

 PDF
PDF Citation
Citation Print
Print


Vertebral compression fractures (VCFs) cause severe pain and spinal instability, devastating patients' quality of life [1]. Vertebroplasty (VP) is a very effective treatment modality that lessens fracture-induced pain and spinal instability, and enables patients to return to their normal activities [2,3]. However, VP can result in complications such as direct nerve damage, pulmonary embolism, and adjacent vertebral fractures [4,5].
Adjacent fractures are particularly bothersome for practitioners because they can occur even after a successful procedure. Adjacent fractures are thought to be caused by an excessive increase in the rigidity of augmented vertebrae [6], and some doctors insist that injecting only a small volume of bone cement (polymethylmethacrylate, PMMA) can prevent adjacent fractures. However, there is not yet a consensus on the optimal volume of PMMA to inject. Furthermore, a volume of injected cement that is too small can be ineffective in controlling pain, and refracture of the augmented vertebra can occur.
In our practice, we encountered a patient with persistent pain and immobility after VP and subsequent refracture of the treated vertebral body. We performed an additional VP with sufficient PMMA to fill the fractured area, which resulted in significant pain relief and resolution of the patient's immobility. We present this case here, along with a review of the literature.
CASE REPORT
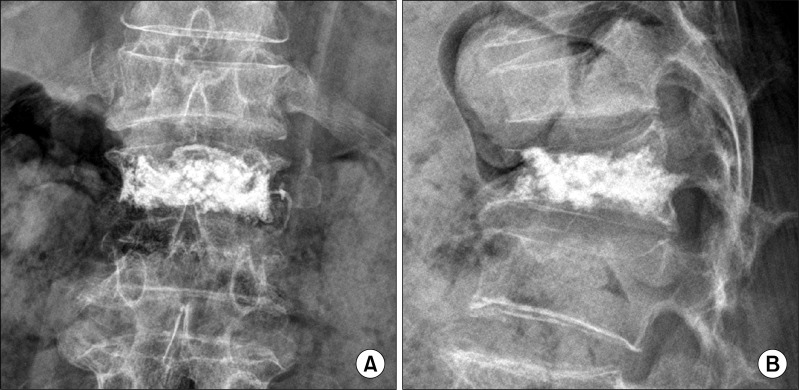
A 65-year-old female presented to our pain clinic complaining of low back pain. A month earlier she had experienced pain in the low back and right flank area, and was diagnosed with osteoporotic VCF in the first and fourth lumbar vertebral bodies (L1 and L4). Unipedicular VPs were performed with the injection of 2 ml and 2.5 ml of PMMA into each vertebra, respectively (Fig. 1). After the procedure, the visual analogue scale (VAS) reduced from 10 to 8, and her flank pain subsided. This state continued without additional pain relief.
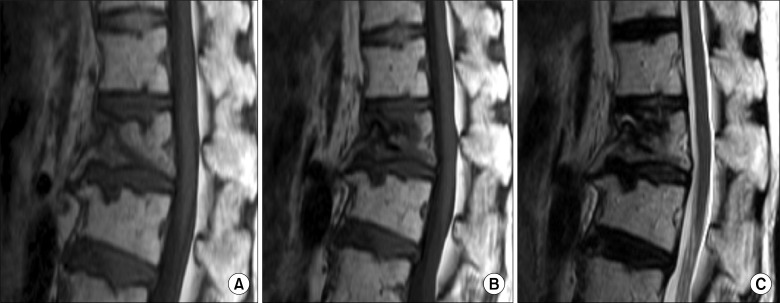
Several days before her visit to our clinic, the patient's back pain worsened and became aggravated when sitting, standing up, or changing her posture (VAS 10). She was also unable to stand or walk unassisted. On physical examination, only tenderness of the L1 spinous process was present and there were no neurological abnormalities. An interval progression of anterior wedging in the L1 vertebral body was detected on lumbar plain radiograph, and MR images showed findings consistent with the refracture of L1 (Fig. 2). Based on these results, we concluded that the previous VP in L1 had failed to relieve her pain and that refracture of L1 worsened the symptoms. We therefore proceeded to repeat VP in the L1 vertebra.
After obtaining informed consent from the patient and her family, repeat VP was performed in the L1 vertebral body using a bipedicular approach with the patient in the prone position. When the bone fillers reached the fractured cavity of the L1 vertebral body, we then slowly injected 3.5 ml of PMMA bone cement on each side under real-time C-arm fluoroscopic guidance to prevent cement leakage and to ensure even dispersion of cement in the fractured lesion (Fig. 3). No cement leakage or dislocation of the previous injectate was detected. During the VP procedure, blood pressure, EKG, and mixed venous oxygen saturation were monitored, and oxygen was supplied via nasal cannula. In addition, a total of 100 mcg fentanyl was administered intravenously for analgesia.
The day after the procedure, the patient's VAS dropped from 10 to 4, and she reported only discomfort in the procedure area. She was also able to walk unassisted, and was therefore discharged on that day. When she visited our clinic a month after the repeat VP, her pain and immobility had resolved completely.
DISCUSSION
VP is effective for managing pain and immobility caused by vertebral compression fractures. However, pain can recur in 1.8-15.6% of patients after VP, which is attributable to rib fracture, infection, non-healing bone-cement interface, or new symptomatic compression fractures [7]. In addition, inadequate impactions of bone cement can make the unfilled intravertebral spaces collapse or the injectates loosen after procedures [6].
Currently, there is no consensus on the adequate volume of bone cement to inject during VP. Some practitioners prefer to inject a small volume of bone cement. Belkoff et al. reported that 2 ml of bone cement is enough to recover the strength of fractured vertebrae [8]. In a biomechanical study using cadavers, a small volume of injected bone cement normalized the distribution of compressive stress on the fractured and adjacent vertebrae [9]. Other researchers have also reported finding no correlation between the injected cement volume and the degree of pain relief [10,11]. In addition, injection of a large volume of PMMA increases the risk of adjacent fractures and cement leakage from the vertebral body, leading to complications such as epidural hemorrhage, spinal cord injury, and acute respiratory distress [4,5,10,12].
On the other hand, He et al. performed additional VPs for 15 patients whose pain persisted after VP, and commented that a sufficient volume of injected PMMA was the most important factor predicting patient prognosis [13]. Kim et al. reported that cement volume was not related to the incidence of subsequent vertebral compression fractures and recommended injecting the largest possible volume of bone cement [14].
In our case, previous VP with small volume PMMA impaction failed to relieve the patient's symptoms, and subsequent refracture of the vertebra on which the procedure was performed worsened her problems. The results of our case clearly confirmed that small volume VP can be ineffective, and the patient's pain and immobility worsened as a result of subsequent refracture to the augmented vertebra.
The optimal volume of PMMA to inject into fractured vertebrae remains controversial. In addition, further studies are needed to investigate long-term patient prognosis and the biomechanics of fractured vertebral bodies. However, in our opinion, it seems appropriate to fill fractured vertebral bodies with a sufficient volume of bone cement that is within the limits of leakage, rather than a small volume of PMMA, in order to improve the patient's prognosis.
In conclusion, VP with small volume bone cement impaction may fail to relieve fracture-induced symptoms and to prevent refracture of an augmented vertebral body. Also, in case of refracture of procedure vertebra, repeat VP can effectively treat unresolved symptoms.

 XML Download
XML Download