

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
There is now ample evidence of an association between preformed antibody to HLA and vascular rejection in kidney transplantation (KT) [123]. A recent study demonstrated the possibility of antibody-mediated injury without donor-specific HLA antibody (HLA-DSA) production, suggesting a role of antibodies against non-HLA antigens expressed on the renal allograft tissue [4].
Among the various types of non-HLA antibodies, angiotensin II type 1 receptor antibodies (anti-AT1Rs) and the MHC class I-related chain A antibodies (anti-MICAs) have been the most widely studied [56]. AT1R is a G-protein-coupled receptor that mediates the actions of angiotensin II, including blood pressure regulation and water-salt balance, and anti-AT1Rs may be formed as a result of inflammation, injury, sensitization, or non-compliance to medication [7]. Polymorphic MICA molecules are constitutively expressed on vascular endothelial cells, and previous experiments revealed that increased MICA expression levels were associated with hypoxic stress conditions accompanying transplantation [8]. Although the adverse effects of anti-AT1Rs or anti-MICA on allograft outcomes have been demonstrated in several studies [91011121314], the clinical significance of pre-transplant non-HLA antibodies remains controversial, and studies on the association between non-HLA antibodies and histological outcomes are limited.
We investigated the comparative impact of the presence of pre-transplant non-HLA antibodies (anti-AT1Rs and anti-MICAs) and HLA-DSA on clinical and histological outcomes in KT patients.
METHODS
1. Study population
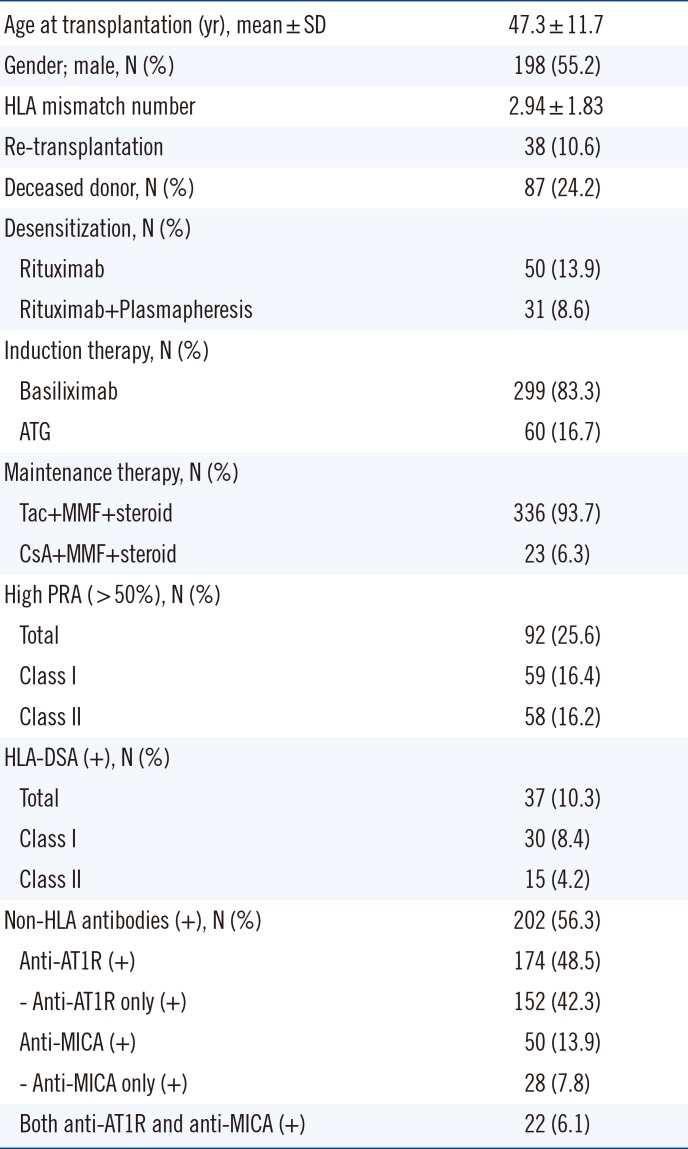
Between March 2010 and September 2014, a total of 475 patients received KT at Seoul St. Mary's Hospital, Korea. Among them, 116 patients were excluded for the following reasons: 65 ABO-incompatible KT patients, five patients who died with a functioning graft, three patients who underwent simultaneous KT and bone marrow transplantation, one patient who underwent simultaneous KT and pancreas transplantation, and 42 patients without available pre-transplant serum samples. Therefore, a total of 359 patients were finally enrolled in this study, and 253 were subjected to either protocol (N=121) or indication biopsy (N=132). The median follow-up duration for graft survival was 32.0 (95% confidence interval [CI]: 29.5–35.0) months. Patients' baseline characteristics are presented in Table 1. This study was approved by the Institutional Review Board of Seoul St. Mary's Hospital (KC13TNMI0701). All patients provided written informed consent.
