

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor,
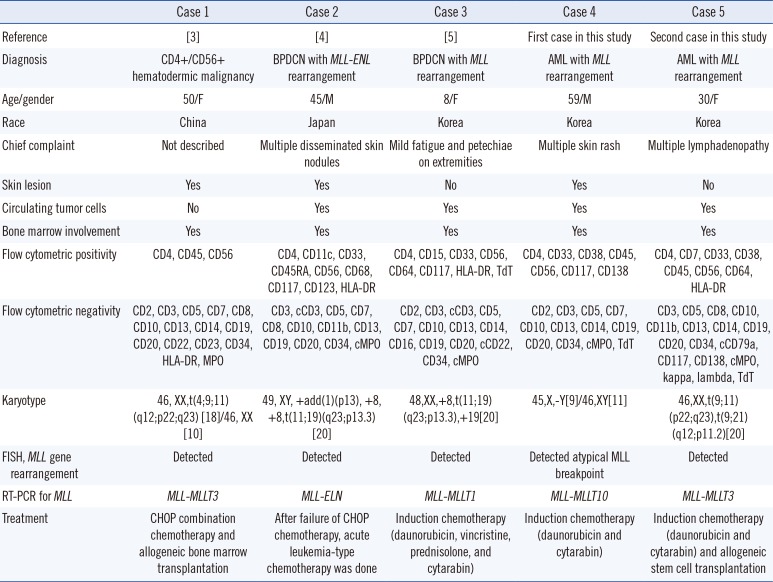
Blastic plasmacytoid dendritic cell neoplasm (BPDCN), characterized by co-expression of CD4 and CD56 without any other lineage-specific markers, is an aggressive tumor type that shows a high frequency of skin involvement and nodal or marrow infiltration with a propensity toward leukemic dissemination [1].This disease was formerly defined by the World Health Organization as blastic NK-cell lymphoma, and was later grouped with AML and related precursor neoplasms [2]. Here we report two AML cases with KMT2A (or MLL) rearrangements along with CD4+/CD56+ expression, which had the potential to be misdiagnosed as BPDCN.
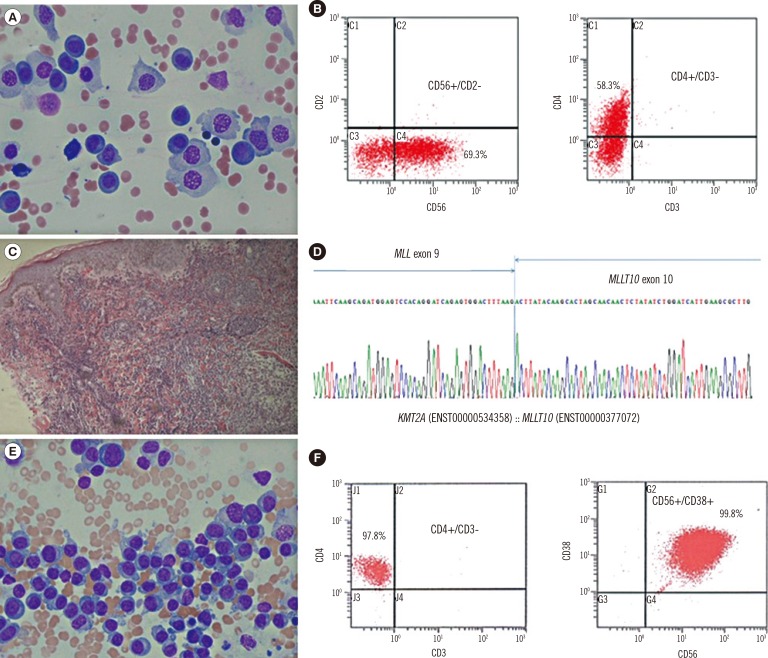
A 59-yr-old man presented with erythematous papules and vesicles on his whole body for one week. Complete blood counts showed anemia (Hb, 80 g/L), thrombocytopenia (62×109 platelets/L), and many circulating plasmoblast-like cells (65%). Bone marrow examination showed hypercellular marrow (90%) mostly composed of plasmoblast-like cells with coarse nuclear chromatin, distinct nucleoli, and abundant basophilic cytoplasm (Fig. 1A). Flow cytometry revealed that the neoplastic cells were positive for CD4, CD33, CD38, CD56, CD117, and CD138 (Fig. 1B), and negative for other myeloid or lymphoid markers (Table 1). Skin lesions showed diffuse infiltration of medium- to large-sized agranular blastic cells with CD4 and CD56 co-expression (Fig. 1C). Bone marrow and skin were negative for CD123 immunohistochemical stain. The chromosome study revealed 45,X,-Y[9]/46,XY[11] without 11q23 abnormalities. Multiplex, nested reverse transcription (RT)-PCR was performed for screening and detection of 28 chromosomal translocations using the HemaVision kit (DNA Technology, Research Park, Aarhus, Denmark), and the presence of MLL-MLLT10 rearrangement was demonstrated. It was confirmed by direct sequencing (Fig. 1D). Fluorescence in situ hybridization for MLL rearrangement revealed nuc ish(5'MLLx3,3'MLLx2)(5'MLL con 3'MLLx2)[170/200], suggesting the presence of an atypical MLL breakpoint. Although the lineage antigens expressed here were not specific to AML, he was diagnosed as having AML with MLL rearrangement in bone marrow and skin.
