

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Glomerulonephritis (GN) is the third leading cause of end stage renal disease (ESRD) in the Korean population (1). Although the incidence of GN can be dependent on the indication for renal biopsy and the medical environment (2), it ranges from 1 to 16 new cases/year/105 adult population (3, 4). GN is related to increased other cause co-morbidities and mortality. The cumulative incidence of ESRD among GN patients was 13% in 10 yr after biopsy in Denmark (5) and 17% during 17 yr after renal biopsy in Japan (6). Patients with GN had higher incidence of all vascular complications compared to the general population (5). The mortality rate in GN patients was 32% at 10 yr after biopsy, which is a higher mortality rate relative to the general population for all pathologic diagnoses (5). GN was also related to a higher incidence of malignancy (7).The incidence of cancer was markedly higher in patients with membranous nephropathy (MN) than in the general population (standardized incidence ratio of 9.8 for men and 12.3 for women) (8) and also higher in other pathologic types (9-11).
Since the mid 1990s, the renoprotective effect of the blockades of renin-angiotensin-aldosterone system (RAAS) in diabetic and non-diabetic nephropathies was reported, although argument continues about the additional effect of RAAS blockades beyond lowering blood pressure (12). As a result, RAAS blocking agents were widely applied to clinical medicine and GN treatment (13). An important meta-analysis recently published suggested that angiotensin II type 1 receptor blockers (ARB) are associated with an increased risk of new cancer diagnosis (14). Considering the wide use of ARB and the higher incidence of malignancy in patients with GN, we should confirm the relationship between ARB prescription and cancer incidence. In this study, we registered patients with renal biopsy, determined the prevalence and incidence of malignancy, mortality rate, and cancer mortality rate, and analyzed the relationship between the use of RAAS blockades and cancer incidence or mortality.
MATERIALS AND METHODS
Study subjects
The subjects who had diagnosed and been followed as glomerulonephritis by the renal biopsy were enrolled in the Progressive REnal disease and Medical Informatics and gEnomics Research (PREMIER) program sponsored by the Korean Society of Nephrology, retrospectively (13, 15, 16). Thirty-four hospitals and clinics in Korea participated in the study. We included 3,288 adult patients, who had been enrolled during August 2003 to December 2005, in the analysis.
Data
The participating researchers had selected patients with renal biopsy and one qualified nurse, who had visited every participated institution, inputted the data into the formatted database. We collected final diagnoses of renal pathology in the format of minimal change lesion (MCN), MN, focal segmental GN (FSGS), membranoproliferative GN (MPGN), IgA nephropathy (IgA), Henoch-Schölein nephritis (HSP), lupus nephritis (Lupus), Crescentic GN (Cresentic), diabetic nephropathy (DMN), and diagnosis not otherwise classified (Others). The pathologic diagnosis was decided by the pathologists in each center. We defined the user-group of medication, such as angiotensin-converting enzyme inhibitors (ACEI), ARB, and any kind of steroid and HMG-CoA reductase inhibitor if it was prescribed for more than 3 months, and started within 6 months after renal biopsy. Hypertension was defined as a reported history of hypertension, a systolic blood pressure (SBP) of 140 mmHg or more, or a diastolic blood pressure (DBP) of 90 mmHg or more. Diabetes mellitus was defined as a random glucose level 200 mg/dL or more or a reported history of diabetes. We grouped patients as no medication of ACEI or ARB (None), ACEI-only, ARB-only, and ACEI and ARB (ACEI-ARB). The estimated glomerular filtration rate (eGFR) was calculated by the modified modification of diet in renal disease equation based on the Jaffe method to measure serum creatinine (17).
The outcomes
The endpoints were the development of new cancer and death by any cancer after renal biopsy. The mortality data were obtained from Statistics Korea. The institution provided the cause of death for an individual patient until December 2006. The primary cause of death was reported by a doctor to the government in ICD-10 disease code. The incidence of cancer was obtained from the Korean National Cancer Center that has collected the data of cancer in Korea since 1980 (18). We could join the data based on the unique personal identifier which all Koreans have.
