

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Apolipoprotein E (apoE) is a plasma protein that serves as a ligand for low density lipoprotein receptors and, through its interaction with these receptors, participates in the transport of cholesterol and other lipids among the various cells in the body (1). The APOE gene is located at chromosome 19q13.2 and has three common variants (APOE*E2, APOE*E3, and APOE*E4; E2, E3, and E4, respectively) and six different genotypes (E2/E2, E2/E3, E2/E4, E3/E3, E3/E4, and E4/E4) (2, 3). Allelic variation of APOE has been shown to influence the levels of serum lipids. Previous studies have consistently shown that total cholesterol (TC) and low-density lipoprotein cholesterol (LDL-C) are highest in E4 carriers, intermediate in E3 carriers, and lowest in E2 carriers (4, 5); however, some reports have shown no effect of APOE genotype on LDL-C levels (6, 7). In contrast, the associations between APOE genotype and triglyceride and high density lipoprotein cholesterol (HDL-C) levels are less clear among different populations (5, 8). Moreover, the association between APOE genotype and lipid levels may be modulated by factors such as age, sex, ethnicity, diet, smoking behavior, alcohol consumption, and the presence of diabetes mellitus (3, 9, 10). The aim of this study was to evaluate the association between APOE polymorphisms and lipid levels in a Korean population, and to explore the gene-environment interactions in this population.
MATERIALS AND METHODS
Populations and study design
Potential participants for this study were recruited from residents of five administrative regions (three Myuns and two Dongs) of Namwon in the Jeonbuk Province of Korea. We used national resident registration lists to identify potential participants. The study area contained an estimated 4,697 people (2,142 men and 2,555 women) who were between 45 to 74 yr old in 2004, the age limits for eligibility for the study. Among these 4,697 eligible subjects, 1,964 (41.8%) underwent a clinical examination following an interview. The participants included 694 men and 1,270 women, and the mean (±standard deviation) ages of the men and women were 61.9 (±6.7) and 61.1 (±7.1) yr, respectively. The response rate of women (48.4%) was significantly higher than men (33.5%), but the difference of mean ages between the respondent and non-respondent was not significant in both sexes. Subjects with missing lipid measurements or lifestyle data, or with triglyceride levels ≥800 mg/dL (11) were excluded from the study. The APOE genotypes were categorized into three groups: APOE*E2 (E2/E2 and E2/E3), APOE*E3 (E3/E3), and APOE*E4 (E3/E4 and E4/E4). Subjects with the E2/E4 genotype (4 men and 12 women) were excluded because of the expected opposing biological effects of the E2 and E4 alleles. Ultimately, 1,900 subjects (668 men and 1,232 women) formed the final study sample for the principal analysis. All participants provided informed consent, and the study was conducted in accordance with the approval of the institutional research ethics committee.
Anthropometric measurements
Anthropometric measurements of subjects wearing light clothing and no shoes were conducted by experienced research staff. Height was measured to the nearest 0.1 cm, and weight was measured in the upright position to the nearest 0.1 kg. The body mass index (BMI) was calculated as weight divided by height squared (kg/m2). Waist circumference was measured to the nearest 0.1 cm at the end of a normal expiration by measuring from the narrowest point between the lower border of the rib cage and the iliac crest.
Lipid measurements
All the participants underwent at least 10 hr of overnight fasting before blood samples were obtained from an antecubital vein. Serum was separated on-site and was stored at -70℃ until analyzed. The concentrations of TC, HDL-C, and triglycerides were measured by an automatic analyzer (AU5400, Olympus, Japan), and LDL-C was estimated using the formula of Friedewald et al. (12). The fasting blood glucose level was measured using an enzymatic method.
Measurement of environmental factors
The questionnaire administered to all participants was designed to determine the history of type 2 diabetes mellitus and lifestyle factors such as alcohol consumption, smoking, and exercise habits. The subjects were categorized according to their smoking habits as current smokers, ex-smokers, and non-smokers. Type 2 diabetes mellitus was defined as a self-reported history (having been informed by a physician that diabetes was present) or as a fasting blood glucose level ≥126 mg/dL.
