

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Assessment of residual disease burden is important for AML patients who had received chemotherapy, because the residual disease status of these patients has been correlated with their clinical course [1234,5678]. Currently, flow cytometric residual disease monitoring, using specific aberrant expression markers found at diagnosis, reportedly has less clinical relevance in AML than in ALL [19,1011]. Specific cytogenetic abnormalities found in patients at AML diagnosis are good candidates as residual disease monitoring markers at patient follow-up. However, the frequency of cytogenetic abnormalities detected at AML diagnosis is approximately 55% [121314], which significantly hinders their use as a general residual disease monitoring method.
Molecular assessment of specific mutation burdens detected at diagnosis using real-time quantitative PCR (RQ-PCR) could be another candidate for residual disease monitoring in AML, especially in patients with a normal karyotype (NK) [1516171819], since the sensitivity of real-time PCR is higher than that of flow cytometry and conventional karyotyping. The frequently detected molecular aberrations in NK-AML include nucleophosmin (NPM1), Fms-related tyrosine kinase 3 internal tandem duplication (FLT3 ITD), and CCAAT/enhancer binding protein alpha (C/EBPα) mutations [202122]. Compared with FLT3 ITD and C/EBPα mutations, which have been reported to be relatively unstable during follow-up, the assessment of NPM1 mutation burden has been regarded to be more beneficial for the purpose of residual disease monitoring owing to its higher frequency in NK-AML and its demonstrated higher stability during follow-up [4567232425]. However, the comprehensive correlation analysis to evaluate the relationship between the NPM1 mutation burden and the results of BM assessment at diagnosis and follow-up in AML patients has not been widely performed. In the present study, we evaluated whether the NPM1 type A mutation (NPM1-mutA; TCTG insertion at the 960th nucleotide in exon 12) burden (as quantitated by RQ-PCR) correlates with the clinical status of AML patients bearing the allele mutation, and whether it could predict patient outcome, which would be useful in residual disease monitoring.
METHODS
1. Patients and samples
Twenty-seven NK-AML patients with NPM1-mutA (demonstrated by direct sequencing at Asan Medical Center from Jan 2008 to Dec 2009) were enrolled in the present study. A total of 93 bone marrow (BM) samples (27 at diagnosis and 56 at follow-up) were obtained retrospectively, with the median follow-up period of 15 months (range: 1-38 months). Among the 27 patients, five (18.5%) possessed FLT3 ITD mutations simultaneously at diagnosis. All patients received standard induction chemotherapy that consisted of cytarabine and daunorubicin as defined in the literature [26]. This regimen included the continuous intravenous infusion of 200 mg/m2/day cytarabine (100 mg/m2/day for patients >60 yr) on days 1-7 and 45 mg/m2/day daunorubicin on days 1-3. Morphologic complete remission (CR) was defined as the presence of <5% blasts and >20% cellularity in BM aspirates, obtained at 28 days after induction chemotherapy. Relapse was defined as the presence of >5% blasts in BM aspirates for patients who had previously achieved CR. A total of 16 (59.3%) patients achieved morphologic CR in the follow-up BM examination, whereas five (18.5%) patients experienced relapse during the follow-up periods. All relapsed patients possessed the FLT3 ITD mutation at diagnosis and showed variable results in the follow-up BM study performed at 28 days after diagnosis (two patients with persistent disease, two patients with hypocellular marrow, and one patient in morphologic CR). The study was approved by the Institutional Review Board of Asan Medical Center, and all patients provided written informed consent for the genetic analysis.
2. Quantitative analysis of NPM1-mutA burden
The quantitation of NPM1-mutA burden was performed by using the Real-Q NPM1-mutA Quantitation Kit (Biosewoom Inc., Seoul, Korea), which uses RQ-PCR (reverse transcription of extracted total RNA into cDNA and amplification of DNA by real-time PCR). Total 93 BM aspirates were obtained and the test was performed following the manufacturer's instructions. The Abelson gene (ABL) was used as a reference housekeeping gene, and the allele burden of NPM1-mutA was represented as a ratio of its copy number relative to the ABL copy number (NPM1-mutA/ABL).
