

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
More than 100 human papillomavirus (HPV) genotypes have been reported [1]. Previous studies on the epidemiologic classification of HPV associated with cervical cancer found that HPV can be grouped into high-risk (HR), probable high-risk (PHR), and low-risk (LR) HPV genotypic groups according to their carcinogenic potential [2]. Recently, the International Agency for Research on Cancer (IARC) defined the HPV16 type, which is known to cause cancer at several sites, as the most potent carcinogenic HPV type [3]. HPV types 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, and 59 were classified as Group 1, which indicates that there is sufficient evidence that these strains cause cervical cancer.
Numerous commercially-available or laboratory-developed HPV typing methods have been introduced to date. These tests have been based on different methods, including DNA-RNA hybrid capture, real-time PCR-based assays, microarray-based assays, suspension array-based assays, and direct sequencing [4, 5]. Several array-based techniques have also been developed, which consist of type-specific oligonucleotide or PCR amplicon probes immobilized on solid surfaces, such as glass, membranes, or liquid beads. These techniques are useful for HPV genotyping, because they allow for rapid and simultaneous identification of various viruses or of the same virus with different genotypes in a single assay [6]. However, array-based techniques are difficult to standardize owing to their large number of probes, and exhibit low reproducibility because of non-specific hybridization reactions [7].
Since their introduction, several studies comparing the performance of these array-based techniques with that of other more well-established HPV detection methods have been conducted [8, 9, 10]. However, few studies have compared the different multiplex array-based techniques using clinical samples [11].
Among the commercially available array-based methods, the digene HPV Genotyping LQ Test (LQ; QIAGEN, Hilden, Germany) uses multiplex, liquid bead-based xMAP suspension array technology to identify 18 HR HPV types [9]. The PANArray HPV Genotyping Chip (PANArray; PANAGENE, Daejeon, Korea) is a peptide nucleic acid (PNA)-based array and uses the DNA chip technology. This technique uses a microarray platform with PNA probes, which have better chemical and enzymatic stability than DNA oligonucleotide probes [12].
The present study aimed to evaluate the performance of two different array-based techniques-the bead-based multiplex genotyping method (LQ) and the DNA chip technology using PNA probes (PANArray)-for HPV detection and genotyping of HR or PHR HPV in Korean women seeking routine screening for cervical cancer.
METHODS
1. Clinical specimens
This was a prospective study conducted in a routine diagnostic laboratory setting at the Samsung Medical Center, Seoul, Korea; the study protocol was approved by the Institutional Review Board (IRB) of Samsung Medical Center (IRB No. 2011-02-045). Five hundred and eight, unselected, consecutive cervicovaginal swab specimens were obtained from women visiting a health-promotion center by using a cytobrush.
The mean age of the 508 patients was 52 yr (range, 27 to 82 yr). The cytologic diagnoses were: 495 (97.4%) normal, 5 (1.0%) atypical squamous cells of undetermined significance (ASCUS), and 8 (1.6%) low-grade squamous intraepithelial lesions (LSIL). There were no patients with high-grade squamous intraepithelial lesions (HSIL).
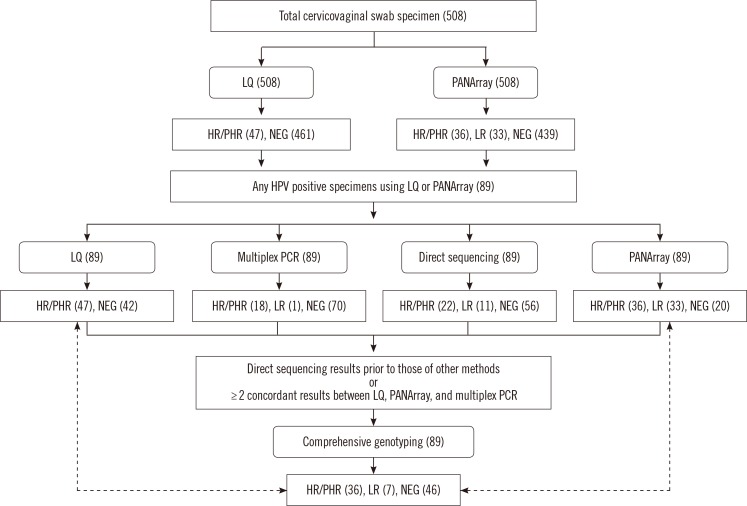
All specimens were tested for HPV, as well as carrying out HPV genotyping, using both PANArray and LQ tests. The HPV-positive samples thus identified were additionally analyzed by multiplex PCR and direct sequencing (Fig. 1).