APOE genotyping
Genomic DNA was extracted from peripheral blood with a AccuPrep Genomic DNA Extraction Kit (Bioneer, Seoul, Korea) according to the manufacturer's protocol. APOE genotypes were determined as described by Hixson and Vernier, with slight modification (13). A 244-bp fragment of the APOE gene that spans the two polymorphic sites at codons 112 and 158 was amplified by polymerase chain reaction in a DNA thermal cycler (PTC-200; MJ Research, Inc, Watertown, MA, U.S.A.) using the primers 5'-ACA GAATTCGCCCCGGCCTGGTACAC-3'and 5'-TAAGCTTGGCACGGCTGTCCAAGGA-3'. The PCR amplifications were carried out in 10 µL reaction volumes containing 0.25 mM each dNTP, 1.5 mM magnesium chloride, 0.75 U of f-Taq polymerase (Solgent, Seoul, Korea), 50 ng of genomic DNA, and 0.25 µM of each of the primers. The PCR cycling conditions were 94℃ for 5 min, followed by 40 cycles of 94℃ for 30 sec, 65℃ for 40 sec, and 72℃ for 90 sec. A final extension phase of 5 min at 72℃ was included at the end of the protocol. The PCR products were digested with 5 units of HhaI (TaKaRa Co. Ltd., Kyoto, Japan) and the fragments were separated by electrophoresis in 10% polyacrylamide gels. After electrophoresis, the gels were treated with ethidium bromide and the DNA fragments were visualized using ultraviolet illumination.
Statistical analysis
The differences between sexes were compared using Student's unpaired t-test for continuous data and the chi-square test for categorical data. Chi-square tests were conducted to compare the differences between the observed and expected frequencies, assuming Hardy-Weinberg equilibrium. Because the distributions of TC and HDL-C were skewed, the data were log-transformed prior to the analysis. Analysis of covariance (ANCOVA) was carried out using the general linear model procedure to exclude the effects of potential confounders (such as age, BMI, waist circumference, smoking, alcohol consumption, exercise, and diabetes mellitus) on lipid levels. The interaction effect between the APOE allele and demographic (sex and age) and environmental (smoking, alcohol consumption, exercise, and diabetes mellitus) factors was tested by introducing corresponding interaction terms in the ANCOVA model. Bonferroni tests were applied to correct for multiple comparisons. All analyses were performed using SPSS software version 11.0 (SPSS, Chicago, IL, U.S.A.).
RESULTS
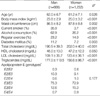
The descriptive characteristics of the study subjects are presented in Table 1. The percentages of men who were current smokers, consumed alcohol, engaged in regular exercise, or had diabetes mellitus were significantly higher than the corresponding percentages of women; however, women had significantly greater mean BMI and waist circumference figures than did men. The TC, LDL-C and HDL-C levels were significantly higher in women than in men, but the triglyceride levels were higher in men. The distribution of the APOE polymorphism in our study population was in Hardy-Weinberg equilibrium, and not significantly different in men and women. The genotype distribution was similar to those observed in other Korean studies (14, 15).
The relationship between the APOE genotypes and the serum lipid concentrations for male and female subjects is presented in Table 2. The APOE allele type had a significant effect on TC and LDL-C levels in both men and women (p<0.05). E2 carriers had significantly lower TC and LDL-cholesterol concentrations than did E3 or E4 carriers. The APOE allele type had no significant effect on HDL-C levels in men, but there was a linear trend (p=0.04). Among women, E2 or E3 carriers had significantly higher HDL-C levels than did E4 carriers. The APOE allele type had no significant effect on triglyceride levels in men; however, among women, E4 carriers had the highest and E3 carriers had the lowest triglyceride levels. The associations between the APOE allele and lipid levels were not modified by sex (Table 2).
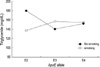
Table 3 shows the interaction effects between the APOE alleles and age and environmental factors in men and women. In women, the effect of the APOE allele type on HDL-C levels differed with age (Table 3). In women <60 yr old, E2 and E3 carriers had significantly higher HDL-C levels than did E4 carriers (Fig. 1). This pattern was similar to that in men (Table 1). In women ≥60 yr old, the APOE allele type still had a significant effect on HDL-C levels (p=0.049); E3 carriers tended to have higher HDL-C levels than E2 or E4 carriers, but there was no significant association of the APOE allele type with HDL-C levels after Bonferroni adjustment for multiple comparisons (result not shown). In addition, in men, the effect of APOE allele type on triglyceride levels was modified by smoking (Fig. 2). Among non-smokers, the triglyceride levels were highest in E2 carriers and lowest in E3 carriers. Among current smokers, E3 carriers had the highest triglyceride levels and E2 carriers had the lowest triglyceride levels, but these differences were not significant.