Statistical analysis
The SPSS (SPSS version 15.0, Chicago, IL, USA) package was used for statistical analysis. Differences in proportions were compared by chi-square test. Group differences for continuous variables were assessed by the Student t-test or one-way ANOVA test according to the number of groups. We compared the cumulative incidence of outcomes after renal biopsy by Log-rank test. The cancer occurrence was compared with that of the general population, taking into account of gender, age, and period of renal biopsy, and the 95% confidence interval (CI) for the observed-to-expected rate was calculated. Expected cases were calculated for each 5-yr stratum of the cohort and by gender. National estimates of overall and organ-specific cancer incidence by gender and 5-yr age group were provided by Statistics Korea. To determine whether the user of ACEI or ARB was independently related to the incidence of cancer or mortality by cancer, we used Cox's hazard proportional analysis. Two-sided P values were reported with 0.05 taken as the level of statistical significance. All data are shown as mean ± standard deviation for continuous variables or frequency per observation for nominal variables.
Ethnic statement
This study was approved by the institutional review board (IRB) in Seoul National University Bundang Hospital (IRB approval number: B-0409/012-003) and other participating hospitals. This study was a retrospective study for which IRB in Seoul National University Bundang Hospital waived patients' consent to review medical records.
RESULTS
Characteristics of patients at renal biopsy
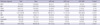
The study sample of 3,288 patients (1,866 males and 1,422 females) had accrued 9,078 person-years (4,109 for males and 4,969 for females) to detect cancer incidence. The mean age at biopsy was 41.4 yr in all patients and was the lowest in the None group (Table 1). The male proportion did not differ among the groups. ARB and/or ACEI were used in 40.4% of the patients. Mean eGFR was 72.0 mL/min/1.73 m2 and was the lowest in the ACEI-ARB group. There were 87 patients with cancer diagnosed before renal biopsy and the proportion of those patients were not different among the groups.
Kidney pathology
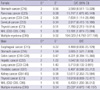
The most frequent diagnosis was IgA nephropathy (44.9%) (Table 2). The frequencies of MCN and Others were higher in the None group, those of MN and MPGN were higher in the ACEI-ARB group, and that of IgA nephropathy was the highest in the ARB-only group. Male was predominant in every diagnosis except Lupus. The mean age at biopsy was the lowest in Lupus (34.5 ± 11.0 yr) and the highest in DMN (54.5 ± 12.9 yr). Hypertension was the most common in DMN (87.8%) and the least in MCN (32.0%).
The incidence of cancer and risk factors to cancer development
After renal biopsy, the cancer was developed in 33 patients (13 females and 20 males) by December 2005 and the incidence rate, adjusted for age and gender, was 1.0% (95% of CI for incidence: 0.7%-1.3%). The cancer was diagnosed in 23 patients within 1 yr, in 6 during 2-3 yr, in 2 during 4-5 yr, and in 2 during more than 5 yr after biopsy. The most frequent cancer was stomach cancer (9 patients), followed by thyroid cancer (6), lung cancer (3), multiple myeloma (3), colon cancer (2), hepatic cancer (2), Non-Hodgkin's lymphoma (2), prostatic cancer (2), cervical cancer (1), esophageal cancer (1), kidney cancer (1), and pancreatic cancer (1). Overall, the incidence of cancer was significantly higher in the patients than in the general population, especially in those aged 65 yr or more (Table 3). Male and female patients showed a 2.481- and 3.270-fold higher rate of cancer incidence, respectively, compared to the general population. The development of cancer was frequent in MN (2.8%, 8/287), DMN (2.7%, 2/74), MPGN (2.4%, 3/127), and Crescentic (2.3%, 1/43). There was 1 case (0.6%) of cancer in 164 Lupus patients, 0.4% (1/235) in FSGS, 0.7% (10/1477) in IgA, none in HSP, and 0.6% (1/172) in MCN. In females, the incidence rate of cancer among patients with IgA (7/642) was 4.906-fold (95% CI: 1.980-10.033) higher and, in males, the incidence rates of cancer among patients with MN (6/177) and MPGN (3/86) were 4.467- (95% CI: 1.647-9.528) and 6.288-fold (95% CI: 1.316-17.773) higher compared to the general population, respectively. Other pathologic diagnoses did not exhibit any differences between the patients and the general population.