2. Digene HPV genotyping LQ test
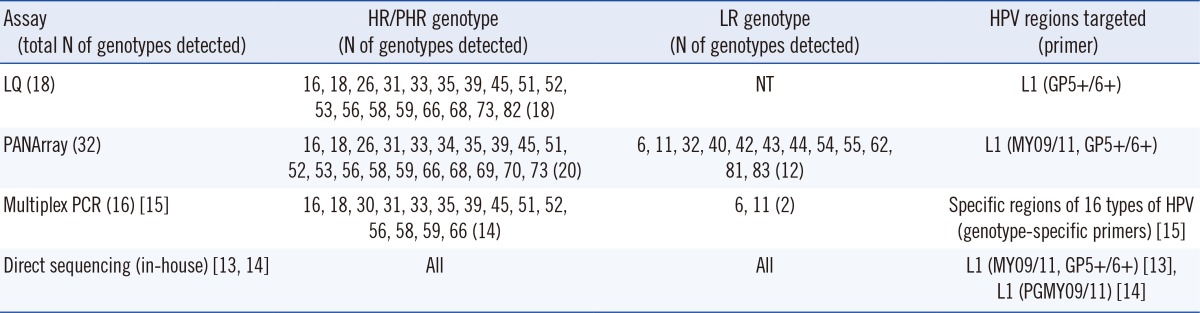
DNA was extracted by using a QIAmp minElute Virus Spin Kit (Qiagen) and a 100 µL was eluted from 200 µL of the sample. The LQ test utilizes probes for 18 HR or PHR HPV genotypes (Table 1), as identified in previous reports on the classification of HPV types associated with cervical cancer [2, 3]. The probes for HPV detection were immobilized on color-coded microbeads and a single color per HPV genotype was detected. The LQ test was performed by using the Luminex 100 IS system (Luminex Corporation, Austin, TX, USA) according to the manufacturer's instructions. A positivity threshold of 100 median fluorescence intensity (MFI) was applied.
3. PANArray HPV genotyping chip
DNA was extracted according to the manufacturer's instructions by using a heating method, in which 1 mL of a liquid-based preparation of a cervical specimen was transferred to phosphate-buffered saline (PBS). This mixture was centrifuged, and then 20 µL of DNA extraction buffer was added. The sample was subsequently heated at 55℃ for 1 hr and at 110℃ for 28 min. After further centrifugation at 12,000 rpm for 5 min, 90 µL of the supernatant was used as the source of DNA for PCR analysis. The PANArray can detect 20 HR or PHR HPV genotypes and 12 LR genotypes (Table 1).
5. Comprehensive genotyping
Comprehensive HPV genotyping was based primarily on the results of direct sequencing. In addition, two or more concordant results between LQ, PANArray, and multiplex PCR tests in the absence of a direct sequencing result were considered part of the comprehensive HPV genotyping (Fig. 1).
6. Statistical analysis
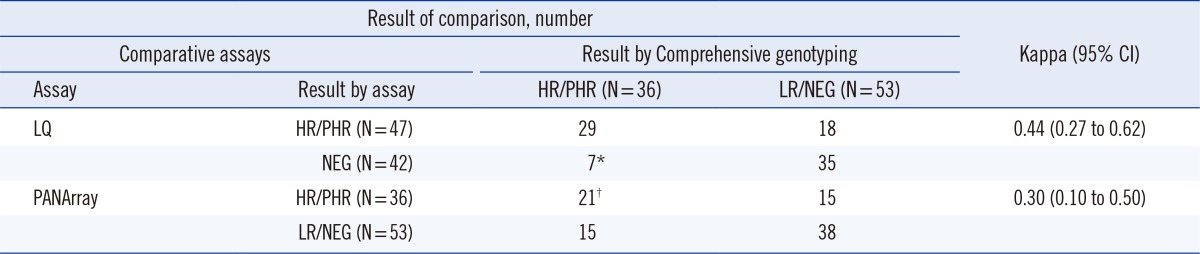
Statistical analyses were performed using SPSS 20.0 (SPSS Inc., Chicago, IL, USA) and MedCalc software (MedCalc software, Mariakerke, Belgium). We calculated kappa inter-rater agreement values with 95% confidence intervals (CI) to compare the detection of HR or PHR HPV genotypes between the LQ and PANArray test results using the comprehensive genotyping results as the reference value. Kappa values are interpreted as follows: 0-0.20 as slight, 0.21-0.40 as fair, 0.41-0.60 as moderate, 0.61-0.80 as substantial, and 0.81-1 as almost perfect agreement.
