

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Osteoporotic vertebral body fracture is reported progressively more with increased aging. The prevalence of osteoporotic vertebral compression fracture (OVCF) is estimated to be 26% in women over 50 yr old and 40% in over 80-yr-old women (1). About one third of OVCFs cause severe back pain with variable pain patterns (2, 3). Procedures like percutaneous vertebroplasty (PVP) or kyphoplasty (PKP), in which polymethylmethacrylate (PMMA) is injected into the collapsed body, have been progressively used to stabilize OVCFs as they can be performed with relative safety under local anesthesia (4, 5).
Despite the exponential increase of publications on the treatment of vertebral body fractures (VBFs) using vertebroplasty or kyphoplasty, pain evaluation has not been commonly reported (6). Most reports adopted simple numerical rating scores (NRS) to measure pre- and post-operative pain severity. Remarkably, despite the common prevalence of osteoporotic compression fractures, qualitative pain analysis, including pain distribution patterns in relation to the disease severity, was not investigated to fully understand the clinical characteristics of the disease. However, pain evaluation is admittedly proven to provide the basis of hypothesizing the mechanism of pain production as well as the initial guide to decision making in the management of the spinal pain (7-10). We analyzed the pain distribution patterns in relation to the morphological changes of the vertebral bodies to elucidate the pain mechanism in patients with OVCF and to determine better strategies for pain management.
MATERIALS AND METHODS
Patient population
Between May 2005 and May 2007, a total of 64 primary OVCF patients were prospectively investigated and followed up. All patients underwent PVP or PKP to control their pains. Thorough clinical and neurological examinations and simple radiography were performed routinely. Bone scintigraphy was performed to confirm the symptomatic compression fracture in all. Magnetic resonance imaging (MRI) and computed tomography (CT) examinations were also performed in most cases to differentiate the acute from chronic fractures, to rule out the unstable fractures, and to distinguish the benign compression fractures from underlying tumors or infections. All patients were interviewed by a pain-specialist nurse, who recorded the pain distribution pattern, NRS, nature of pain, pain-related dynamic factors, and factors influencing life pattern and daily activities. Exclusion criteria comprised the pathological fractures due to underlying tumors or infections: presence of neurological deficits, uncooperative patients, uncorrectable coagulopathy, severe rigid collapse of the vertebral body, and significant retropulsion of the bone into the spinal canal. In addition, patients who had collagen, vascular, or rheumatologic diseases were also excluded.
Evaluation of pain pattern
Pain drawing was completed by all patients before the operation. Drawings of pain patterns were analyzed to harvest the most frequently presented patterns. Subsequently, the pain patterns were classified into three types of pain patterns (Fig. 1): Type A shows the pain distribution in the aravertebral area mostly localized to midline. Type B shows the diffuse extension of paravertebral pain. Extension of paravertebral pain was confined to posterior back in Type B1. However, if the pain extended into the anterior chest, it was coined as Type B2. Type C indicates the low back pain or lumbosacral pain remote from the site of the lesion.
Measurement of compression fracture
Vertebral compression fractures were divided into three types depending on the preoperative radiography findings: compression fracture involving anterior column only (Type I fracture), fracture involving anterior and middle column without encroching into the spinal canal (Type II fracture), and facture combining Type I and Type II fracture (Type III fracture).
The height of the vertebral body represented as deformity index, kyphosis rates and kyphosis angles were measured in lateral radiographs and MRI sagittal views before and after the operation according to Nakano et al. (Fig. 2) (11). Briefly, vertebral deformity index indicates the ratio of the sum of three heights to longitudinal diameter of the vertebral body. Kyphosis rate is the percentage of anterior height/posterior height of the vertebral body. Kyphosis angle represents the angle between the lines drawn in the lower margin of the upper vertebra and upper margin of lower vertebra.
Operative techniques
Vertebroplasty or kyphoplasty was performed in the same manner as in previously reported PMMA percutaneous techniques (12-14). One 11-gauge needle was introduced via transpedicular route to reach over the center under fluoroscopic guidance in most cases. However, two-needle technique was also employed according to the surgeon's preference. After intravertebral injection of the contrast dye, an average of 3 to 5 cc of PMMA was injected into the fracture's vertebral body with care to prevent leakage. After injecting the PMMA, the patients remained on the operating table until the cement hardened. For the kyphoplasty, a balloon was introduced and inflated to achieve compaction of surrounding cancellous bone and varying degree of elevation of the compressed vertebra, followed by injection of PMMA.
Postoperative outcomes
NRS for pain were checked before and after each procedure as part of a baseline questionnaire administered to all patients. Pain drawing was also done to investigate the changes of pain distribution by operations. For analysis of treatment outcome, patients who showed more than 50% pain reduction following PVP or PKP were considered as a favorable outcome group. All patients were followed up at 1, 3, and 6 months following the procedure.
