

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Ectopic ovaries including accessory ovaries and supernumerary ovaries are rare gynecologic conditions. The incidence of these conditions was reported at 1:29,00-700,000 gynecologic conditions (1). Tumors arising in accessory ovaries are extremely rare. There are reports of various cases of tumors arising in accessory or supernumerary ovaries such as dermoid cyst, serous cystadenomas, mucinous cystadenomas, Brenner tumor, steroid cell tumor, and sclerosing stromal tumor (2-4). Because accessory and supernumerary ovaries develop from abnormal embryogenesis, congenital malformations or genetic abnormalities are seen in connection with them. Malformations include accessory fallopian tube, bifid fallopian tube, accessory tubal ostium, bicornuate and unicornuate uteri, septate uterus, agenesis of the kidney or ureter, agenesis of the fallopian tube, double urinary collecting system, bladder diverticulum, accessory adrenal gland, and lobulated liver (1, 2, 5-7).
CASE REPORT
A 33-yr-old woman with para 2-0-1-2 presented with a 5-month history of left lower quadrant pain. She had neither previous operations nor pelvic inflammatory disease. She completed two normal pregnancies when she was 26 and 28 yr old. The uterus which was slightly deviated to the right pelvic wall was of normal size and there was an indistinct irregular mass about 8×8 cm in size in the left adnexal area. The patient was admitted to the Department of Gynecology under the diagnosis of torsion of a left ovarian tumor.
CT scans showed a cystic mass with fat attenuation. Another small, fatty mass with foci of calcification was noted at the left posterior aspect of this mass. The right ovary appeared to be normal (Fig. 1).
An exploratory laparotomy was performed. On operation, two cysts were found. One was a 8×6 cm-sized dermoid cyst which was derived from the left eutopic ovary, and the other derived from a third ovary, the accessory ovary with 2×2.5 cm in size, was found in the left infundibulopelvic ligament adjacent to the retroperitoneum. There was no connection between the two ovaries. The right ovary appeared to be normal. Further anomalies including urogenital anomalies were not identified.
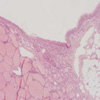
Grossly the eutopic ovary measured 8×8×6 cm in size and 160 g in weight. It was replaced by a cystic tumor containing a Rokitansky tubercle of 4×3×2.5 cm in size. The accessory ovary was measured 2.5×2×2 cm in size and 14 g in weight. Histologic examination of both eutopic and accessory ovary masses revealed teratoid components including mature thyroid tissue, repiratory epithelium, adipose tissue and epidermis (Fig. 2).
The patient's postoperative course was uneventful. The patient was discharged on the sixth postoperative day.
DISCUSSION
Accessory ovary was described in 1864 for the first time by Grohe (3). The incidence of accessory ovaries and supernumerary ovaries was reported to be very low 1:29,000-700,000 gynecologic admissions (1).
The distinction between accessory ovaries and supernumerary ovaries was defined in the Wharton's review. Wharton's criteria for a supernumerary ovary are; 1) the ovary must contain ovarian follicle tissue, and 2) the third ovary must be entirely separated from the normally located ovary and must arise from a separate primordium (8). We distinguish an accessory ovary from a supernumerary ovary by its relationship to the normal ovary (2). The accessory ovary which is supplied by vessels continuous with those of the eutopic ovary is connected to the infundibulopelvic ligament or the uteroovarian ligament. On the other hand, the supernumerary ovary is not (5, 8). In the present case, the accessory ovary was located on the left infundibulopelvic ligament adjacent to the retroperitoneum.
The ectopic ovaries may occur in two ways. First, in the embryonic theories, they are believed to result from abnormal separation of a small portion of the developing and migrating ovarian primordium (10). Secondly, the accessory ovary can occur from acquired conditions such as inflammation and operations. Part of ovarian tissue which had been detatched from the ovary could be implanted anywhere in the pelvic cavity. Experimental animal models have demonstrated that the detached and transplanted ovarian tissue may continue to function in vivo as autotransplanted splenic tissue in animals or humans (3). Mobius and Carol proposed that the ectopic tissue should arise from a trapping or cutting off of portions of a differentiated gonad by secondary peritoneal adhesion, synechia, or cicatizations (11). Lachman and Berman named the this ovarian implant (3).
