

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Mean platelet volume (MPV), which reflects the size of platelets, is an accepted marker of platelet function [1]. Measuring MPV is inexpensive and can be included in routine blood tests. On comparison of the two platelet types, larger platelets have more granules, aggregate more rapidly with collagen, have a higher thromboxane A2 level, and express more glycoprotein Ib and IIb/IIIa receptors than smaller platelets [2]; however, both secrete substances that are important mediators of coagulation, inflammation, thrombosis, and atherosclerosis. Therefore, platelets can increase the incidence of occlusive vascular disease [3, 4]. Studies have shown that MPV levels are associated with both arterial and venous diseases, such as coronary artery disease [5], diabetes [6], stroke [7], hypertension [8], and venous thromboembolism [9].
The main function of vitamin D is calcium metabolism and bone structure. Vitamin D deficiency is a major health problem that affects all age groups, and is associated with rickets in children and osteoporosis in adults. In adults, the deficiency may contribute to the etiology of hypertension and other adverse cardiovascular effects [10], cancer [11], and impaired cognitive function [12]. Vitamin D supplementation improves cognitive function [13] and decreases cardiovascular disease incidence [14]. Vitamin D deficiency can also lead to immunological diseases and inflammation. Vitamin D has many different functions in humans; for example, it acts as an immunomodulatory factor [15]. In addition, the levels of proinflammatory cytokines such as tumor necrosis factor alpha (TNF-α) and interleukin (IL)-6 are increased in vitamin D deficiency [16]. While vitamin D supplementation restores immune function and decreases cytokines levels [17], elevated cytokine levels lead to increased MPV [4, 18]. However, vitamin D decreases the expression of the various adhesion molecules, thus preventing platelet activation and decreasing fibrinolysis and thrombosis [19]. In patients with vitamin D deficiency, the combined effect of elevated TNF-α and IL-6 levels and increased release of adhesion molecules may lead to an increased MPV. Therefore, we aimed to investigate whether vitamin D deficiency is associated with high MPV.
METHODS
1. Patients
This study was an observational cross-sectional study carried out at the Internal Medicine Department of Faculty of Medicine of Recep Tayyip Erdogan University from March in 2012 to May in 2013. A total of 438 patients (288 women and 150 men) were included in the patient groups who visited our internal medicine clinic with simple complaints such as headache, low back pain, and simple abdominal pain, etc., without concomitant diseases. They were nonsmokers, not taking calcium or vitamin D supplements, not consuming alcohol or using drugs. The study excluded patients with a history of diabetes, hypertension, hyperlipidemia, coronary artery disease, chronic obstructive pulmonary disease, vitamin D deficiency, and calcium metabolic disorders, etc. All blood samples were collected in the spring season. The literature states that patients with vitamin D levels <10 ng/mL have vitamin D deficiency that is associated with a very high cardiac risk and those with vitamin D levels <20 ng/mL have vitamin D insufficiency associated with just an increased cardiac risk [20]. Thus, we divided patients into three groups as follows: Group 1, vitamin D level of <10 ng/mL (n=138; 46 men and 92 women); Group 2, vitamin D level of 10-20 ng/mL (n=148; 54 men and 94 women); and Group 3, vitamin D level of >20 ng/mL (n=148; 50 men and 98 women).
2. Laboratory tests
Biochemical parameters were measured after a 12-hr fast. Biochemical tests that measured fasting plasma glucose (FPG), AST, ALT, blood urea nitrogen (BUN), and creatinine were performed by using photometric assays on the Architect c16000 analyzer (Abbott Diagnostics, Abbott Park, IL, USA). Hematologic tests that measured Hb, platelets, white blood cells (WBC), and MPV were performed by using the Cell-Dyn Ruby analyzer (Abbott Diagnostics). Serum levels of vitamin D (25-hydroxyvitamin D) were measured by chemiluminescent microparticle immunoassay on the Architect-I 2000 system (Abbott Diagnostics).
3. Ethics
The study conformed to the principles outlined in the Declaration of Helsinki and was approved by the local ethics committee of Recep Tayyip Erdogan University, School of Medicine, Rize, Turkey.
4. Statistical analyses
Among patients with a vitamin D level >20 ng/mL, the mean vitamin D level was <30 ng/mL. The MPV and other laboratory test results were evaluated separately for all three groups. In addition, statistical analyses were repeated for all patients with a vitamin D level of <20 ng/mL and >20 ng/mL so that we could investigate the association between a vitamin D level of <20 ng/mL and a high MPV.
