

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Several studies have reported that hyperuricemia is associated with the development of hypertension and cardiovascular disease (1-3). In addition, epidemiological studies have shown an association between a high level of serum uric acid and increased vascular events and mortality in patients with hypertension (4).
More evidences also show that hyperuricemia may have a pathogenetic role in the progression of renal disease (5). Iseki et al. (6) showed that an elevated serum uric acid level correlated with the development of renal insufficiency in individuals with normal kidney function. Paradoxically, it has been suggested that uric acid have antioxidant activity in experimental studies (7). In addition, it has been reported that uric acid administration to healthy volunteers increase their serum antioxidant capacity (8). Studies have shown that the relationship between serum uric acid and cardiovascular risk is J-shaped with a nadir in the second quintile (3, 9). This may reflect the association between low serum uric acid and low plasma antioxidant activity (10). There are also evidences showing that hyperuricemia seems to induce high blood pressure, renal afferent arteriopathy, a rise in glomerular hydrostatic pressure, and renal scarring (11). However, the relationship between the estimated glomerular filtration rate (eGFR) and serum uric acid has not been studied in people with normal serum levels of uric acid. Therefore, we aimed to investigate the association between eGFR and uric acid in a general population with physiological serum levels of uric acid.
MATERIALS AND METHODS
Study population
We studied adults who were between 20-80 yr old and visited Gangnam Severance Hospital for Preventive Medicine for a medical examination and health counseling. Cross-sectional surveys of adults listed on the electoral roll were undertaken from November 2006 to June 2007. This study is based on an analysis of the data from 2,170 males and 1,658 females at the time of their first survey. A total of 452 subjects (274 men, and 178 women) were excluded based on the following exclusion criteria: 14 subjects reported the current use of blood uric acid-lowering agents; 118 subjects had a history of cancer, ischemic heart disease, stroke, respiratory, renal, liver, or rheumatologic disease; 234 had high levels of uric acid level (≥7 mg/dL for men and ≥6 mg/dL for women) (12), and 86 had missing medical history, laboratory, or urinalysis data. Because some individuals were excluded for multiple reasons, the total number of eligible subjects for the study was 3,376 (1,896 men, and 1,480 women).
Data collection
Medical examinations were performed by trained medical staff according to a standardized procedure. Participants were asked about health-related behaviors, including cigarette smoking, alcohol consumption, and physical activity as well as current treatments for any type of disease. If subjects were receiving treatment, they were asked to provide the date of diagnosis of the disease and a list of medications being taken. Body weight and height were measured in light indoor clothing without shoes to the nearest 0.1 kg and 0.1 cm, respectively. Body mass index (BMI) was calculated as the ratio of weight (kg)/height (m2). After a 12-hr overnight fast, blood samples were obtained from each subject from the antecubital vein. Fasting plasma glucose, total cholesterol, triglyceride, HDL-cholesterol, high sensitivity-C reactive protein (CRP), and uric acid were measured using a Hitachi 7600-110 Chemistry analyzer (Hitachi, Tokyo, Japan). Kidney function was calculated using the Modification of Diet in Renal Disease 7 (MDRD7) equation: GFR (mL/min per 1.73 m2)=170×(serum creatinine)-0.9994×(age)-0.176×(BUN)-0.170×(albumin)0.318×(0.762 if female) (13).
Urine protein was determined at each examination by a single uric stick semi-quantitative analysis (URiSCAN Urine Strip; YD Diagnostics, Yong-In, Korea). Dipstick urinalysis was conducted on fresh, midstream urine samples collected in the morning. The amount of urine protein was reported as absent, trace, 1+, 2+ 3+, or 4+. The results of trace, 1+, 2+, 3+, and 4+ correspond to protein levels of about 10, 30, 100, 300, and 1,000 mg/dL, respectively. Proteinuria was defined as grades of 1+ or above (14). Diabetes was defined as a self-reported history of the disease or a fasting plasma glucose level ≥126 mg/dL. Hypertension was defined as a self-reported history of the disorder, systolic blood pressure ≥140 mmHg, or diastolic blood pressure ≥90 mmHg.
Statistical analysis
Clinical and chemical characteristics of the study population were summarized. All continuous variables are presented as means (SD) or medians (IQR), and the categorical variables are summarized as percentages in each group. Due to skewness, CRP was log transformed before statistical analyses. Pearson and Spearman rank correlation coefficients were determined for GFR vs age, BMI, cigarette smoking, regular exercise, systolic and diastolic blood pressure, plasma glucose, CRP, non HDL-cholesterol, proteinuria, hypertestion, diabetes, and uric acid in men and women. To examine independent factors of GFR, multivariate linear regression analyses were performed. All analyses were conducted using SPSS statistical software (version 15.0). All statistical tests were 2-sided, and significance was determined at a P value <0.05.
RESULTS
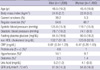
The data of 3,376 study participants are presented in Table 1. The average age was 46.5 yr for men, 45.4 yr for women, and the mean level of serum uric acid was 5.2 mg/dL for men and 4.1 mg/dL for women. Approximately 39.2% of men and 5.3% of women were current smokers, while 64.6% of men and 48.7% of women exercised regularly. The overall prevalence of diabetes was 2.5% for men and 1.4% for women.
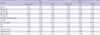
In multivariate linear regression analysis, age, DM, cigarette smoking, fasting plasma glucose, non-HDL cholesterol, and uric acid were found to be independent variables that were significantly associated with GFR in men. Non HDL-cholesterol and uric acid were found to be independent variables associated with GFR in women (Table 2). Multiple stepwise regression models were used to evaluate the association of GFR with uric acid (Tables, 3, 4). The association of GFR with uric acid was negative after adjusting for age, DM, cigarette smoking, fasting plasma glucose and now HDL-cholesterol (Table 4).