3. Comparison of NPM1-mutA quantitation results with respect to the clinical condition of each patient
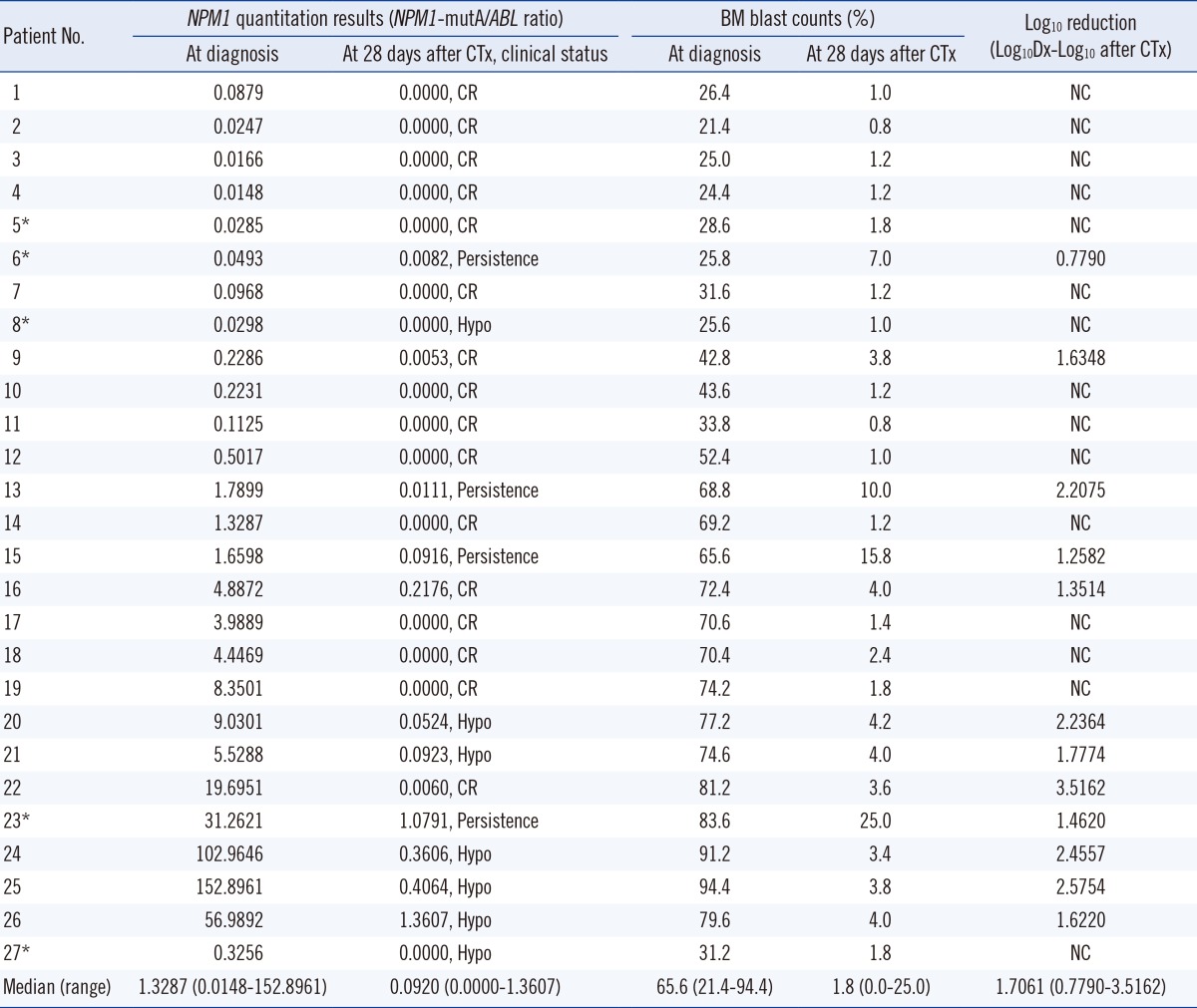
The NPM1-mutA quantitation results obtained at diagnosis and at 28 days after chemotherapy were assessed in each patient and analyzed in relation to the clinical condition of the patient. In addition, for each patient, the BM blast counts measured at diagnosis and at 28 days after chemotherapy were correlated with their NPM1-mutA quantity. These results are summarized in Table 1. For the five patients who experienced relapse during follow-up, NPM1-mutA mRNA levels at each follow-up time point before the relapse were assessed, and compared with the patient's clinical condition. These results are illustrated in Fig. 1.
4. Statistical analysis
The Spearman's correlation analysis was performed to see the correlation between the BM blast counts and NPM1-mutA quantitation results measured at diagnosis and at 28 days after chemotherapy. All tests were two-tailed, and P≤0.05 was considered significant. All analyses were performed by using SPSS 13.0.1 for Windows (SPSS Inc., Chicago, IL, USA).
