

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Knee osteoarthritis (OA) is the most common form of arthritis that affects the elderly. It is a leading cause of disability and has a formidable societal and public health impact (1, 2). The prevalence of symptomatic knee OA is estimated as 12% of the US adults older than 65 yr of age (2). The increasing prevalence of knee OA with age may present serious new health issues in any rapidly aging societies such as Korea. However, the exact prevalence of knee OA in Korea is not known. A few studies have attempted to assess the prevalence of knee OA in Korea, but have used different definitions for knee OA and populations with different demographics (3-6). Reported prevalences of knee OA vary from 10.2% among 867 persons aged 20-69 yr in Guri city to 55% among 432 female rural residents over the age of 40. However, all of these previous reports have limitations, such as, the inclusion of radiographs for only symptomatic subjects, a lack of standardization of knee radiographs, or a failure to utilize a standardized radiographic grading system, such as, the Kellgren-Lawrence system (K-L) (7). In this study, the authors investigated the prevalence of knee OA in elderly residents in Chuncheon and used standardized radiographs and K-L grades to identify the risk factors of knee OA.
MATERIALS AND METHODS
Subjects
The Hallym Aging study (HAS) is a prospective cohort study, which was initiated to investigate qualities of life and health among elderly community residents in Chuncheon city, located about 120 km east of Seoul. This ongoing study commenced in 2004 and involves follow-up examinations at 3 yr intervals. The eligibility criteria applied were; an age of more than 50 yr, residence within the borders of the survey area for at least 6 months before testing, and the mental and physical ability to participate. Two hundred of 1,408 census tracts were randomly sampled to represent residential areas proportionately based on the Korean National Census conducted in 2000 (8). In addition, study subjects were selected so that those over 65 yr old represent about 70% of the study cohort. During the 2004 survey, 918 subjects were interviewed among 1,489 eligible subjects (response rate 61%). The present study involved 702 subjects that participated in the 2007 follow-up survey (64 subjects had died, 49 had moved, and 103 refused to participate or could not be contacted). Five hundred and seventy three subjects who underwent knee radiography were analyzed in this study. The ethics committee at our university approved the study protocol.
Data collection
Demographic information was collected at baseline using a standard questionnaire by face-to-face interview. The questionnaire requested information on educational attainment, marital status, household income, occupation, exercise, and co-morbidities. Occupations were categorized as; none, office work mostly sedentary, work demanding some walking, work demanding physical exertion (sometimes carrying heavy objects or the use of instruments, work demanding heavy physical exertion (e.g., construction worker, laborer, farmer). Work demanding physical or heavy physical exertion was defined as manual work. Exercise status was self-reported and replies were classified as <3 times/week or ≥3 times/week. Co-morbidity health information was also self-reported, and was recorded using 29 pre-defined illnesses categories, which included hypertension, arthritis, stroke, myocardial infarction, diabetes mellitus, and osteoporosis.
Height (cm) and body weight (kg) were measured to the nearest 0.1 cm and 0.1 kg, respectively, with subjects wearing light clothing and barefoot, and body mass indices (BMIs) were calculated.
Knee pain was assessed by asking, "Have you experienced pain, aching, or stiffness lasting at least a month in a knee?". All subjects were also asked to complete the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) questionnaire, a validated instrument that measures knee pain and physical function in those with knee and/or hip OA (9), the Short Form (12 item) (SF-12) questionnaire to evaluate self-reported functional status and physical disability.
Radiographic assessment
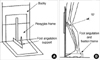
Weight-bearing anteroposterior, 14×17 inch, semi-flexed knee radiographs were obtained of all 573 subjects. A Plexiglas frame (SYNARC, San Francisco, CA, USA) was used to standardize knee positions, according to the manufacturer's recommendations (Fig. 1). This protocol has been utilized in many previous studies (10, 11). Briefly, each knee was filmed separately with the knee of interest centered on film. The great toes of both feet were placed in contact with the anterior wall of the Plexiglas frame, and the index foot was fixed at 5° of external rotation against the V-shaped support at the base of the frame. Patients flexed knees until they touch the anterior wall of the frame. The tube was positioned so that the radiography beam was centered on the joint line of the target knee in the popliteal space at 10° of caudal angulation. To proceed with radiographic evaluations, the following criteria had to be satisfied: 1) Medial tibial plateau was horizontal; 2) The long axis of the tibia was parallel to the vertical margin of the film; and 3) the affected knee was located in the middle of the film (Fig. 2). Knees were evaluated for osteophytes, joint space narrowing, subchondral sclerosis, and cysts, and were graded for overall evidence of radiographic OA using the K-L grade, which allocates grades of 0-4, where 0=none; 1=possible osteophyte; 2=definite osteophytes and/or possible joint space narrowing; 3=moderate osteophytes and/or definite joint space narrowing; and 4=large osteophytes, severe joint space narrowing, and/or bony sclerosis. We considered knees with a K-L grade of ≥2 to have radiographic OA, and knees with a K-L grade of 3 or 4 to have severe radiographic OA (12, 13). Symptomatic knee OA was defined as the presence of knee pain and a radiographic change in the tibiofemoral joint of ≥K-L grade 2. Radiographs were read twice by one reader, an academically based rheumatologist. The reproducibility of intra-reader assessments was high (for OA vs. no OA, κ=0.89). Films allocated different K-L grades at the two readings were adjudicated by consensus between the original reader and a second reader.