Results are reported as the mean±SD. All data were analyzed using the statistical software SPSS for Windows (version 13.1, SPSS, Chicago, IL, USA). All continuous variables were checked with Kolmogorov-Smirnov normality test to show their distributions. The continuous variables in all groups showed a normal distribution. The differences in all parameters between the three groups were analyzed using two by two tables and performing a t-test for independent samples. Subgroup analyses for gender were performed using nested ANOVA followed by the Bonferroni analysis. Linear regression analysis was performed to determine the presence of an independent relationship between the MPV and the vitamin D level with other potential confounding variables. The relationship between these variables was analyzed using Pearson's correlation. Differences were considered significant at P<0.05.
RESULTS
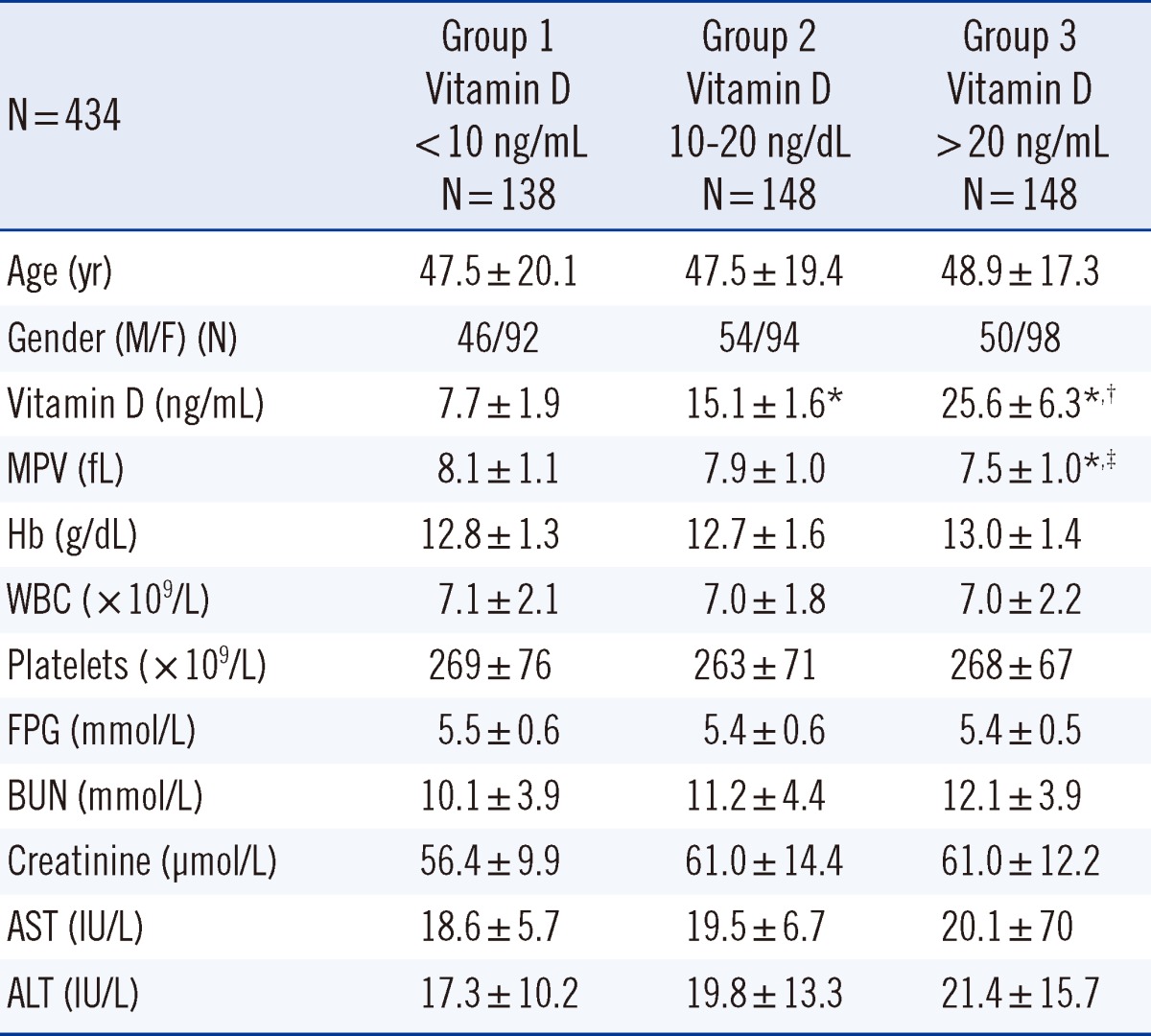
Patients' demographic characteristics and laboratory values are shown in Table 1. The mean age in Group 1, 2, and 3 was 47.5±20.1 (range, 18-87) yr, 47.5±19.4 (range, 17-93) yr, and 48.9±17.3 (range, 18-83) yr, respectively. Vitamin D level in Group 1 (7.7±1.9 ng/mL) was significantly lower than that in Group 2 (15.1±1.6 ng/mL, P<0.001) and Group 3 (25.6±6.3 ng/mL, P<0.001). The MPV in Group 3 (7.5±1.0 fL) was significantly lower than that in Group 1 (8.1±1.1 fL, P<0.001) and Group 2 (7.9±1.0 fL, P=0.009). The Hb level, WBC count, and platelet level of Groups 1, 2, and 3 were similar (Table 1).
