

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hip fracture occurs primarily in the elderly, and is one of the most important causes of disability and death in this age group (1). The number and mean age of the elderly continues to increase, and thus fracture incidence is likely to follow (2-5). Hip fracture is becoming a major health burden worldwide. Rowe et al. (6) at our institute, reported the first epidemiological study on hip fracture in Korea and provided much information. However, since the previous study conducted in 1991 (reported in 1993) the socio-economic environment has changed and the number of elderly Koreans has increased.
The purpose of this study was to determine the incidence of hip fracture in 2001, to compare this with that of 1991.
MATERIALS AND METHODS
Patients aged 50 yr or more, living in Gwangju City and Chonnam Province, Korea, and who sustained a fracture of the hip during the year 2001 were investigated. Primary patient information was obtained from the Health Insurance Review Agency (HIRA). As a crosscheck, all hospitals to which patients suspected of hip fracture might have been referred were visited. A total of 125 hospitals was visited, and medical records and radiographs were reviewed. All registered patients with a diagnosis of hip fracture or with a suspected diagnosis of hip fracture were reviewed. In this study, only patients who were admitted to hospitals for primary treatment of a first hip fracture were selected. We also interviewed patients or relatives by telephone to confirm post-fracture course or survival. The time from injury to interview ranged from 15 to 25 months with a mean of 18 months.
There were 1,152 patients; 367 from Gwangju City and 785 from Chonnam Province. Only fractures of the femoral neck and intertrochanteric fractures were included, subtrochanteric fractures were excluded, since they usually caused by high energy trauma.
Information collected from the hospital records included age, sex, the nature of injury, the day of injury, location, the period from injury to hospital presentation, the method of treatment, the degree of osteoporosis, and the presence of concomitant medical conditions. Location and type of fracture were determined from radiographs. The degree of osteoporosis was measured using the method of Singh et al. (7).
The level of daily activity was graded into 4 groups according to a modification of Halpin and Nelson classification (8). The semiactive group in his classification was subdivided into those with "moderate activity" and those with "limited activity". In the present study, we described patients with full and moderate activity as having "good activity", and those with limited activity or who were bedridden as having "poor activity".
Population figures were obtained from the Korea National Statistical Office. Age and sex specific annual incidences were calculated using the population of the Gwangju City and Chonnam Province area as of 1 July 2001.
RESULTS
The population of the Gwangju City and Chonnam Province, aged 50 yr or more in 2001, was 864,966, of whom 491,673 were female and 373,293 were male, giving a sex ratio of 1.3:1. These individuals accounted for 25% of the total population (3,483,073) of this area.
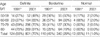
Hip fractures occurred in 1,152 patients, an incidence of 0.133% (13.3/10,000 per year) in this age group; 15.0/10,000 in Gwangju and 12.6/10,000 in Chonnam. Incidences were 3.1/10,000 in the age group 50-59 yr, 9.3 between 60-69 yr, 26.6 between 70-79 yr, and 62.8 in patients aged 80 yr or more. Age specific incidence rates showed a gradual increase (p<0.001) (Table 1).
No significant differences were found between the incidences in urban and rural areas. In the urban area (Gwangju, Mokpo, Yeosu, and Suncheon Cities), this was 14.2/10,000 and in the rural area 12.5/10,000 (p=0.239).
The mean age of patients who sustained a fracture was 74.1 yr (range 50 to 100 yr), and was 70.6 yr in men and 76.2 yr in women. The mean age for a fracture of the femoral neck was 74.1 yr and for an intertrochanteric fracture 74.2 yr. The mean age of patients from urban areas was 73.9 yr and from rural areas 74.4 yr. There was a 5.6-yr difference between the mean age of men and women (p<0.001), but no statistical difference was found between the two fracture types or between their incidences in urban and rural areas.
In terms of sex distribution among those that experienced a fracture, 730 were females and 422 males, a ratio of 1.7:1 (p<0.001). The frequency of hip fractures among men was 11.3 per 10,000 per year (422/373,293), and among women was 14.8 per 10,000 (730/491,673), thus female patients predominated (p<0.001).
Fractures occurred in spring in 301 patients, summer in 276, fall in 292, and winter in 283, which was not significantly different (p=0.746). 907 patients (78%) were injured by slipping at ground level, 101 by falls from more than one meter, 79 in road traffic accidents, and 65 from other causes.