Statistical analysis
Statistical analysis was performed using SPSS software (SPSSWIN 12.0: SPSS, Inc, Chicago, IL, U.S.A.). Differences in the deformity index, kyphosis rate, and kyphosis angle following the operation were compared using paired t-test. Pain patterns were compared with change of deformity index, kyphosis rate, and angle using Pearson correlation. Postoperative outcome was also compared with differences in the deformity index, kyphosis rate and angle using the Pearson correlation. Relation of pain patterns with outcome was compared by analysis of variance (ANOVA). A p value less than 0.05 was considered statistically significant.
RESULTS
Demographic profile
Table 1 summarizes the demographical characteristic of the patients. Patients consisted of 14 males (78%) and 50 females. Average ages of male and female patients were 74.57±9.7 and 69.16±9.5, respectively. Augmentation of the vertebral body was performed by PVP in 55 patients (73 vertebral bodies) and by PKP in 9 patients (10 vertebral bodies). Among 83 vertebral bodies, the most commonly treated one was L1 (N=29), followed by L2 (N=16), T12 (N=13), T11 (N=8), and T9 (N=5). The average interval from injury to operation was 18.95±21.54 days.
Pain patterns and morphological changes
Preoperative radiography showed Type I fracture in 21 patients, Type II fracture in 40, and Type III fracture in 3 patients. Types of fratures were not significantly correlated with pain patterns in the patients with OVCF. Pain patterns of the patients with OVCFs are shown in Fig. 1. Type A pattern was demonstrated in 9 patients, Type B in 27 (Type B1: 17 and Type B2: 10), and Type C in 28 patients (Fig. 2). Type A pattern was commonly represented in the patients with involvement of L2 (40%), T12 (20%), and L1 (20%): Type B was common in L1 (56%), L2 (32%), and T9 (26%): Type C in L1 (47%), T12 (22%), L2 (16%).
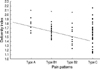
As deformity index is decreased, extent of pain distribution was enlarged. Type A and B patterns significantly showed the reverse relationship with deformity index (p<0.05). On the contrary, Type C pattern was not affected by deformity index. As deformity index decreased, extension of pain was evident (Fig. 3). On the other hand, the kyphosis rate and angle were not significantly changed with the pain patterns.
Pain severity and postoperative outcome
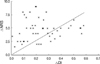
Preoperative NRS was 7.7 in Type A, 7.8 in Type B1, 8 in Type B2, and 7.3 in Type C. PVP or PKP significantly reduced pain in all the patients with OVCFs in the same manner as in previously published studies. Type A showed the most improvement of pain following the procedures, followed by Type B1 and B2 (Fig. 4). However, Type C did not significantly affect the postoperative outcomes. Deformity index, kyphosis rate, and angle show a significant change following PVP or PKP (p<0.05), respectively (Fig. 5). As the height of vertebral body (deformity index) was increased following the procedure, postoperative outcome improved (Fig. 6). Consequently, postoperative difference of deformity index was reversely related with favorable outcome. Postoperative differences in the kyphosis rate and angle were, however, not correlated with postoperative outcome.
Adjuvant treatments and complications
PVP- or PKP-related complication was not observed in our study group except for minor leakages. Minor leakage was observed in 5 patients; however, they did not cause any neurological deficit at all. Six patients with Type B pattern underwent medial branch blocks or radiofrequency (RF) neurotomies at the site of fractures because of unsatisfactory long-term control of pain. Four of them showed positive results. Five patients with Type C pattern also received medial branch block, three of which showed alleviation of their pains.
DISCUSSION
Thoracic spinal pain has been very rarely described; therefore, there has been a limitation in interpreting the clinical features that allow a physician to diagnose with confidence. Historically, classical experiments by Kelgren and Feinstein showed the common patterns of pain referral following irritation of thoracic spinal somatic structures (15, 16). Recently, these were further refined in normal volunteers to map the pain referral patterns elicited by noxious stimulation of the thoracic zygapophyseal joints (8). Moreover, although pain patterns depend on the location of the disk pathology and whether neural elements have been compromised, thoracic disc herniation presents dull backache localized to thoracic spine as a primary symptoms (17, 18). Previous studies did not satisfactorily show pain referral patterns in the osteoporotic compression fractures despite the high incidence of OVCFs. Nonetheless, if the regional variation is accepted, the expression of symptoms may be analogous to that of cervical and lumbar spine based on the anatomical background, since all spinal structures are commonly innervated by similar nerves: zygapophyseal joints and paravertebral muscles by medial branches, the anterior third of vertebral body and disk by sympathetic nerves, and the posterior two thirds by sinuvertebral nerves (19, 20).