2. Pre-transplant immunologic work-up and immunosuppressive regimen
Pre-transplant immunologic workup was performed as described previously [15]. In brief, we performed panel reactive antibody (PRA)-Luminex screening and cross-match (XM) testing using complement-dependent cytotoxicity (CDC), CDC-anti-human globulin, and flow cytometric XM in all patients. In patients with positive PRA or positive XM test results, we investigated the presence of HLA-DSA using a Luminex single-antigen assay (One Lambda, Canoga Park, CA, USA). Desensitization therapy was performed on living donor transplant patients who tested positive for pre-transplant HLA-DSA and/or T cell or B cell XM, as described previously [15]. In brief, rituximab (RTX) at a dose of 375 mg/m2 (MabThera Genentech, Inc., San Francisco, CA, USA) was administered two to three weeks before transplantation, and plasmapheresis/intravenous immunoglobulin (PP/IVIG) therapy was initiated 13 days prior to transplantation and administered every 48 hours. Tacrolimus (Tac) or cyclosporin A (CsA) was administered in combination with mycophenolate mofetil and prednisolone as a maintenance immunosuppressant (IS) regimen, with Tac as the main IS in all HLA-DSA (+) patients regardless of desensitization and median fluorescent intensity (MFI) strength. Basiliximab or anti-thymocyte globulin was administered as induction therapy.
3. Detection of anti-AT1Rs and anti-MICAs
Pre-transplant anti-AT1R and anti-MICA was assessed for all 359 patients, using serum samples taken before the initiation of IS. Serum anti-AT1R levels were measured using the EIA-AT1R kit (One Lambda). Microtiter 96-well polystyrene plates were coated with AT1R, and 100 µL of diluted samples were incubated at 2–8℃ for 2 hours according to the manufacturer instructions. After washing, the plates were incubated for 60 minutes with 100 µL horseradish peroxidase-labeled anti-human IgG. After incubation with 100 µL tetramethylbenzidine substrate for 20 minutes, the optical absorbance of each well was measured at 450 nm. Concentrations of anti-AT1Rs were determined based on the calibration curve, in which 10 U/mL was considered to be the cut-off value following the manufacturer's recommendation, similar to some previous studies [916]. Anti-MICA was measured using the LABScreen Mixed assay (One Lambda) on a Luminex platform according to the manufacturer's specifications. MICA alleles *001, *002, *004, *007, *009, *012, *017, *018, *019, and *027 were coated in microbeads.
4. Histological examination of renal allograft biopsy
Protocol biopsy was performed at three months post-transplant in 121 patients after obtaining consent. Indication biopsy was performed in patients with a 20% increase in serum creatinine above the baseline value at any time post-transplant. The mean time to indication biopsy was 5.7±9.8 months. The biopsies were performed as described in our previous study [17], using a 16-gauge biopsy gun under ultrasonic localization. Histopathological diagnosis was made based on the revised Banff working classification [18]. The microvascular inflammation (MVI) score was defined as the sum of the glomerulitis (g) and peritubular capillaritis (ptc) scores. The threshold for moderate MVI (g+ptc≥2) was used to determine the association of antibodies with MVI, which has been applied for the diagnosis of C4d(−) acute antibody-mediated rejection (ABMR) in the revised Banff criteria [18].