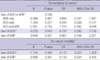
Cancers were found in excess in the pancreas, lung, and thyroid in female patients, and in the stomach and kidney in male patients than in general population. Non-Hodgkin's lymphoma and multiple myeloma were diagnosed more frequently in patients compared to the general population (Table 4). There was no difference of estimated cancer incidence after biopsy among the groups according to the use of ACEI or ARB (Fig. 1A). Cancer was developed in 23 (1.2%) patients of the None, 5 (0.7%) of the ARB-only, 1 (0.4%) of the ACEI-only, and 4 (1.2%) of the ACEI-ARB (P = 0.487) groups. With Cox's hazard proportional analysis, medication with ACEI or ARB was not a related factor to cancer incidence (Table 5).
The incidence of all-cause mortality and cancer mortality
There were 153 deaths (4.7%) caused by malignancy (45), renal disease (38), cardiovascular disease (24), hepatic failure (8), infection (7), SLE (6), and miscellaneous causes (26) until December 2006. Among 87 patients with cancer diagnosed before renal biopsy, 28 patients were dead due to malignancy and the other 17 deaths were in patients with cancer diagnosed after renal biopsy. Most deaths (76.5%) occurred within 24 months after biopsy and the mean duration from biopsy to death was 17.4 ± 23.7 (0.1-183.3) months in the deceased patients (Fig. 1B). The independent risk factors to death were age, eGFR, history of cancer diagnosed before biopsy, renal pathology, and usage of ACEI or ARB with Cox's hazard proportional analysis adjusted with adjustment for age, gender, diabetes, hypertension, history of CVA, CHD, and cancer diagnosed before kidney biopsy, eGFR, usage of steroid and statin, year at biopsy, and renal pathology.
Users of ARB-only, ACEI-only, and ACEI and ARB had mortality risk of 0.263 (0.137-0.504), 0.442 (0.191-1.023), and 0.453 (0.198-1.035)-folds compared to the None-user group by Cox's hazard proportional analysis, respectively. The number of deaths due to cancer was 41 (2.1%) in None and 4 (0.2%) in the other groups (P < 0.001), that is, 3 (0.4%) in ARB-only, 0 (0.0%) in ACEI-only, and 1 (0.3%) in ACEI-ARB (P < 0.001) groups. The independent risk factors to cancer mortality were age, history of cancer, and ARB usage. The risk of cancer mortality in patients with ARB was 0.124-fold (0.034-0.445) compared to non-users of ARB (Table 5).
DISCUSSION
We confirmed that the GN patients showed a higher incidence of cancer, especially in patients with MN, MPGN, and IgA, or patients aged more than 65 yr, compared to the general population. The cancer types more frequently diagnosed in GN patients than in the general population were Non-Hodgkin's lymphoma, multiple myeloma, stomach cancer, kidney cancer, pancreas cancer, lung cancer, and thyroid cancer, which were usually diagnosed within 1 yr after renal biopsy. The use of ARB was an important prognostic factor to decrease cancer mortality without increasing cancer incidence after renal biopsy. The leading cause of mortality in GN patients was malignancy followed by renal disease and cardiovascular diseases.
Cancer occurs in 11% to 13% of patients with the nephritic syndrome (7, 19) and reaches as high as 24.6% in patients over 65 yr presenting with MN (8). The incidence of cancer in GN patients compared to the general population is increased dependent on the age and duration of observation after renal biopsy. Cancer incidence is increased 2.4- to 3.5-fold at < 1 and 1 to 4 yr, respectively, but not for five years or more after renal biopsy (9) and is increased 13.2-fold in older female patients with MN, but not in females aged less than 65 yr (8). Although the well-known type of GN related to malignancy is MN (8), cancer excess is also observed in other pathologic types, such as IgA nephropathy, MPGN, and minimal change lesion (8, 20). Hematologic malignancies such as lymphoma and myeloma are most frequently reported among various types of cancer related to GN (9).
Recently, a meta-analysis of a randomized controlled study showed that patients receiving ARB had a significant increased risk of new cancer compared with patients in a control group (14). However, they pooled the results of studies that were not designed to explore cancer outcomes and did not adjust for any risk factors to cancer development (14). Therefore, further studies are required to confirm these findings.