Statistical analyses
Subjects were divided into 4 age groups, namely, 50-59 (56 subjects), 60-69 (126 subjects), 70-79 (274 subjects), and 80-89 yr (48 subjects). The age-specific prevalences of radiographic and symptomatic knee OA were calculated. To compare subjects with/without OA, continuous variables were tested using the Mann-Whitney U test and categorical variables using Fisher's exact test. Crude odds ratios (OR) for risk factors of radiographic and symptomatic knee OA were calculated using 95% confidence intervals (CI). Adjusted ORs were calculated by logistic regression analysis after adjusting for age, educational level, the presences of hypertension, osteoporosis, diabetes mellitus, exercise, smoking, alcohol consumption, a manual occupation, and body mass index. Data were analyzed using SPSS version 15. All data are presented as means and standard deviations (SD) or as percentages. P values <0.05 (2-tailed) were considered statistically significant.
RESULTS
Characteristics of the study subjects
Of the 702 that participated in the 2007 survey, 129 refused to undergo radiography. Subjects that declined were significantly older that those that participated. Of the 573 participants, 69 were excluded for poor film quality or a missing film. The remaining 504 constituted our study cohort. Mean subject age was 70.2 yr, and 54% were women. The demographic, clinical, and anthropometric characteristics of the study subjects are summarized in Table 1.
Prevalence of radiographic and symptomatic knee OA by age and sex
Based on our radiographic results, 188 subjects (37.3%) had radiographic knee OA (defined as K-L grade ≥2 in either knee), 111 subjects had bilateral knee OA, 45 had right knee OA only, and 32 had left knee OA only. Of the 188 subjects with radiographic knee OA, 96 subjects (51%) had a moderate to severe OA defined as K-L grade ≥3, and 121 (64%) had symptomatic OA. Women accounted for the majority of subjects with radiographic and symptomatic OA (80% and 86%, respectively). This female preponderance was particularly large in the 60-69 age group. Figs. 3, 4 summarize prevalences of radiographic and symptomatic knee OA by age and sex.
Factors associated with the presence of radiographic knee OA and symptomatic knee OA
Initially, we calculated the age-adjusted odds ratios of radiographic knee OA. It was found that the risk of radiographic knee OA was significantly greater in women and in subjects with a lower level of education, hypertension, osteoporosis, a higher body mass index (BMI), a higher body fat mass, or a lower lean body mass. A manual occupation also found to be significantly associated with an increased risk of radiographic knee OA, whereas smoking and alcohol intake significantly reduced the risk. Subjects with radiographic knee OA also exercised less than subjects with a normal knee radiograph. Multivariate analysis adjusted for age, level of education, presence of hypertension, osteoporosis, diabetes mellitus, exercise, smoking, alcohol consumption, and manual occupation, revealed that body mass index, a lower level of education, the presence of hypertension, and a manual occupation were significantly associated with the presence of radiographic knee OA (Table 2).
We then compared subjects with symptomatic knee OA and subjects with asymptomatic knee OA or without knee OA combined. Risk factors associated with radiographic knee OA were also found to be significantly associated with symptomatic knee OA after age adjustment (Table 3). Multivariate analysis revealed that a female sex, the presence of hypertension and manual occupation were significantly associated with the presence of symptomatic knee OA.