5. Statistical analysis
Continuous variables are presented as mean±SD, and categorical variables are summarized as number and percentages. Continuous variables were compared using the Student's t-test, and categorical variables were compared using the chi-square test or Fisher's exact test. Allograft survival among groups was compared using Kaplan-Meier analysis with a log-rank test. Risk factors for MVI were determined by odds ratios (OR) using a multivariable logistic regression analysis. Risk factors affecting allograft outcomes were determined by hazard ratios (HR) using a Cox regression multivariate analysis. Statistical analysis was performed using SPSS version 20 for Windows (SPSS Inc., Chicago, IL, USA) and MedCalc version 15.5 (MedCalc, Mariakerke, Belgium). P<0.05 was considered statistically significant.
RESULTS
1. Prevalence of HLA-DSA, anti-AT1R, and anti-MICA in pre-transplant sera
As shown in Table 1, pre-transplant HLA-DSA was detected in 37 of the 359 KT patients (10.3%), with more patients producing class I than class II. Moreover, pre-transplant anti-AT1R was detected in 174 patients (48.5%), and pre-transplant anti-MICA was detected in only 50 patients (13.9%). Of the 37 HLA-DSA (+) patients, 21 patients (56.8%) were anti-AT1R (+) and five patients (13.5%) were anti-MICA (+). Of the 322 HLA-DSA (−) patients, 153 patients (47.5%) were anti-AT1R (+) and 45 patients (14%) were anti-MICA (+).
2. Association of pre-transplant antibodies with histological diagnosis of allograft biopsy
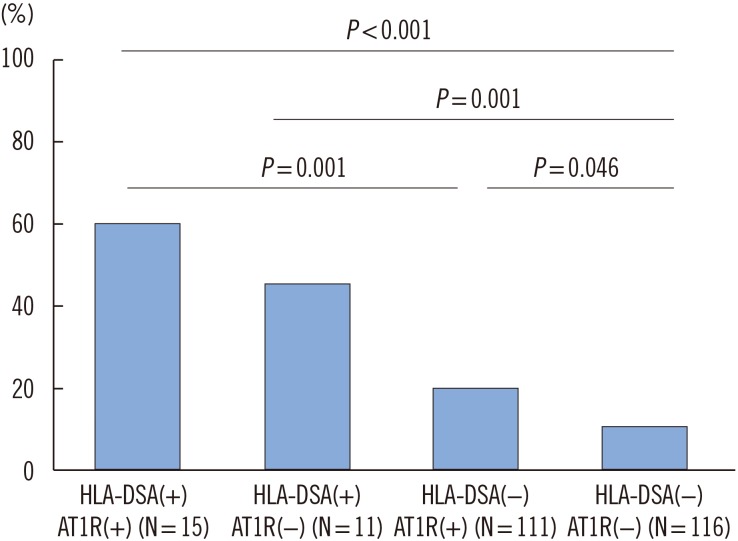
There was a higher prevalence of ABMR in the HLA-DSA (+) patients (9/26, 34.6%) compared with that in the HLA-DSA (−) patients (8/227, 3.5%) (P<0.001). However, no significant difference in ABMR frequencies was detected between pre-transplant anti-AT1R (+) and (−) patients (10/126 [7.9%] vs 7/127 [5.5%]) or anti-MICA (+) and (−) patients (3/35 [8.6%] vs 14/218 [6.4%]). In addition, T cell-mediated rejection (TCMR) development was not associated with the presence of pre-transplant HLA-DSA, anti-AT1R, or anti-MICA. The prevalence of MVI was significantly higher not only in HLA-DSA (+) patients compared with HLA-DSA (−) patients (14/26 [53.8%] vs 34/227 [15.0%]; P<0.001) but also in anti-AT1R (+) patients compared with anti-AT1R (−) patients (31/126 [24.6%] vs 17/127 [13.4%]; P=0.023). In HLA-DSA (+) anti-AT1R (−) patients and HLA-DSA (−) anti-AT1R (+) patients, the mean durations to MVI development were similar at 11.2±20.1 months and 8.4±10.7 months, respectively. Patients with both HLA-DSA and anti-AT1R showed a relatively earlier onset of MVI (2.1±3.4 months post-transplant), but this difference was not statistically significant. However, MVI was detected most frequently in patients with both HLA-DSA and anti-AT1R (Fig. 1; P<0.001, chi-square for trend). Among the 48 patients with MVI, 17 (35.4%) were diagnosed as having ABMR based on the revised Banff criteria. There was also no significant difference in the frequency of MVI development between anti-MICA (+) and anti-MICA (−) patients (9/35 [25.7%] vs 39/218 [17.9%]). There were no statistically significant associations of each antibody with individual Banff classification scores (g, ptc, and C4d); however, the anti-AT1R (+) and anti-MICA (+) groups also showed a tendency toward higher g and ptc scores, but not C4d scores.
The frequencies of de novo DSA (dn DSA) development were not significantly different between pre-transplant anti-AT1R (+) (7.9%, 5/63) and anti-AT1R (−) patients (5.2%, 3/58). In addition, the time to detection of dnDSA did not vary according to the pre-transplant anti-AT1R status. All five patients with dnDSA that were pre-transplant anti-AT1R (+) showed MVI, and three patients showed ABMR.
3. Multivariate analysis of pre-transplant risk factors for MVI in allograft biopsy
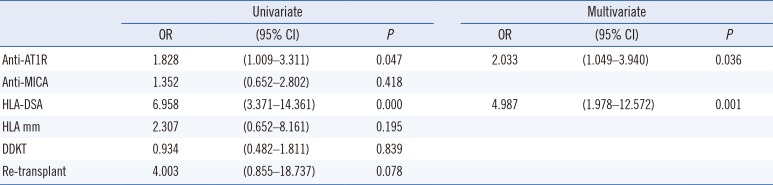
Among the 253 biopsies analyzed, both anti-AT1R and HLA-DSA proved to be significant risk factors for MVI (Table 2). When we performed subgroup analysis for the indication and protocol biopsy groups, both HLA-DSA (OR 4.802, 95% CI [1.46–15.726]; P=0.010) and anti-AT1R (OR 2.694, 95% CI [1.086–6.678]; P=0.032) emerged as significant risk factors for MVI in the indication biopsy group. However, in the protocol biopsy subgroup, only HLA-DSA was a significant risk factor for MVI (OR 8.810, 95% CI [1.656–46.877]; P=0.011).