The average period elapsed between injury and presentation at hospital was 2.7 days, ranging from the day of injury to 180 days after injury. Only 64% (732/1,152) visited hospital on the day of injury.
There were 557 fractures of the femur neck. The subtypes were subcapital in 278 (50%), transcervical in 160 (29%) and basicervical in 119 (21%). And there were 595 intertrochanteric fractures; Type I of the Tronzo classification (9) was found in 43 (7%), Type II in 153 (26%), Type III in 269 (45%), Type IV in 116 (19%), and Type V in 14 (2%). The ratio of neck fracture to intertrochanteric fracture was 1:1.07.
Radiographic examinations showed definite osteoporosis (Singh Grade I-III) in 70%, borderline osteoporosis (Grade IV or V) in 29%, and 1% were normal (Grade VI). Definite osteoporosis was seen in 48% of patients aged 50-59 yr, in 65% of those aged 60-69 yr, in 70% of those between 70-79 yr and in 81% in those aged 80 yr or more (Table 2). Women and those with a fracture of the femoral neck showed more osteoporosis. Definite osteoporosis was identified in 63% of males and in 73% of females (p=0.000). Osteoporosis was observed in 73% of fractures of the femoral neck and in 67% of intertrochanteric fractures (p<0.012).
An operation was performed in 1,010 patients (88%). Operations included replacement arthroplasty of the femoral head in 434, total hip replacement in 39, and osteosynthesis in 537. The types of fixation used in osteosynthesis were a compression hip screw in 341, multiple pins in 83, an Ender intramedullary nail in 5, a Rowe plate in 2, a Gamma nail in 101, and an angled blade plate in 5. Arthroplasty was performed in 393 of 490 operations for a fracture of the femoral neck, and in 80 of 520 procedures for intertrochanteric fracture (Table 3).
Of 1,010 patients (88% of all patients) who received an operation, 374 (37%) achieved full activity postoperatively, 245 (24%) moderate activity, 180 (18%) limited activity, and 211 (21%) were bedridden. In 142 patients that received non-operative management 33 (23%) showed full activity, 9 (6%) moderate activity, 17 (12%) limited activity, and 83 (59%) were bedridden. Postinjury activity was good in 61% of the operated group and in only 30% of the non-operated group (p<0.001).
Of the 1,152 patients, 172 died within 12 months of injury, a mortality rate of 14.9%. The age and sex adjusted mortality rate in the general population was 5.8% in this age group. In detail, the mortality rate in the operated group was 5.5% within 3 months of injury, 7.7% within 6, 10.5% within 9, and 12.3% within 12. The mortality rate in the non-operated group was 16.2% within 3 months of injury, 23.2% within 6, 32.4% within 9, and 33.8% within 12 (p<0.001). Thus the annual mortality rate of patients that experienced fracture (14.9%) was 2.6 times higher than in the general population (5.8%).
Significant changes after 1991
To determine significant changes during the 10-yr period from the year of 1991, when the first Korean epidemiological study of hip fracture was conducted by our institution in the same area (6), the year 2001 and 1991 results were compared.
The total annual number of hip fractures rose considerably during the 10-yr period from 247 in the year 1991 to 1,152 in 2001, an average increase of 36.6% per year. The fracture incidence also increased remarkably from 3.3 per 10,000 in 1991 to 13.3 in 2001, representing a 4-fold increase over 10 yr (p<0.001).
In 1991, the total population of Gwangju City and Chonnam Province area was 3,685,283 and the population aged 50 yr or more was 757,417, accounting for 20.6% of the total population. In the year 2001, there was a 5.5% decrease in the total population versus 1991, but the population aged 50 yr or more increased by 14.2% (p<0.001).
The mean age of the elderly that experienced a hip fracture also rose during this 10-yr period from 70 yr in 1991 to 74 yr in 2001. In women this increase was from 73 yr to 76 yr, and in men from 67 yr to 71 yr.
Although seasonal incidences were not significantly different, there was a difference between the observed seasonal increases. Increases in incidence of fractures were higher in winter (4.7-fold increase) and spring (4.4-fold increase) than in fall (3.8-fold) and summer (3.6-fold), suggesting that the elderly people are becoming at higher risk of falling in the cooler seasons.
Regarding fracture pattern, a definite increase was observed in unstable intertrochanteric fracture (Tronzo type III, IV, V), which is usually caused by a severe fall. In 1991, the proportion of unstable intertrochanteric fractures was 54%, which increased to 66% in 2001 (p=0.006).