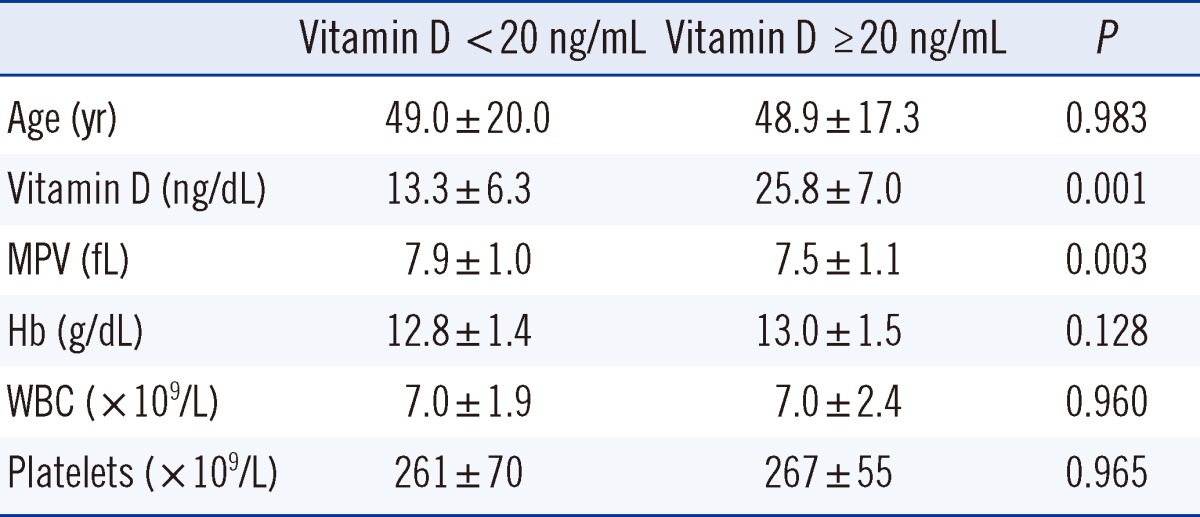
Patients were divided into two groups according to a vitamin D level of <20 ng/mL or >20 ng/mL (Table 2). The MPV in patients with a vitamin D level of <20 ng/mL was significantly higher than that in patients with a vitamin D level of >20 ng/mL (7.9±1.0 fL vs. 7.5±1.1 fL, P=0.003).
Vitamin D level and MPV were evaluated after stratifying patients according to gender, for each group in Table 3. Vitamin D levels for both male and female patients in Group 1 was lower than those in Groups 2 and 3 (P<0.001 for all). In addition, vitamin D levels for both male and female patients in Group 2 were lower than those in Group 3 (P<0.001). For MPV, female patients in Group 1 (8.0±1.0 fL) had significantly higher MPV than both male and female patients in Group 3 (men, 7.4±1.0 fL; women, 7.6±1.0 fL, P<0.001 for all).