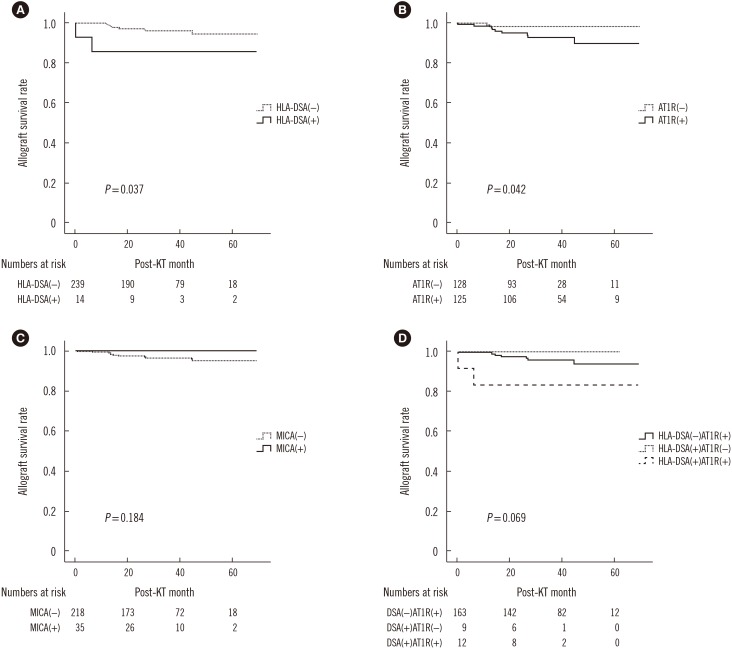
4. Effects of pre-transplant antibodies on allograft survival rate
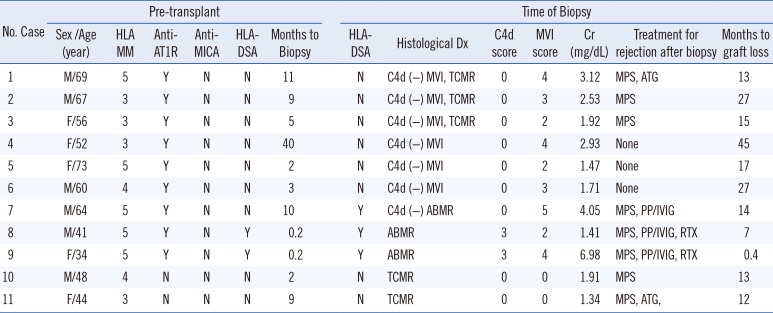
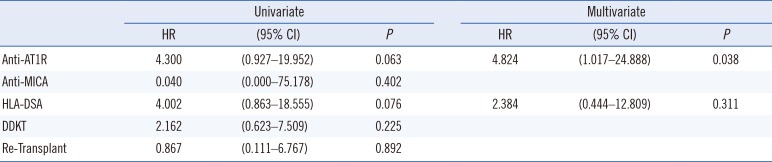
Patients that were HLA-DSA (+) showed significantly poorer allograft survival compared with HLA-DSA (−) patients (Fig. 2A, P=0.037). Similarly, anti-AT1R (+) patients showed significantly inferior graft survival compared with anti-AT1R (−) patients (Fig. 2B, P=0.042). However, there was no significant difference in graft survival between the anti-MICA (+) and anti-MICA (−) groups (Fig. 2C). There was also no statistically significant synergic effect of HLA-DSA and anti-AT1R on graft survival. Overall survival was poorest in the HLA-DSA(+)AT1R(+) group (Fig. 2D). Nine of the 11 patients who suffered from allograft failure (81%) were anti-AT1R (+), whereas only two (18%) were HLA-DSA (+) pre-transplant (Table 3). All nine anti-AT1R (+) patients with allograft failure presented with MVI on allograft biopsy, including three patients (no. 7, 8, 9) diagnosed as having ABMR (33.3%), and the other six patients exhibited C4d(−) MVI (66.6%). The average duration to failure of the C4d(−) MVI patients was 24±11.9 months. Cox regression multivariate analysis showed that anti-AT1R was the only significant risk factor for the development of allograft failure (HR 4.824, 95% CI [1.017–24.888], P=0.038) (Table 4).
DISCUSSION
Our study demonstrates that pre-transplant anti-AT1R is a significant risk factor for the development of MVI in allograft biopsy, and that it contributes to poor post-KT allograft survival.
First, we investigated the prevalence of each antibody at the pre-transplant phase. Previous reports have shown an incidence of anti-AT1R (+) status in the range of 10.0–47.2% [791119]. We detected pre-transplant anti-AT1R antibodies in 48.5% of patients, which is similar to the results of Giral et al [9], and to a recent study reporting a 59.0% rate of anti-AT1R (+) [20]. The incidence of pretransplant anti-MICAs has been reported to be approximately 7.2–25% [1321]. We could not find any association between the detection of anti-HLA antibodies (HLA-DSA) and non-HLA antibodies.
