

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The current treatment strategies for B-cell ALL (B-ALL) are based on several factors, including patient-related parameters as well as intrinsic characteristics of particular disease subtypes. Abnormalities with the most significant effects on the management of B-ALL are t(12;21)(p13;q22)/ETV6-RUNX1 and high hyperdiploidy for good risk management, and t(9;22)(q34;q11)/BCR-ABL1, t(4;11)(q21;q23)/MLL-AFF1, and near-haploidy/low hypodiploidy for high-risk stratification. However, a substantial proportion of childhood leukemias remain genetically undefined or the correlation of genetic abnormalities with clinical outcome is not fully understood [1]. The detection of chromosomal abnormalities by conventional cytogenetic analysis is an essential approach for the diagnosis, and its utility has been expanded by the development of FISH [2]. The use of FISH has enabled the identification of a number of alterations in patients with failed cytogenetic results and has led to the detection of cryptic abnormalities that cannot be determined [3].
Intrachromosomal amplification of chromosome 21 (iAMP21), discovered during routine screening for the presence of the ETV6-RUNX1 fusion by FISH analysis [3], is usually defined as three or more additional copies of RUNX1 signals on a single abnormal chromosome 21 (a total of five or more RUNX1 signals per cell) [4]. This chromosomal abnormality is found in 1.5-2% of ALL cases [5] and is characterized by a low white blood cell count and a pre-B/common immunophenotype in children and adolescent populations [2]. A significant finding was that patients with iAMP21 had an inferior outcome when treated with standard therapy and an improved outcome on intensive therapy [67]. Therefore, an accurate detection of this abnormality is very important for the choice of treatment.
The morphology of the abnormal chromosome 21 is highly variable among cases and a variety of cytogenetic nomenclatures such as add(21), dup(21), and der(21) were used to describe the iAMP21 abnormalities, with the loss of chromosome 21 and an associated gain of a marker chromosome being the most common [8]. Furthermore, in cases where metaphase chromosomes are absent, other methods should be applied to distinguish iAMP21 from high hyperdiploidy with extra copies of chromosome 21. These include a subtelomeric FISH probe for chromosome 21 to demonstrate that the number of RUNX1 signals is greater than the number of chromosomes 21 [4], array comparative genomic hybridization, single nucleotide polymorphism array, and multiplex ligation-dependent probe amplification (MLPA) [9].
Because little data are available on the frequency and clinical characteristics of iAMP21 in Korean pediatric B-ALL patients, we comprehensively analyzed FISH data and further performed MLPA analysis to confirm suspected and equivocal cases.
Go to : 
METHODS
1. Patient selection and FISH analysis
A total of 102 pediatric patients diagnosed with B-ALL between February 2009 and June 2015 were retrospectively investigated in this study. Of the 102 pediatric B-ALL patients, 65 were men (63.7%) and 37 were women (36.3%), and the median age at diagnosis was 5 yr (range, 0 to 19 yr) (Table 1). Written informed consent was obtained from the patients or patients' parents for genetic analysis.
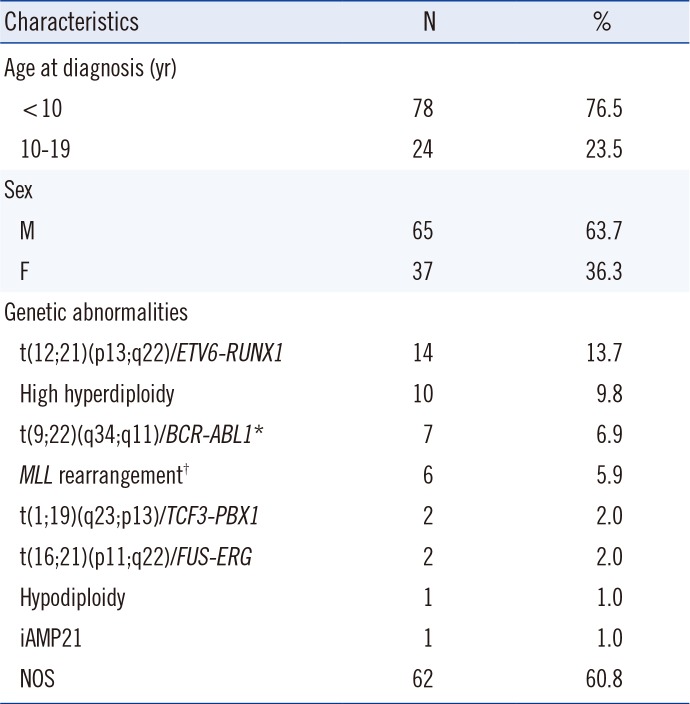
Table 1
Patient characteristics
*Five patients with e1a2, one with b2a2, and one with b3a2 fusion transcripts were included; †Three patients with t(4;11)(q21;q23)/MLL-AFF1, two with t(11;19)(q23;p13.3)/MLL-MLLT1, and one with t(1;11)(p32;q23)/MLL-EPS15 were included.
Abbreviations: M, male; F, female; iAMP21, intrachromosomal amplification of chromosome 21; NOS, not otherwise specified.
![]()
The chromosomal abnormalities were comprehensively analyzed on the basis of G-banding karyotype, FISH, and multiplex reverse transcription-PCR (RT-PCR). The screening of iAMP21 was performed by using FISH probe, ETV6-RUNX1 (TEL-AML1) dual color extra signal probe (Abbott Molecular, Abbott Park, IL, USA). For interphase FISH analysis, the slides were subjected to hybridization according to the manufacturer's instructions. The slides were counterstained with 4,6-diamidino-2-phenylindole. The slides were viewed at a magnification of 400×, and the number of interphase cells with five or more RUNX1 signals was counted; a total of 300 cells were counted for each sample.