DISCUSSION
In this large population-based study, we have shown that APOE polymorphisms had a significant effect on lipid levels and that gene-environment interactions significantly affected lipid levels in a Korean population. We found that E2 carriers had significantly lower TC and LDL-C levels than did E3 or E4 carriers. This finding is consistent with previous studies, in which TC and LDL-C levels were the highest in E4 carriers, intermediate in E3 carriers, and the lowest in E2 carriers (5, 8, 16, 17). Our study also showed that E4 carriers tended to have higher TC and LDL-C levels than E3 carriers, although this difference was small and not significant. However, a metaanalysis (17) showed that subjects with E3/E4 and E4/E4 genotypes had significantly higher TC levels than did subjects with the E3/E3 genotype. Frikke-Schmidt et al. (8) found that there was a stepwise increase in cholesterol and apoB levels, in both sexes, as a function of genotype (E2/E2, to E2/E3, to E2/E4, to E3/E3, to E3/E4, to E4/E4) and alleles (E2, to E3, to E4). In a Singapore-based study (5), Tan et al. showed that E4 carriers had higher TC and LDL-C levels than did E3 carriers among ethnic Chinese, but that there were no significant allelotype-related differences among ethnic Malays or Asian Indians of either sex, with the exception of the LDL-C levels in ethnic Malaysian women. Therefore, differences in TC and LDL-C levels between E3 carriers and E4 carriers may be variable across populations.
Our study also showed that the APOE allele type had a no significant effect on HDL-C levels in men, although a negative linear trend (p=0.04) was present; however, in women, E2 and E3 carriers had significantly higher HDL-C levels than did E4 carriers. Frikke-Schmidt et al. (8) showed that there was a stepwise decrease in HDL-C in women, but not in men, according to allelotype, as described above. In the Singapore study (5), Tan et al. showed that E2 carriers had the highest HDL-C levels and E4 carriers had the lowest HDL-C levels in the three ethnic groups studied. However, a metaanalysis (17) showed that there was no clear association between HDL-C levels and the APOE allele type, apart from the finding that HDL-C levels were significantly lower in E3/E4 carriers than in E3/E3 carriers.
We showed that female E4 carriers and male E2 carriers had the highest triglyceride levels, and that E3 carriers had the lowest triglyceride levels. This finding is in accordance with previous studies (5, 8, 14, 17, 18). In a study of Korean men, Chun et al. (14) showed that APOE allele type was associated with the median serum triglyceride levels in descending order from E2/E3, to E3/E4, to E3/E3. In the Singapore study (5), Tan et al. showed that E4 carriers had higher triglyceride levels, as compared with E2 and E3 carriers, with the exception of ethnic Malaysian males, in whom triglyceride levels were the highest in E2 carriers. A meta-analysis (17) showed that triglycerides were higher in E2 carriers and E4/E3 carriers than in E3/E3 carriers. Frikke-Schmidt et al. (8) showed that E2/E2 and E4/E4 carriers had the highest triglyceride levels, whereas E3/E3 carriers had the lowest triglyceride levels in both sexes. The higher levels of triglycerides observed in subjects carrying the E2 allele can be explained by their slower plasma clearance of chylomicron and VLDL remnants (17, 19, 20).
The association between APOE polymorphism and triglyceride and HDL-C levels are not entirely clear among different populations (4, 5, 8, 21). Gene-environment interaction may contribute to the discrepancies observed between studies. We found that the association between the APOE alleles and HDL-C levels was modified by age in women, and that the association between APOE alleles and triglyceride levels was modified by smoking status in men, and tended to be modified by the presence of diabetes mellitus in women (p=0.051). Previous studies have shown that HDL-C levels vary with physical activity, alcohol consumption, and diet (9, 22). Reznik et al. (23) showed that the association between APOE polymorphism and postprandial triglyceride clearance was modified by age, body weight, and fasting TG pool level. Some previous studies have also shown that the association between APOE polymorphism and lipid levels was modified by sex (24), but in our study, the associations between the APOE allele types and lipid levels were not modified by sex, with the exception of an association of borderline significance (0.093) for triglyceride levels. However, the underlying mechanisms responsible for the gene-environment interactions found in the present study are not clear. Such interactions imply that, at the molecular level, there is synergy between gene products, or between gene products and the by-products of environmental insults, resulting in greater than additive effects (25).
The present study has some limitations. First, the relatively small sample size in men prevented us from showing statistically significant associations, although the patterns for TC and HDL-C levels that were observed in men were similar to those observed in women. Second, the proportion of the study population with risk factors such as smoking in women, diabetes mellitus, and the APOE*E2 or E4 alleles was low, and this limited the power of this study to detect gene-environment interactions.
In summary, we have shown that APOE polymorphisms had a significant effect on lipid levels in Koreans, that the association between the APOE allele type and HDL-C levels was modified by age in women, and that the association between the APOE allele type and triglyceride levels was modified by smoking status in men. These findings highlight the important effect of gene-environment interactions on lipid levels.



 XML Download
XML Download