Next, we investigated the impact of each antibody at the pre-transplant stage on the risk of the post-transplant development of ABMR and MVI. The presence of pre-transplant HLA-DSA is a well-known major risk factor for antibody-mediated allograft injury [5152223], which was confirmed in the present study. Pre-transplant AT1R detection was an independent risk factor for the development of MVI. Activation by anti-AT1R increases pro-inflammatory protein expression, thereby stimulating the recruitment of inflammatory cells [142425]. These processes can result in the development of peritubular capillaritis and glomerulitis. Moreover, endothelial cell damage caused by anti-AT1R is not mediated by complement activation but rather through ERK1/2 followed by AP-1 and NF-κB, resulting in the activation of MCP-1 and RANTES and in the up-regulated expression of the tissue factor [62627]. Therefore, C4d deposition in the peritubular capillary is rarely detected in these cases, and the ABMR due to anti-AT1R presents most often as C4d(−) MVI, which was detected in the present study (Table 3).
Interestingly, we also found that MVI was most frequently detected in patients with both HLA-DSA and anti-AT1R, suggesting the synergistic impact of the two antibodies; it supports previous reports showing that HLA-DSA and non-HLA antibodies may function in synergy [1114]. An explanation for this synergistic impact may be that the pro-inflammatory environment induced either by HLA-DSA or anti-AT1R can encourage further up-regulation of AT1R or HLA expression [142425]. In our study, there was no difference in the time to detection of dnDSA at the time of indication biopsy with respect to the pre-transplant anti-AT1R status. This is in contrast to the findings of Cuevas et al [28], who reported that a high pre-transplant anti-AT1R level was an independent risk factor for earlier dnDSA detection after KT. Further follow-up studies are needed to clarify the association between pre-transplant anti-AT1R (+) status and dnDSA development.
Finally, we investigated the impact of each antibody on post-transplant allograft survival rates, and found that recipients with pre-transplant anti-AT1R showed poorer allograft survival. However, HLA-DSA did not emerge as a significant risk factor for allograft failure in our study. The detrimental effects of preformed HLA-DSA are well-known; therefore, desensitization therapies are initiated in patients when pre-transplant HLA-DSA is detected [1529]. Moreover, in patients that are HLA-DSA (+) at the pre-transplant stage, MVI usually presents as early ABMR, combined with rapid deterioration of allograft function. Therefore, early intervention would be performed in these patients along with desensitization therapy [3031]. In contrast, in patients that are pre-transplant anti-AT1R (+), detection of C4d (−) MVI without HLA-DSA at the time of biopsy could not be diagnosed as ABMR. In addition, allograft injury due to anti-AT1R occurs via a chronic damaging process, and the clinical course is usually indolent [4]. Therefore, aggressive therapy is not performed in such cases, which might result in the progression of chronic allograft injury leading to poorer allograft outcomes.
In contrast to anti-AT1R, anti-MICA did not show a significant impact on any post-transplant outcome, supporting a previous study, which suggested that the role of anti-MICA was questionable under sufficient immune suppression [32]. The current practice guideline does not recommend routine typing for anti-MICA in KT patients [33]. Further studies including MICA genotyping and determination of donor specificity are needed to clarify these effects.
The main limitation of this study is its retrospective cohort design. Therefore, we were not able to measure non-HLA antibody levels in the patients at the time of allograft biopsy. Given that a previous study found an association of anti-AT1R at the time of biopsy with antibody-mediated injury [34], further randomized controlled studies on the monitoring of anti-AT1R antibodies are required to reinforce our findings.
In conclusion, anti-AT1R, but not anti-MICA, detected before KT may be an important risk factor for allograft failure, which could be mediated by the induction of MVI in the allograft tissue. Hence, development of C4d(−) MVI might require more aggressive anti-humoral therapy in patients with pre-transplant anti-AT1R.
 XML Download
XML Download