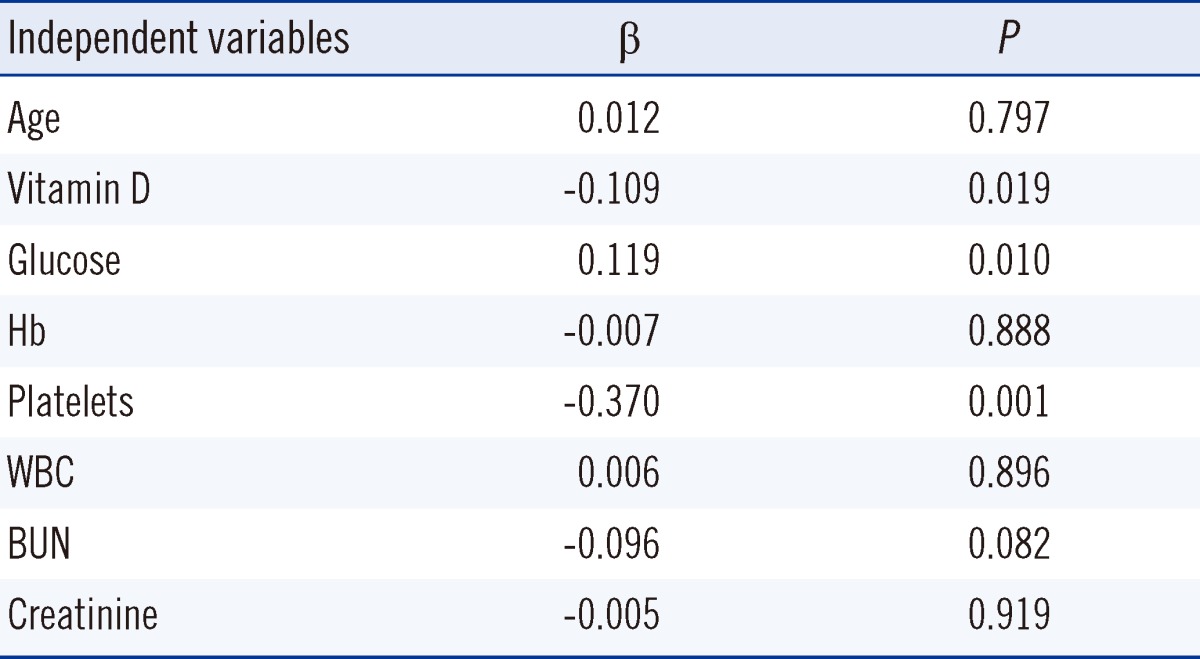
MPV and age were dependent variables and the vitamin D level and other hematologic and laboratory parameters were independent variables in the linear regression analysis. Low vitamin D (β=-0.109, P=0.019) and FPG (β=0.119, P=0.010) were independently associated with a high MPV (Table 4). In the Pearson's correlation analysis, a negative correlation was found between the vitamin D level and MPV (r2=0.020, P=0.003).
DISCUSSION
In this study, patients were divided into three groups according to the vitamin D level. The MPV in Group 3 was substantially lower than that in Groups 1 and 2. Although the MPV in Group 1 was higher than that in Group 2, the difference was not statistically significant. When comparing patients according to vitamin D levels of <20 ng/mL or >20 ng/mL, the MPV was substantially higher among those with a vitamin D level of <20 ng/mL. A markedly high MPV in patients with vitamin D level of <20 ng/mL indicates an increased cardiac risk. When patients were divided into subgroups according to the vitamin D level and gender, the MPVs in both the male and female patients in Groups 1 and 2 were higher than those in both the male and female patients in Group 3, and female patients in Group 1 had higher MPVs than both the male and female patients in Group 3. Vitamin D deficiency was more frequent in women than in men [21]. Male gender is a risk factor for coronary artery disease, while female gender is associated with a lower incidence of coronary artery disease [22]. This study suggests that vitamin D deficiency may be associated with an increased risk of cardiac disease in women with a high MPV, since high MPV is associated with an increased risk of coronary artery disease [5].
Vitamin D insufficiency is very common worldwide and in Turkey [23]. In particular, vitamin D deficiency is common in the Eastern Black Sea region of Turkey (41.2°N) [23, 24]. An established relationship between vitamin D deficiency and cardiac disease exists, and some mechanisms underlying the development of cardiac disease have been proposed [25]. For example, a vitamin D level of <20 ng/mL increases the risk of certain cardiac diseases, such as ischemic heart disease, sudden cardiac death, and heart failure [26]. Some studies have reported an increased risk of heart disease, when the vitamin D level is <10 ng/mL [27]. Another study reported that the prevalence of hypertension increased with a vitamin D level of <15 ng/mL [28]. Moreover, calcium plus vitamin D supplementation is thought to reduce systolic and diastolic hypertension [29].