Our results showed that our classification of pain patterns can encompass most referral pain due to OVCFs: midline paravertebral (Type A), diffuse paravertebral (Type B), and remote lumbosacral pain (Type C). Pain mechanisms may be multifactorial, for compression fractures not only damage the vertebral bodies but also secondarily affect the neighboring structures that may play a role as pain generators. Recent studies on pain pattern in other degenerative disorders demonstrated that various pain distribution patterns can be differentiated from each other depending on the source of pain (7). Interestingly, we drew an analogy between the paravertebral pain due to OVCFs, and discogenic pain and zygapophyseal joint pain which are common in patients with degenerative spinal disorders. This analogy potentially suggests that midline paravertebral pain (Type A) may come from the irritation of the sinuvertebral nerve endings which are innervating the outer third of the vertebral body. Meanwhile, diffuse paravertebral pains (Type B) may be caused by the zygapophyseal joint pathology secondarily resulting from decreased height of the vertebral body. Diffuse paravertebral pain may often combine midline paravertebral pain, thus, zygapophyseal joint seems to play an important role in potentiating the pain expression, Remarkably, our study showed that diffuse paravertebral pain (Type B) is significantly related to deformity index (height of vertebral bodies). Also pain was extended in the anterior chest to the lowest height of the vertebral body as the height of vertebral bodies decreased.
Low back or lumbosacral pain from OVCFs is a unique phenomenon because the pain is distributed far from the site of injury. It seems to be not directly linked to the upper back problem; however, Head's drawing of dermatome clearly showed that T12, L1 and L2 dermatome are localized in the low back and lumbosacral area (21). Therefore, if the posterior branches of the spinal nerve at T12, L1, and L2 are irritated by the narrowing of the intervertebral foramen resulting from the decreased height of the vertebral bodies, their pain may have been distributed in these areas as a radicular or somatic referred pain. Interestingly, their dermatomal pain is very similar to the pain distribution patterns of lumbar zygapophyseal or sacroiliac joint arthropathy, and thus requires careful attention to differentiate it from that of lumbosacral joint arthropathies.
It is generally understood that vertebroplasty or kyphoplasty can reduce the pain for two reasons: increasing the strength of hardening of the fractured vertebral body is expected to reduce pain by halting further compression or micromotion (22, 23) and PMMA cement itself is toxic to the nerve of bone (24). Furthermore, heat generated during the course of cement hardening causes at least partial denervation of the bone matrix (24, 25). We believe that these hypotheses are the leading parameters for pain reduction. Although there are some reports suggesting that vertebroplasty does not restore the vertebral body height, our study revealed that the height of the vertebral body is significantly increased after vertebroplasty or kyphoplasty similar to other reports (14, 26-28). In addition, our study showed that the increase of height was directly related with positive postoperative outcomes. Recent reports also support this as the immediate outcomes of PVP were found less effective in patients with more collapsed vertebrae (29). Therefore, the decrease of vertebral body height damages the surrounding zygapophyseal joint and narrows the intervertebral foramen leading to the symptoms of paravertebral and lumbosacral pain. Conversely, it is hypothesized that restoration of the height is contributing to reduce the pain arising from the secondary changes by compression fractures.
Recently, combined approaches for the management of OVCFs were reported with promising results. These procedures add facet joint block or medial branch block, neurotomy of gray ramus communicans, and sympathetic ganglionectomy as a preoperative screening or adjuvant therapy to the main vertebroplasty procedures (30, 31). Considering the secondary morphological changes in the surrounding spinal structures by compression, it seems to be ideal to perform other denervation procedures if such changes are observed. We performed medial branch blocks or RF neurotomies in the patients with type B and C with promising results. Patients with paravertebral pain may be recommended for medial branch neurotomy, based on the pain pattern study. On the other hand, transforaminal selective epidural block may be suggested for lumbosacral pain because their pain may arise from the irritation of the posterior spinal root or dorsal root ganglion.
Our study has limitations in interpreting all pains resulting from OVCFs, because all pain mechanisms are not fully understood. Furthermore, location of pain may overlap with that of other spinal disorders, for instance, annular tear of thorasic disc may present diverse radicular referral pattern of pain including radicular or referral depending upon the anatomical location of annular tear. Anterior tears may refer pain to anterior chest, while posterior tears typically produce back pain in either a local or diffuse pattern (32). However, we believe that our classification of pain pattern may be useful as an initial guide to hypothesize the pain sources from OVCFs, and hence facilitate decision-making in the pain management of these patients. Further work is needed to enhance accuracy in finding the pain source and in differentiating the pain patterns which may come from other spinal structures.





 XML Download
XML Download