RESULTS
Among the 508 specimens, the LQ test detected 47 (9.3%) HPV cases with HR or PHR genotypes, and the PANArray test identified 36 cases (7.1%) with HR or PHR genotypes and 33 cases (6.5%) with LR genotypes (Fig. 1). There were 89 HPV-positive specimens identified by LQ and/or PANArray testing, and these were analyzed further by multiplex PCR and direct sequencing. The detection rates of HR or PHR genotypes were 52.8% (47/89) by the LQ test, 40.4% (36/89) by the PANArray test, 20.2% (18/89) by multiplex PCR, and 24.7% (22/89) by direct sequencing. Thirty-six cases (40.4%) were determined to be HR or PHR genotypes using comprehensive genotyping based on integrated interpretation of the results of all 4 assays. Because the LQ test can detect only 18 HR or PHR genotypes (Table 1), we assigned the results to 2 groups: HR or PHR and LR or HPV-negative to facilitate direct comparison of the results of LQ and PANArray, LQ and comprehensive genotyping, and PANArray and comprehensive genotyping. For all specimens, the results of the LQ and PANArray showed 90.6% agreement with a kappa value of 0.36 (95% CI, 0.22-0.51).
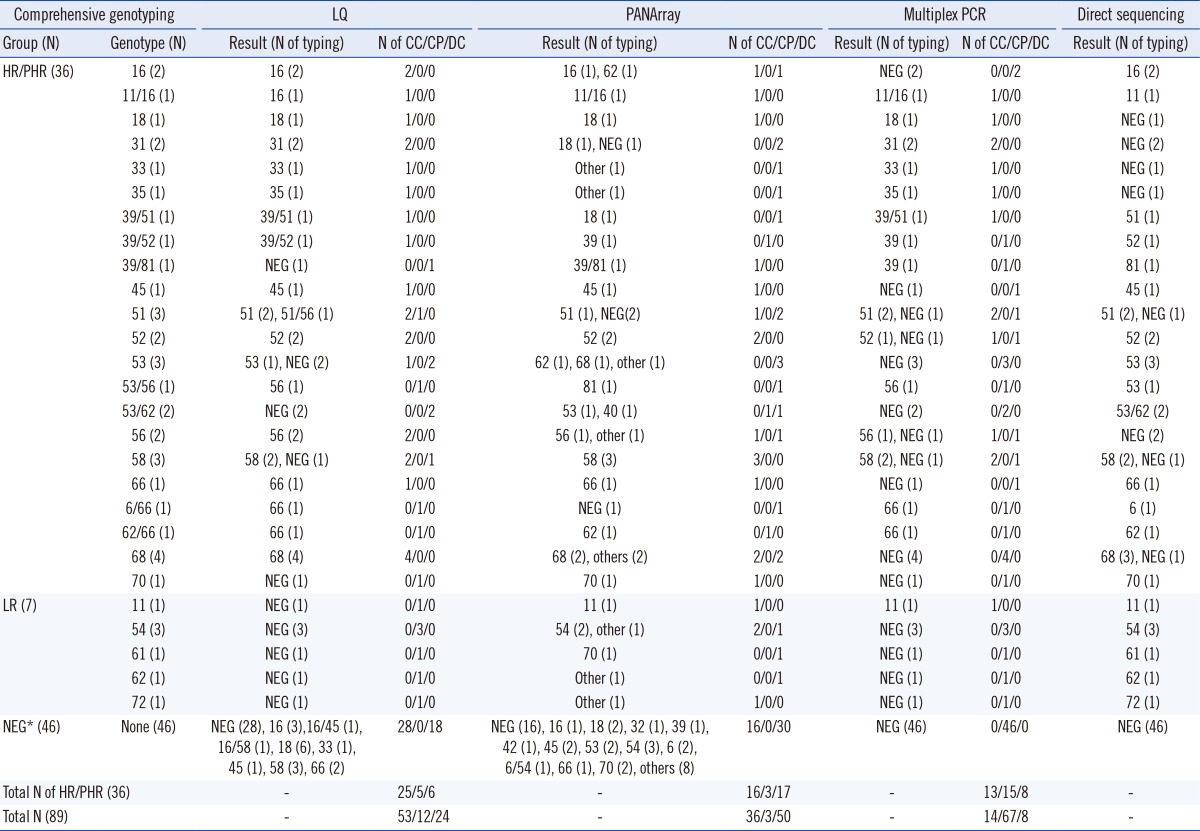
Of the 89 HPV-positive specimens identified using either the LQ or PANArray, the kappa values were 0.44 (95% CI, 0.27-0.62) for LQ and 0.30 (95% CI, 0.10-0.50) for PANArray with respective to that of comprehensive genotyping for the detection of HR or PHR genotypes (Table 2). LQ yielded 53 (60.0%) results concordant with and 12 (13.5%) results compatible with those obtained with comprehensive genotyping, whereas the PANArray yielded 36 (40.4%) concordant and 3 (3.4%) compatible results (Table 3). Multiple infections with different HPV genotypes were detected in 9 cases by comprehensive genotyping. Only direct sequencing could detect multiple infections in the 2 cases. The remaining 7 cases were determined by comprehensive analysis of the results of 4 assays (Table 3).