Few clinical reports have targeted the effect of ARB on cancer incidence. A cohort study, using data of the randomized Department of Veterans Affairs Topical Tretinoin Chemoprevention trial, showed that users of ACEIs or ARBs had a lower incidence of keratinocyte cancers than non-users among 1,051 participants with a high risk of skin cancers (21). Although only 27 participants used ARB compared to 505 using ACEI, users of either of the two had two-thirds the rate of basal cell carcinoma compared to non-users during up to 6-yr follow-up period (21). Among Chinese women in Singapore, genetic polymorphisms in the 5'-regions in angiotensin II type 1 receptor (AT1R) gene (A-168G, C-535T, and T-825A) were studied in the aspect of breast cancer risk (22). Relative to the homozygotes (AA, CC, and TT), individual genotypes with one or two copies of putative low-risk genotypes were each associated with a -30% reduction in breast cancer risk (22). In an in vitro study, angiotensin II stimulated the proliferation of a human breast adenocarcinoma cell line via AT1R and was involved in the pathogenesis of premalignant lesions (23). Those findings suggested AT1R activity might be linked to breast cancer risk.
In the present study, there was no increase of cancer incidence related to the use of ACEI or ARB among GN patients but the use of ARB was related to decrease of all-cause mortality and cancer mortality. In patients with GN, the incidence of all vascular complications, such as acute myocardial infarction or cerebral thrombosis, was higher than in the general population (5). In this aspect, it was surprising that the most common cause of death was cancer in this study. Age was the most important factor in the cancer incidence of MN, which is a well known type of GN associated with malignancy (8). The mean age of patients in this study was higher than that of other studies (5, 6), which might explain the higher incidence of cancer mortality. The blockade of RAAS was not proved to improve overall mortality in patients with diabetes or at high risk for cardiovascular disease (24), although few large studies have examined patients with GN. In this study, ARB usage decreased the mortality, especially in cancer mortality. The relationship between cancer mortality and ARB usage was more evident in patients aged 50 yr or more (users:non-users = 4/357:34/623, P < 0.001) than in younger patients. Previously, candesartan (25) and telmisartan (26) were proposed to have the usefulness of the cytostatic activity in recurrent prostatic cancer. Recipients of either ACEI or ARB showed 3.1-month longer median survival than non-recipients among patients with advanced non-small cell lung cancer (27). We could not identify the relationship between ARB usage and mortality due to lung cancer because only 8 such cases presented in our sample.
Several anti-cancer mechanisms have been suggested for ARB. Inhibition of angiotensin II by ARB or ACEI down-regulates vascular endothelial growth factor (VEGF), which is important in angiogenesis, and inhibites tumor growth (28). Inhibition of AT1R activity decreased leukocyte adhesion, extravasation, and inflammation, which are known risk factors for shorter survival in patients with advanced cancer (29). Stimulation of AT1R activates the mitogen-activated, protein kinase/signal transducers and activators of transcription pathways that play a role in the response to several growth factors regulating cell proliferation (30).
The present study suffered several limitations. The complete information about the histologic findings of light microscopy, immunofluorescence, and electron microscopy were not available in all patients. We gathered the defined pathologic diagnosis from many centers for a long period of diagnosis. The pathologic criteria also varied according to the pathologists and the time. Secondly, the initial laboratory findings were not complete, except the data showed in this presentation, and we could not evaluate the effect of other possible confounding variables that may have affected the incidence and mortality of cancer. Thirdly, the exact dose, brand name, and duration of treatment of ACEI or ARB were not specified. We defined users of medication as being the recipients of ACEI or ARB for more than 3 months, started within 6 months after renal biopsy. We could not evaluate the dose responsiveness for outcomes to medication. Fourthly, the primary cause of death was defined by doctors, but this definition may not have been applied consistently. The data were extracted from the national database and their exactness was not confirmed by the researchers. Fifthly, we could not evaluate the carcinogenic effect of cytotoxic agents, such as cyclophosphamide and azathioprin, which were used in the treatment of glomerulonephritis.
In conclusion, patients with GN show a higher incidence of cancer and cancer mortality compared with the general population. Prescription of ACEI or ARB in patients with GN does not increase cancer incidence and recipients of ARB show rather to be lower rates of all-cause mortality and cancer mortality.



 XML Download
XML Download