Fewer than 50 cases of ectopic ovary have been reported in the literature and only in two cases the diagnosis was establised prior to the operation. In the remaining cases including the present case, the ectopic ovary was an incidental finding on autopsy or on operation (7). The ectopic ovarian tissue can function as normal ovaries and can also cause pathologic abnormalities (1, 2). Only two cases which were suspected preoperatively had regular menstrual bleeding after bilateral oophorectomy carried out due to breast cancer. Gonadotropin was used to stimulate the ectopic ovarian tissue to aid in the finding of the location of the ovarian tissue at the time of laparotomy (5, 7).
Reported locations of accessory and supernumerary ovaries have been the mesosalpinx near the fornix, the posterior wall of the bladder, the posterior cul-de-sac, the retroperitoneum next to the aorta and psoas muscle, colon, distal ileum, in the omentum and in the mesentery, and the upper abdominal cavity (14, 15). Some accessory ovaries were confused with lymph nodes, because the most of accessory ovarian tissue measured up to less than 1 cm (1, 5). Therefore the ocurrence rate of accessory ovary may be more common than those reported (1, 9). On the other hand, the diameter of the supernumerary ovary is variable from a few millimeters to several centimeters (12).
To date, the literatures report various cases of tumors arising in accessory or supernumerary ovaries, such as dermoid cyst, serous cystadenoma, mucinous cystadenoma, Brenner tumor, steroid cell tumor, and sclerosing stromal tumor (2, 4, 11). Thus, it may be brought to a conclusion that the various types of neoplasms that occur in accessory or supernumerary ovaries are similar to that in eutopic ovaries. To our knowledge, we report the first case of two dermoid cysts developed in a an accessory ovary located in left infundibulopelvic ligament and an eutopic ovary at same side concurrently.
Dermoid cyst is common benign cystic tumor. In general, the overall incidence of dermoid cyst is unknown. It is frequently found in childhood and in young women (16). More than 80% of dermoid cysts occur during the reproductive years (17). A totipotential single germ cell may develop in benign ectoderm, mesoderm, or endoderm and may transform into malignancy such as a squamous cell carcinoma, adenocarcinoma, spindle-cell sarcoma, trabecular carcinoid (18-20). Thus they are often lined with epithelium like the epidermis and contain skin appendage, teeth, sebaceous material, hair, and nervous tissue. Endodermal derivatives include the thyroid, the bronchus and the intestine, and the mesoderm may be represented by bone and smooth muscle. The risk of torsion of the dermoid cysts is approximately 15%. Approximately 60% of most mature teratomas are asymptomatic (21). In the CT findings, a fat attenuation within the cyst, calcification or teeth in the wall is diagnostic for dermoid cyst. In the ultrasonography, imaging features are usually composed of a cyst with echogenic tubercle, a diffusely or partially echogenic mass with shadowing, and multiple echogenic bands in the cystic cavity. Conventional therapy is a surgical extirpation of the tumor and has a very favorable outcome. Ovarian cystectomy is almost always possible, even if ovary appears to have only a small amount of ovarian tissue left. Preserving a small amount of ovarian cortex in a young patient with a benign lesion is preferable compared to the loss of the entire ovary (22).
In 23% of the reported cases, congenital malformations or genetic abnormalities are seen in connection with both accessory and supernumerary ovaries (1, 8). Defects have included accessory fallopian tube, bifid Fallopian tubes, accessory tubal ostium, bicornuate and unicornuate uteri, septate uterus, agenesis of kidney or ureter, agenesis of fallopian tubes, double urinary collecting system, bladder diverticulum, accessory adrenal gland and lobulated liver (1, 2, 5-7, 13). There was no defect in our case.

 XML Download
XML Download