DISCUSSION
In this study of 504 Chuncheon city residents aged 50 yr and older, the prevalences of radiographic knee OA and symptomatic knee OA were 37.3% and 24.2%, respectively. Furthermore, the presence of hypertension and a manual occupation were found to be significantly associated with radiographic and symptomatic knee OA, whereas a lower level of education and a female sex were found to be significantly associated with the presence of radiographic and symptomatic knee OA, respectively. A small number of studies have attempted to assess the prevalence of knee OA in Korea, but reported prevalences vary considerably. Furthermore, these studies were limited by the use of self-reports, the inclusion of only symptomatic subjects for radiographic investigations, or the lack of standardized knee radiograph and a grading system (3-6, 14). Cho et al. reported prevalences of hand and knee OA in the largest community cohort reported in Korea. In this previous study, which involved subjects over 40 yr of age, the prevalences of radiographic and symptomatic knee OA were found to be 14.9% and 5.4%, respectively. These markedly lower prevalences as compared with the present study are probably explained by the age differences between the two cohorts, i.e., mean age 59.2 vs. 70.2 yr, and by the different radiographic technique (sitting vs. weight bearing semi-flexed knee radiograph [present study]). The present study is the first study to evaluate the prevalence of radiographic and symptomatic knee OA using standardized radiographs and a recognized grading system in Korea. Data on the prevalence of knee OA is limited in other than Caucasians and African Americans. It is known that the prevalence of knee OA in East Asia among men is similar to that reported for Caucasian Americans, but that it is higher among Asian women (15, 16). For example, in a study conducted in Beijing among individuals aged ≥60 yr, prevalences of symptomatic knee OA were 15% in women and 5.6% in men (3), and in a community study of Japanese women aged 63 yr or older, the age adjusted prevalence of knee OA was found to be higher than in Caucasians (OR 1.96), whereas the prevalence of hand OA, other than of the distal interphalangeal joint, was lower than that reported in Caucasians (15). As compared with the Beijing cohort, which was similar to ours in terms of age and sex, the prevalence of both radiographic and symptomatic knee OA were higher in the present study, especially among women.
The discrepancy between the total knee replacement (TKR) surgery rates of Korean men and women has been well documented (17). In the previous report, the age-standardized rate ratios of TKR in women as compared with men ranged from 7.4-8.0, which is much higher than those reported in Western countries such as the US and Sweden. Some surgical series have also revealed that female patients account for more than 80% of TKR cases in China and Japan (18, 19). Furthermore, because TKR is performed on the severest cases of knee OA, these findings imply that knee OA is both more prevalent and more severe in Asian women. In the present study, the prevalence of radiographic OA was about 3.5 times higher in women (15.7% vs. 55.5%), while that of symptomatic OA was 5.2 times higher in women (7.4% vs. 38.3%), and this gender difference was particularly marked for those aged between 60 and 70 (Figs. 3, 4). The causes of these gender difference in the prevalences of radiographic and especially symptomatic knee OA in Koreans warrants further investigation.
The risk factors found to be significantly associated with radiographic knee OA in the present study, are largely consistent with those identified in previous studies, thus, corroborating the validity of this cohort for investigation of knee OA. Although high BMI is a major risk factor of radiographic knee OA, the OR for high BMI just reached statistical significance in the present study (adjusted OR 2.04, 95% CI 0.99-4.20) when we defined BMI as ≥25, which we attribute to the rather small sample size of the present study. Nevertheless, we did find that a high BMI was a significant risk factor for men when we analyzed men and women separately (adjusted OR for men, 5.28, 95% CI, 1.25-22.22). Risk factors associated with symptomatic knee OA were similar to those of radiographic knee OA. The associations between hypertension and radiographic and symptomatic knee OA are of note. In the present study, although hypertension was related to a number of confounding factors associated with knee OA, such as, obesity and lack of exercise, it remained significant after adjusting for these factors. In the Chingford population study of 1,003 women aged 45-64 yr, hypertension was found to be associated with both unilateral and bilateral knee OA independently of obesity, which supports the notion that OA has an important systemic and metabolic component in its etiology (20).
Our study has several limitations that require consideration. First, the sample size was rather small, and perhaps, as a result many previously reported risk factors of knee OA did not reach statistical significance by multivariate analysis. Second, only A-P knee radiographs were included, thus, patellofemoral compartment OA, which is currently attracting interest as a major contributor to knee pain, could not be evaluated (21). Finally, the study was limited to the Chuncheon area, which may have lead to bias and prevents us making sweeping generalizations.
In conclusion, the prevalences of radiographic and symptomatic knee OA are 37.3% and 24.2%, respectively, among residents of Chuncheon, which are significantly higher in women than in men. The factors that cause this sex difference in radiographic and symptomatic knee OA in Korea should be identified by future investigations.






 XML Download
XML Download