD score (≥31) among Status 2B group showed poorer survivals (48.2% of 3-months survival) than current Status 2A group (70.2%) (Fig. 2C).
Clinical course of the cohorts
Fig. 3 shows the clinical course of the patients for 6 months after registration under the current allocation system. Only 8.6% of patients (68/788) in the waiting list received DDLT within 1 month. The rate of DDLT was not much increased until 6 months after that 19% of the patients (150/788) received LDLT within 1 month. It was increased until 6 months. 337 (42.8%) patients underwent LT during 6 months follow-up. Among them, only 91 patients (91/337, 27.0%) underwent DDLT, and 246 patients (246/337, 73.0%) underwent LDLT. However, 353 patients (44.8%) were still in waiting list and 121 patients (15.4%) were dropped out due to death and 8 patients (1.0%) were loss of follow up during 6 months after initial registration.
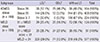
Among status 2A patients, 48.2% (79/164) received DDLT. However, only 18.5% (23/124) of highest MELD and 27.6% (24/87) of high MELD group received DDLT (Table 2).
DISCUSSION
Deceased donor allocation system has not been a major concern in Korea, because LDLT has been prevalent. Current Korean liver allocation system adopted the previous UNOS system, which utilizes CTP score-based system. However, it comprises a couple of subjective factors such as ascites and encephalopathy, therefore, it can be easily manipulated for the purpose of allocation. Furthermore, in Status 2B category, non-medical factors such as waiting time and center incentive determined the order of allocation in current Korean allocation system. As the DDLT is increasing in Korea, there is an argument that the current allocation system needs to be changed into more objective system such as MELD score-based system. Medical environment of Korea is somewhat different from the Western. Hepatitis B virus (HBV) related liver disease is more prevalent and LDLT is more prevalent. Therefore, it is necessary to evaluate the feasibility of MELD system in Korea compared with the current allocation system by analyzing Korean database.
There have been some studies about the feasibility of MELD score in Korea. However, most of them were about the prognosis after resection or prognosis of the patients with cirrhosis. Song et al. (11) showed that MELD score was better predictive factor of early mortality after resection for patients with HCC and cirrhotic liver than CTP score irrespective of etiology of cirrhosis. Kim et al. (12) also showed the MELD-Na and MELD score was superior to CTP score for prediction of early mortality for patients with cirrhosis. Hwang et al. (8) suggested the MELD system as a solution for allocation dilemma (Status 1 vs Status 2A) in cases of HBV related fulminant hepatitis. However, there have been no Korean studies about the usefulness of MELD score system for prediction of early mortality after registration for DDLT.
The definition of KONOS Status 2A is the life expectancy of 1 week or so without LT. So far, those patients of Status 2A have had priority of deceased donor liver over the patients of other status according to this definition. This study, however, did not show the early mortality corresponding to the definition. One month mortality of Status 2A patients was relatively low. Only 12.7% of patients among Status 2A patients were dead at 1 month after registration and they also showed low mortality rate 29.8%, 33.8% at 3 and 6 months respectively. Because of relatively higher incidence of LDLT in Korea, the mortality could be lower than the United States. However, compared with relatively higher mortality rate in highest MELD score (34.8% of one month mortality in MELD≥31), the one month mortality rate of current Status 2A (12.7%) is too low in contrast to the definition. The risk of mortality in Status 2B group was also relatively low compared with that of intermediate MELD score group (Fig. 2A & 1D). Therefore, current allocation system does not reflect the risk of early mortality after registration correctly. Furthermore, short term mortality can be stratified by MELD score among Status 2A group (Fig. 2B). One month mortality was 35.1% in patients with MELD score more than 31 among Status 2B, which is higher than that of general Status 2A patients (12.7%) (Fig. 2C). Thus, we might have overestimated some patients with low actual risk of mortality and we also have overlooked some patients with high actual risk of mortality in the current allocation system. Therefore, we can conclude that MELD system is better than the current allocation system to stratify the survival during waiting in Korea.
In the current system, if there is no Status 1 patient in the waiting list, deceased liver allocates to the Status 2A recipients in the same region first, and then if no candidate in the same region, it extends to whole nation before seeking Status 2B patient in the same region. In this study, we tried to find the optimal cut-off to apply this nation-wide extension policy in Status 2A if MELD system is applied. In the United States, it is 35 and 15 point (13). According to our analysis, 31 point seems appropriate to differentiate one month survival. However, 24 point seems more appropriate to differentiate 3-month survival. Furthermore, the proportion of patients (MELD≥24) group was 26.7%, which was similar with that of the current Status 2A (20.8%). Therefore, 31 and/or 24 point seemed appropriate cut-offs to differentiate allocation policy in Korea.
Optimal allocation means 'more livers to sicker patients', however, short-term post-operative mortality might be increased after this strategy. The actual short term outcome has been reported not to be changed compared with the previous outcome according to UNOS/OPTN analysis. Instead, waiting list mortality was reduced (14). There have been several efforts of validation after adoption of MELD based system in the United States (15, 16). And further studies are ongoing for refinement of MELD score-based system (4-6, 17). Biselli et al. (4) reported that MELD-Na and integrated MELD were the best prognostic models after comparing 6 score systems. Validation and modification should also be followed if MELD system is adopted in Korea.
Another issue is the exceptional situations such as HCC and hepatopulmaonary syndrome and so on in which MELD based allocation is not applicable (18-20). We need another study to identify optimal exceptional indication in Korea.
One of the limitations of this study is that we assumed that all mortality was related with hepatic failure. The non-liver failure related mortality such as HCC progression was not considered in this study. However, the tumor biology of the patients in waiting list was usually good because no additional point for HCC in the current listing rule and therefore, the reason for DDLT listing was mainly liver dysfunction in Korea.
In conclusion, MELD score-based system is better than CTP score-based system in that it uses objective data and it can predict short-term mortality better. Therefore, we expect that more number of high risk patients can receive DDLT and thus, dropout rate will be decreased by adopting MELD score-based system in Korea. The current CTP score-based system should be changed into the MELD score-based system in Korea. However, nation-wide study is needed to make concrete conclusion.


 XML Download
XML Download