RESULTS
1. Comparison of NPM1-mutA burden at diagnosis and at 28 days after chemotherapy
The median NPM1-mutA/ABL ratio was 1.3287 at diagnosis and 0.0920 at 28 days after chemotherapy. When converted to log scale, the median log10 reduction at 28 days after chemotherapy relative to that at diagnosis was 1.7061. Spearman's correlation analysis results demonstrated significant positive correlation between the BM blast counts and NPM1-mutA quantitation results measured at diagnosis (γ=0.5885, P= 0.0012) and at 28 days after chemotherapy (γ=0.5106, P= 0.0065).
Of the 27 patients, 16 showed morphologic CR, seven developed hypocellular marrow, and four showed cancer persistence in the follow-up BM examination performed at 28 days after chemotherapy. Of the patients with morphologic CR, 13 patients showed complete loss of NPM1-mutA burden, and the additional one patient showed log10 reduction values of 3.5162 at 28 days after chemotherapy. This means that 87.5% of patients achieved reduction of the NPM1-mutA/ABL ratio of >3 log10 at the morphologic CR state compared with that at diagnosis. Of the seven patients with hypocellular marrow, two patients showed complete loss of NPM1-mutA burden but the remaining five patients showed residual NPM1-mutA burden at 28 days after chemotherapy. All patients with cancer persistence showed persistent NPM1-mutA burden at 28 days after chemotherapy (Table 1).
In summary, 81.3% of patients with morphologic CR and 28.6% of patients with hypocellular marrow at 28 days after chemotherapy achieved complete loss of NPM1-mutA burden at that time. In contrast, 18.7% of patients with morphologic CR, 71.4% of patients with hypocellular marrow, and 100.0% of patients with persistence at 28 days after chemotherapy showed residual NPM1-mutA burden at that time.
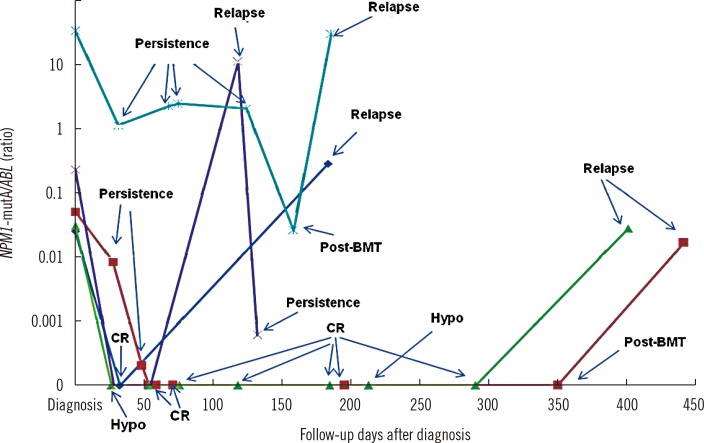
2. Correlation of NPM1-mutA burden in relapse patients with their clinical status
Of the five patients who experienced relapse at follow-up, one patient (dark blue line) had complete loss of NPM1-mutA burden at the morphologic CR state, but showed increased burden at relapse. A second patient (light blue line) showed persistent NPM1-mutA burden during the persistence state, followed by reduced burden at the post BM transplantation state, and finally prominent increase of the NPM1-mutA burden at relapse. A third patient (purple line) showed complete loss of NPM1-mutA burden at the hypocellular marrow state but recorded marked increase of the NPM1-mutA/ABL ratio at relapse. The remaining two patients (green and red lines, respectively) recorded complete loss of mutation burden at the morphologic CR, hypocellular marrow, and post BM transplantation states during follow-up, but showed an increased NPM1-mutA/ABL ratio at relapse. All five relapsed patients had simultaneous NPM1-mutA and FLT3 ITD mutations at diagnosis, but showed loss of the FLT3 ITD mutation while retaining stable NPM1-mutA at relapse.
In summary, NPM1-mutA disappeared in almost all the patients at the morphologic CR, hypocellular marrow, and post BM transplantation states during follow-up, but appeared again with high stability at relapse. This represented a median mutation burden increase of 0.91-fold (range: 0.33-46.88) over that at diagnosis (Fig. 1).