DISCUSSION
In the present study, we compared the performance of 2 array-based techniques for HPV genotyping using clinical samples from visitors to a health promotion center. We used multiplex PCR and direct sequencing, in addition to comprehensive genotyping (integrated interpretation of the results of LQ, PANArray, multiplex PCR, and direct sequencing) as reference methods.
Recent studies have evaluated the performance of the digene LQ test in comparison with those of other established HPV genotyping methods [8, 9, 16]. In these studies, the LQ test showed high concordance with the reference methods with respect to HR HPV detection, with kappa values of 0.884 between LQ and the reverse line blot assay [16], 0.923 between LQ and the Amplicor HPV test (Roche Molecular Diagnostics, Pleasanton, CA, USA) [9], and 0.94 between LQ and the Hybrid Capture 2 test (HC2; Qiagen, Gaithersburg, MD, USA) [8].
Studies evaluating DNA chip-based methods for detection of HR HPV genotypes also reported high concordance with the results of reference methods for HR HPV detection, with kappa values of 0.80 [11], 0.61 [17], and 0.80 [18] between the DNA chip results and those of direct sequencing.
However, in the current study, although comprehensive genotyping was used as a reference method in addition to direct sequencing, the concordance between the results of the 2 array-based techniques and comprehensive genotyping for HR HPV detection was relatively low, with kappa values of 0.44 between LQ and comprehensive genotyping and 0.30 between PANArray and comprehensive genotyping.
The results of the present study differ from those of prior studies for several reasons. We used a prospective, unselected study design and used clinical specimens from healthy visitors to a health promotion center, rather than specimens from visitors presented to a gynecology clinic for cervical cancer screening. Many prior studies comparing HPV genotyping assays used selective positive samples as determined by other assays such as HC2 or PCR [8, 16, 19] or clinical samples with abnormal cytology [17, 18]. Therefore, a relatively high proportion of samples with HSIL were included in these studies. However, when HPV genotyping assays are used for HR HPV detection and HPV genotyping in a routine diagnostic laboratory, HSIL specimens are not likely to be encountered.
According to the previous studies [20, 21], although the HPV DNA viral load does not correlate with histomorphological findings (normal; cervical intraepithelial neoplasia grades CIN1, CIN2, or CIN3; and cervical squamous cell carcinoma), statistically significant differences were present between all grades of CIN and the group lacking CIN [20]. In addition, the association of viral load with lesion grade may change depending on HPV genotype [21]. In the present study, the cytologic findings of nearly all enrolled cases were normal (97.4%), which implies that if these individuals had HPV, they might have a lower HPV DNA viral load than did patients included in the previous studies.
We observed several cases where HR HPV was detected by 2 or more tests among LQ, PANArray, and multiplex PCR, but not by direct sequencing, and vice versa. We surmise that the low HPV DNA viral load in our samples may have affected the results of these assays. The different assays may also differ in diagnostic sensitivity across HPV genotypes. Considering this potential limitation, we used comprehensive genotyping as the reference method. Therefore, the detection rate of HR or PHR genotypes using comprehensive genotyping was higher than that of direct sequencing (24.7% [22/87] vs. 40.4% [36/87]).
Direct sequencing results were given priority to determine the comprehensive HPV genotype, but we also considered concordant positive results from the other assays. Although direct sequencing is the gold standard for viral typing, it has limitations with regards to detecting multiple HPV genotypes [22]. Similar observations were made in the present study, where comprehensive genotyping detected 7 additional cases with multiple infections relative to those detected by direct sequencing. If subjects had multiple HPV genotypes, with each HPV genotype being present at a low DNA concentration, direct sequencing alone might not be sufficient for accurate detection.
The present study had some limitations. We could not compare a large number of HPV genotypes between assays because of the low number of HR HPV-positive specimens. In particular, the numbers of HPV 16- and HPV 18-positive samples were low, which are the most potent HPV types for inducing cervical cancer. Furthermore, to understand the reason behind the difference between the assay results, a comparative analysis of the detection limits for each HPV type should be conducted.
In conclusion, for the detection of HR or PHR genotypes, the results of the LQ assay had higher concordance or compatibility with those of comprehensive genotyping than those of PANArray assay.
 XML Download
XML Download