A 30-yr-old woman presented with multiple lymphadenopathy for three weeks. Laboratory analysis revealed anemia (Hb, 81 g/L), thrombocytopenia (82×109 platelets/L), and leukocytosis (16.77×109 white blood cells/L) with circulating plasmacytoid cells (63%). Neither skin lesion nor monoclonal gammopathy was present. Bone marrow analysis showed hypercellular marrow (100%) with leukemic cells containing abundant basophilic cytoplasm (Fig. 1E). Flow cytometry revealed that the neoplastic cells were positive for CD4, CD7, CD33, CD38, CD56, and CD64, (Fig. 1F), and were negative for other markers (Table 1). The cytochemical stain for non-specific esterase in neoplastic cells was negative. Immunohistochemical stains of bone marrow biopsy specimens showed that the neoplastic cells were negative for CD123, CD138, kappa, and lambda. Lymph node biopsy analysis demonstrated that the neoplastic cells co-expressing CD4 and CD56 were negative for CD123. Cytogenetic analysis revealed 46,XX,t(9;11)(p22;q23),t(9;21)(q12;p11.2)[20]. The MLL-MLLT3 rearrangement was detected by RT-PCR. Although adequate lineage-specific markers were not observed, she was diagnosed as having an AML with MLL rearrangement in bone marrow and lymph nodes.
So far, three cases of CD4+/CD56+ hematologic malignancies with MLL rearrangements have been reported as rare cases of BPDCN with MLL rearrangement (Table 1). The leukemic cells reported in the literature expressed the myeloid and monocytic markers CD33, CD117, CD11c, CD15, or CD64, which were not specific enough to identify a specific lineage [345]. These three cases did not express highly specific plasmacytoid dendritic cell-associated antigens, such as CD123, TCL1, CD2AP, or CD303 (BDCA2); therefore, additional immunohistochemical studies were necessary at their diagnosis. Variable expression of CD4 or CD56 in adult AML cases with MLL rearrangement has been reported [6], and BPDCN is often confused with monocytic leukemias. Based on the limited information on immunophenotypes of these cases, MLL-related monocytic leukemia would be a reasonable diagnosis (Table 1).
This study emphasizes that the diagnosis of BPDCN should only be considered after a full investigation of plasmacytoid dendritic cell markers, ensuring there is no expression of myeloid or monocytic markers on the blasts [7]. Since hematologic neoplasms such as BPDCN, AML, extranodal NK/T cell lymphoma, nasal type, and mature T cell lymphomas with or without skin involvement may express CD56 with or without CD4, extensive immunohistochemical and genetic analyses are necessary before definitively diagnosing BPDCN or AML [89].
In conclusion, CD4+/CD56+ hematologic malignancies can be suspected to be BPDCN, and clinicians should conduct a full analysis including flow cytometry for adequate myeloid/monocytic markers, immunohistochemical stain for highly specific plasmacytoid dendritic cell-associated antigens, cytogenetic, and genetic studies to make an exact diagnosis and determine effective treatment.
 XML Download
XML Download