Hypertension and increased cardiac risk due to vitamin D deficiency may be associated with the direct effects of calcium deposition in vascular smooth muscle that may in turn lead to renin-angiotensin system activation, impaired glycemic control, hyperuricemia, and increased levels of inflammatory cytokines [30, 31]. One experimental study showed that vitamin D receptor (VDR) knockout mice had increased blood pressure, cardiac hypertrophy, and elevated activation of the renin-angiotensin-aldosterone system [32]. These mice demonstrated impaired cardiac relaxation and contractility as well as developed left ventricular hypertrophy [32]. Several small observational and case-control studies have suggested that vitamin D deficiency is associated with insulin resistance or impaired insulin secretion, while insulin resistance and hyperglycemia are associated with hypertension and coronary heart disease [33, 34]. A previous study also showed that vitamin D supplementation given to patients with heart failure decreases symptoms that may be related to decreased levels of inflammatory cytokines [35].
In previous investigations on potential adverse effects of vitamin D deficiency on the heart, MPV (known to cause cardiac events such as myocardial infarction and acute coronary syndrome) has not been considered in the analyses. The balance of body cytokines changes with decreased levels of vitamin D, and the release of cytokines increases TNF-α and IL-6 levels [15, 16]. The increased release of cytokines in patients with vitamin D deficiency may be associated with the VDR, a transcription factor that mediates the genomic effects of calcitriol. The VDR is constitutively expressed in monocytes and macrophages. Thus, the release of cytokines such as IL-6 and TNF-α may be affected. Previous studies have reported decreases in IL-6 and TNF-α after vitamin D treatment [36]. TNF-α and IL-6 are related to oxidative stress and stimulate megakaryopoiesis [18]. These cytokines are associated with enhanced oxidative stress that contributes to platelet activation. The induction of this event leads to the release of immature and activated platelets from bone marrow to the circulatory system, thus increasing MPV. Previous studies have shown that vitamin D decreases the expression of vascular cell adhesion molecule (VCAM)-1 and membrane type-1 matrix metalloproteinase (MT1-MMP), therefore preventing platelet activation and decreasing fibrinolysis and thrombosis [19].
We observed that a low vitamin D level was correlated with a high MPV. Vitamin D deficiency increases the release of proinflammatory cytokines such as IL-6 and TNF-α [16] that may lead to a high MPV. Consequently, a high MPV increases cardiac disease risk. One previously reported mechanism suggests that vitamin D exerts anticoagulant effects by upregulating the expression of an anticoagulant glycoprotein (thrombomodulin) and downregulating the expression of a critical coagulation factor (tissue factor) in monocytes [37]. Therefore, vitamin D derivatives may be developed as new types of antithrombotic agents. A study conducted by Kebapcilar et al. [38] on women diagnosed with primary ovarian insufficiency showed a negative correlation between MPV and the vitamin D level, and Koyama et al. [37] found similar results. The results of our study also coincide with these studies.
This study showed that FPG was strongly associated with an increased MPV. High FPG or hyperinsulinemia may cause an increased MPV. Hyperglycemia can increase platelet reactivity by inducing nonenzymatic glycation of proteins on the surface of the platelets [39]. Additionally, platelet function is directly regulated by insulin via the functional insulin receptor (IR) found on human platelets [39]. Vitamin D plays an important role in insulin secretion, and vitamin D deficiency is associated with glucose intolerance and insulin sensitivity and type 2 diabetes [40]. Nonetheless, vitamin D deficiency can lead to the destruction of pancreatic β-cells via increasing IL-6 and TNF-α levels [17]. Thus, increased levels of cytokines such as IL-6 and TNF-α may lead to hyperglycemia and hyperinsulinemia in patients with vitamin D deficiency. This could explain why the patients in this study had high MPV. Therefore, low vitamin D level may deteriorate the balance between anticoagulant glycoprotein and coagulation factors in favor of coagulation. This event may stimulate the release of platelets and lead to the emergence of large, young platelets into the peripheral circulation.
This study has several limitations. First, the number of enrolled patients was inadequate to reflect the general population. Second, the presence of cardiac disease was not analyzed when comparing MPV with vitamin D deficiency. This should be investigated in future studies. Last, vitamin D supplementation in vitamin D-deficient individuals may decrease MPV; however, it was not analyzed in our study. Further studies are needed to validate our findings.
Vitamin D deficiency is related to an increased incidence of hypertension and cardiac events and increases the release of proinflammatory cytokines such as TNF-α and IL-6. Moreover, vitamin D deficiency may increase hyperglycemia and hyperinsulinemia that may deteriorate the anticoagulant glycoprotein and coagulation factor balance, thereby leading to an increase in MPV. This study suggests that vitamin D deficiency may increase MPV.

 XML Download
XML Download