DISCUSSION
The assessment of cancer remission using specific molecular markers in AML patients has been included in the treatment response criteria, with residual disease monitoring being regarded as an important tool in the management of these patients. Previous studies showed that the NPM1 mutation burden is correlated with the clinical status of patients and can be used for the prediction of relapse risk in AML patients with the mutated NPM1 gene [67]. The advantages of NPM1 mutation as a residual disease monitoring marker lie in its high stability at relapse and its relatively high incidence in NK-AML patients [4567232425262728]. Focused on this point, in the present study, we evaluated the applicability of NPM1-mutA quantitation by RQ-PCR for assessing the clinical status and predicting the outcomes of AML patients bearing this mutation.
We found that 81.3% of patients in morphologic CR and 28.6% with hypocellular marrow at 28 days after chemotherapy had achieved complete loss of NPM1-mutA, whereas 18.7% of patients in morphologic CR, 71.4% with hypocellular marrow, and 100.0% with cancer persistence at 28 days after chemotherapy showed residual NPM1-mutA burden at that time. In addition, we identified the prediction rate of morphologic CR at 28 days after chemotherapy to be 87.5% when a >3 log10 reduction of NPM1-mutA burden was recorded at that time compared with the value at diagnosis. These results suggest that NPM1-mutA burden indeed correlates with the clinical status of patients, and a >3 log10 reduction of NPM1-mutA burden is a reliable molecular marker for predicting morphologic CR at 28 days after chemotherapy. This underscores the need for NPM1-mutA quantitation in the clinical setting for the evaluation of residual disease burden if the patient harbors this gene mutation. Subsequent analysis also demonstrated the association between a complete loss of NPM1-mutA burden and morphologic CR, hypocellular marrow, and post BM transplantation status, and the high stability of this mutation at relapse. All these results point to the main conclusions that the quantity of NPM1-mutA correlates well with the patient's status categorized as CR, relapse, or persistence, as defined by the BM blast percentage, and that the increase in NPM1-mutA burden can predict the patient outcome. This supports the high validity of adopting the NPM1-mutA quantitation assay in the clinical setting, which corresponds to previous study conclusions [672728].
In the present study, the BM blast counts and NPM1-mutA levels had significantly positive correlation (P<0.05), both at diagnosis and at 28 days after chemotherapy. These results underscore our main observation above, that the NPM1-mutA level would be correlated with the patient's clinical status as categorized by BM blast counts (CR, persistence, or relapse). However, our study also revealed a wide range of NPM1-mutA levels among the 27 patients at diagnosis, with some patients showing a high mutation burden with high BM blast count and others showing a low mutation burden. The wide range of BM blast counts detected among our patient cohort may contribute to these results, and partial expression of mutated NPM1 protein in the BM blasts may be another possible explanation for the variations.
Although 12 patients had persistent NPM1-mutA burden at 28 days after diagnosis, only five patients experienced relapse at follow-up. We speculate that a small portion of residual leukemic blasts (<5%) would survive in the morphologic CR or hypocellular marrow state, and complete loss of NPM1-mutA burden may not be achieved in these patients. We found that the eight patients who were in the morphologic CR or hypocellular marrow state, but did not achieve complete loss of NPM1-mutA burden, possessed relatively higher BM blast counts at 28 days after diagnosis (3.4-4.2%) than the 14 patients who achieved complete loss of the gene mutation (0.8-2.4%), supporting our speculation above.
Besides monitoring of the residual disease burden, clarification of the association between the degree of reduction of NPM1-mutA burden and the clinical improvement of patients would provide important information to clinicians. Although our study found a relatively smaller log10 reduction of NPM1-mutA burden (range: 0.7790-2.2075) in patients with cancer persistence at 28 days after chemotherapy than in patients with morphologic CR (complete loss in 81.3% of patients, and 1.6348, 1.3514, and 3.5162 log10 reductions in the remaining three patients) and hypocellular marrow (complete loss in 28.6% of patients, and 2.2364, 1.7774, 2.4557, 2.5754, and 1.6220 log10 reductions in the remaining five patients), the statistical significance of the results could not be determined owing to the small patient cohort, and so our study could not evaluate this issue accurately. This would be the major limitation of this study and should be assessed in a future comprehensive study.
In conclusion, we demonstrated that the NPM1-mutA burden in NK-AML patients correlates well with their cancer status, with high stability at relapse, and could predict their outcomes. This emphasizes the need for including the NPM1-mutA quantitation assay in the treatment program of AML patients harboring this gene mutation.
 XML Download
XML Download