A significant increase in definite osteoporosis was noted, from 50% in the year 1991 to 70% in the year 2001 (p<0.001). A remarkable increase was observed in two age groups: 27% in the year 1991 to 48% in the year 2001 in those aged 50-59 yr (p=0.012) and 37% in the year 1991 to 65% in the year 2001 in those aged group of 60-69 yr (p<0.001) (Table 2).
DISCUSSION
Our results confirm a rising trend in the absolute number of hip fractures from 247 in 1991 to 1,152 in 2001, which is equivalent to a fracture incidence from 3.3 persons per 10,000 population in the year 1991 to 13.3 in 2001, and an age-adjusted incidence from 3.74 persons per 10,000 population in the year 1991 to 13.3 in the year 2001. This study also confirms rising trends in age-specific incidences of women and men, as illustrated in Table 1. An increase of 4.8-fold was observed in women and 3.1-fold increase in men in terms of fracture incidence during the 10-yr period from the year 1991 to 2001.
There were two limitations of our study. In the first limitation, there were patients who were not treated in the hospitals after hip fractures. As their number is very small compared with the number of hospital admission in the present medical system, the resulting underestimation of the incidence of these fractures is negligible. In the second limitation, patients developed the hip fracture in our study area were transferred to the other region in any cause. Informations obtained from the HIRA were included all the patients who had hip fractures in our country. Because we selected all the patients registered in the Gwangju City and Chonnam Province among the above mentioned patients, the loss of patients who were transferred to outside the Gwangju City and Chonnam Province could be prevented.
In most industrialized countries, the overall number of hip fractures is increasing annually. Kannus et al. (1) reported a 2.7-fold increase in fracture incidence over 27 yr in Finland. Martin et al. (10) reported an increase of 59.7% in women and 42.2% in men in annual hip fracture numbers during the period 1972-1984. In Singapore, fracture incidences in 1957-1963, were 106/10,000 in women and 148/10,000 in men for ethnic Chinese and 44 in women and 52 in men for ethnic Malays (11). According to studies made in 1991-1998 (12), these incidences increased to 410 in women and 168 in men for Chinese and 264 in women and 71 in men for Malay. These data mean that the increase in fracture incidence was from 3.7- to 6.0-fold in women and from 1.1- to 1.4-fold in men.
In the present study, an increase in fracture incidence of 4.8-fold was observed in women and 3.1-fold in men during the 10-yr period from the year 1991 to 2001. Thus, our study demonstrates that the number of hip fractures in Gwangju City and Chonnam Province, Korea has increased at a rate that cannot be explained by demographic changes alone. The precise reason for this are not known, but increases of osteoporosis and injurious falls of the elderly could partly account for the difference. The incidence of osteoporosis and an increased propensity for injurious falls have been proposed as factors frequently in the literature (1, 13-16). These factors include increased body height, greater occurrence of associated systemic diseases, poorer nutrition including calcium and vitamin D, more frequent use of drugs (particularly psychotropic drugs), greater consumption of tobacco and alcohol, a less active life style, poorer general mobility including an impaired gait, balance, proprioception, reaction times, and muscle strength (1, 13, 15, 17).
As a possible explanation for the rising incidence observed in the present study, three factors are suggested by our results. Firstly, there was an increase in the elderly population from 20.6% of the total population in the year 1991 to 24.8% in the year 2001. Secondly, bone weakness increased due to osteoporosis. Patients with definite osteoporosis increased substantially from 50% in the year 1991 to 70% in the year 2001. A remarkable increase was observed in two age groups, i.e., 27% in the year 1991 to 48% in the year 2001 for those aged 50-59 yr, and 37% in the year 1991 to 65% in the year 2001 for those aged 60-69 yr. Thirdly, the risk of injury increased due to a higher activity level. Although seasonal incidences were not significantly different, seasonal increase differences were found. As compared with the year 1991 figures in the year 2001 fractures increased more so in winter (5.5-fold) and in spring (5.3-fold) than in the summer (4.0-fold) and fall (4.2-fold), suggesting that the elderly people are becoming at higher risk of falling in the cooler seasons. In addition, the proportion of unstable intertrochanteric fracture increased from 54% in 1991 to 66% in the year 2001.
In conclusion, the reasons for this rising trend of hip fracture in Gwangju City and Chonnam Province, Korea, were not fully explained. However, an increase in the elderly population, an increase in osteoporosis, and an increase in injurious falls could partly account for the observed increase.


 XML Download
XML Download