It has been observed an increase in uric acid of 1 mg/dL is independently association with a decrease in GFR of about 5 mL/min/1.73 m2 in men and about 6 mL/min/1.73 m2 in women in Table 4.
DISCUSSION
In the present study, we found an association between increased uric acid levels and decreased GFR in Koreans with normal serum levels of uric acid. The liver produces uric acid by degrading dietary and endogenously-synthesized purine compounds. Uric acid is reabsorbed and excreted by the proximal tubular cells. Therefore, hyperuricemia might develop when the production of uric acid increases or the excretion of uric acid declines, or both (15). Several studies have shown that an increase in uric acid is associated with hypertension, cerebral vascular disease and chronic kidney disease (CKD) (2, 16, 17). Experimental animal studies and in vitro studies have identified the mechanisms in which elevated uric acid levels might cause nephrotoxicity. Afferent arteriopathy, mild tubulointerstitial fibrosis, glomerular hypertrophy, and glomerulosclerosis occur in hyperuricemic rats (18). However, despite several epidemiological, experimental, and prospective cohort studies, it is still controversial whether hyperuricemia can be considered to be a risk factor for the progression of CKD. Sturm et al. (19) reported that uric acid levels are not independent predictors of the progression of CKD. However, Iseki et al. (20) reported that a high level of serum uric acid was more predictive for the development of renal dysfunction than proteinuria. One of the reasons for the controversy over whether hyperuricemia is a risk factor for the progression of CKD is that uric acid may function as an antioxidant (21). Uric acid can chelate transition metals and can scavenge singlet oxygen and superoxide radicals (22). GFR has been suggested to be an indicator of early stages of kidney dysfunction (23). Therefore, we investigated the association between GFR and uric acid in a population with normal serum levels of uric acid. In multivariate linear regression analysis, age, cigarette smoking, fasting blood sugar, DM, and uric acid were independently and negatively associated with GFR in men, but not in women. Non-HDL cholesterol and uric acid were independently and negatively associated with GFR in both men and women. Messerli et al. (24) reported that a decrease in GFR was correlated with an increase in uric acid in patients with hypertension. They argued this is because a low renal blood flow stimulates uric acid reabsorption. However, in our study, GFR was not significantly correlated with hypertension in either men or women. Galvan et al. reported that hyperuricemia develops frequently in subjects with insulin resistance, because insulin stimulates sodium and uric acid reabsorption in the proximal tubule (25). GFR was negatively associated with fasting blood sugar and DM in men, but not in women. The reason for this difference is unclear; however, the uricosuric effect of estrogen could be one possible reason for this difference (25). Recently, Chonchol et al. (26) reported that high uric acid levels are strongly associated with the risk of kidney disease progression and a decrease in estimated GFR based on a prospective community-based cardiovascular health study of 4,610 participants. However, it is also possible that hyperuricemia is just a bystander to kidney disease. One reason for this hypothesis is the fact that uric acid is excreted by the proximal tubular cells. When GFR decreases, both enteric excretion and fractional urinary excretion increase, but these processes do not fully compensate for the decrease in GFR, and hyperuricemia is induced (15). Therefore, CKD could be the cause of hyperuricemia. The other reason that hyperuricemia could just be a bystander to kidney disease is that uric acid is an antioxidant in the extracellular setting (22). Our study showed that an increase in uric acid of 1 mg/dL is independently associated with a GFR decrease of about 5 mL/min/1.73 m2 in men and about 6 mL/min/1.73 m2 in women. Although it is possible that a high level of uric acid could simply be a result of low GFR, several studies have provided evidences that uric acid might actually play a role in the development or progression of renal disease. Kang et al. (5) showed that uric acid induced renal hypertrophy, glomerulosclerosis and interstitial fibrosis in animal study. Yen et al. (27) reported that serum uric acid level was associated with a decline in renal function in a prospective study. Siu et al. (11) reported that allopurinol therapy was able to significantly decrease the probability of kidney function deterioration in a prospective trial of 54 hyperuricemic patients with CKD. Kanbay et al. (28) showed that treatment with allopurinol improved not only uric acid levels but also GFR in patients with normal renal function. These results suggest that uric acid might have play a pathologic role in kidney disease progression. Our findings are consistent with previous results showing a negative association between eGFR and the serum level of uric acid.
This study has several limitations. First, we used eGFR to assess renal function instead of directly measuring GFR. However, several organizations recommend the use of equations that estimate GFR to evaluate renal function in epidemiologic studies (29). Second, a dipstick can be inaccurate for detecting proteinuria, because the number of false-positives can be increased by a comorbid illness in older people or by menstruation in women. However, in our study, we used this variable only as an adjustment variable. A third limitation was that the influence of hypertensive drugs as confounding variables was not examined. Diuretics such as thiazides increase serum uric acid by stimulating uric acid reabsorption in the proximal tubule (30). Last, this was a cross-sectional study; therefore, it is not clear whether the observed serum levels of uric acid contribute to the development of CKD. The potential therapeutic effects of lowering uric acid levels in CKD patients should be investigated in future prospective studies.
In conclusion, uric acid is independently and negatively associated with GFR in both men and women with normal serum levels of uric acid. This suggests that a high level of uric acid is a valuable predictor of a GFR decrease, and our findings have important clinical and public health implications.


 XML Download
XML Download