2. Detection of recurrent translocations
Total RNA was extracted from EDTA-anticoagulated blood samples by using the QIAamp RNA Blood Mini kit (Qiagen, Hilden, Germany). cDNA was synthesized by using the Transcriptor First Strand cDNA Synthesis kit (Roche Diagnostics Corp., Indianapolis, IN, USA). To determine recurrent translocations, RT-PCR was performed by using the HemaVision kit (DNA Technology, Aarhus, Denmark) according to the manufacturer's instructions. Recurrent genetic abnormalities were detected in 40 (39.2%) patients, including ETV6-RUNX1 (14 patients, 13.7%), high hyperdiploidy (10 patients, 9.8%), BCR-ABL1 (7 patients, 6.9%), MLL rearrangement (6 patients, 5.9%), TCF3-PBX1 (2 patients, 2.0%), FUS-ERG (2 patients, 1.2%), and hypodiploidy (1 patient, 1.0%) in the order of decreasing frequency.
3. DNA extraction and MLPA analysis
DNA was extracted from bone marrow samples of patients and controls by using the QIAamp DNA Blood Mini kit (Qiagen) according to standard procedures. The presence of iAMP21 was retrospectively evaluated in three patients by using SALSA MLPA P327-B1 iAMP21-ERG probemix (MRC Holland, Amsterdam, The Netherlands), including 46 probes encompassing a region around 21q11.2 to 21q22.3, according to the manufacturer's instructions. Hybridized probes were amplified on a C1000 thermal cycler (Bio-Rad, Hercules, CA, USA). Amplicons were separated on an ABI 3730 capillary sequencer (Applied Biosystems, Foster City, CA, USA). The data were analyzed by using GeneMarker software (Softgenetics, State College, PA, USA). The relative fluorescence peak ratios were calculated from patients' peak heights divided by control's peak heights. Relative ratios between 0.75 and 1.3 were considered normal, whereas those below 0.75 and above 1.3 indicated loss or gain of genomic material.
Go to :
RESULTS
1. FISH and MLPA results
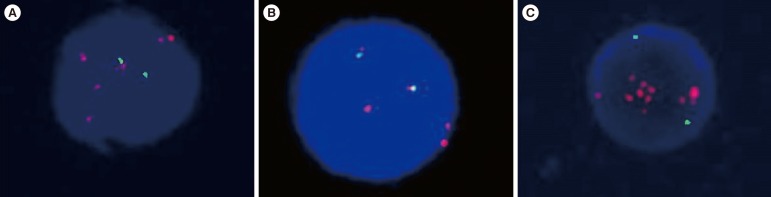
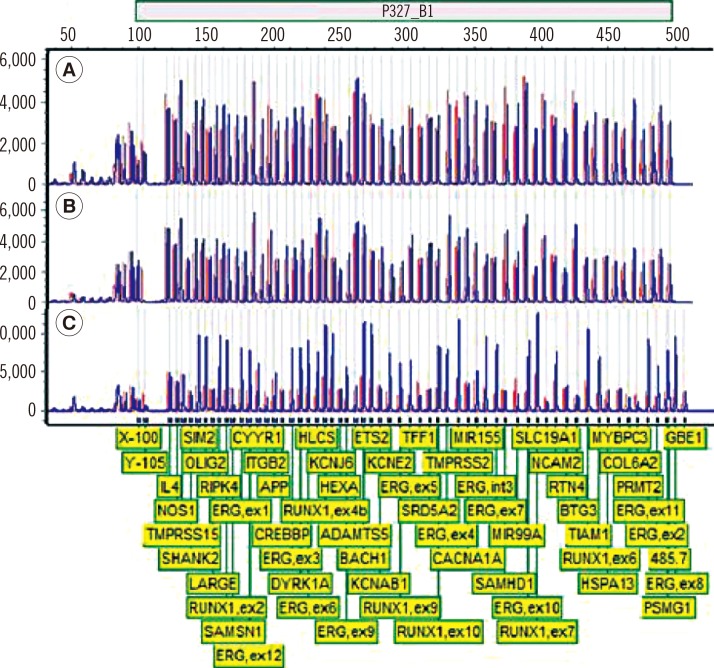
FISH screening revealed three patients with more than five RUNX1 signals (Fig. 1). The clinical characteristics of the three patients are summarized in Table 2. MLPA analysis revealed amplification of chromosome 21 in only patient C (Fig. 2). The 32 probes encompassing a 12.5-Mb region around 21q21.3 to 21q22.3, which include NCAM2, BACH1, TIAM1, OLIG2, KCNE2, RUNX1, SIM2, HLCS, DYRK1A, KCNJ6, ERG, ETS2, PSMG1, TMPRSS2, and PIPK4, showed amplification (Fig. 3). The average relative ratio of probes in amplified regions was 2.82 (range, 1.87-3.50), indicating the presence of more than five allele copies compared with the two alleles in normal controls. MIR99A on the proximal site of the amplified region and TFF1, ITGB2, SLC19A1, COL6A2, and PRMT2 on the distal site of the amplified region showed deletion signals. The average relative ratio of probes in the deleted regions was 0.62 (range, 0.53-0.72).
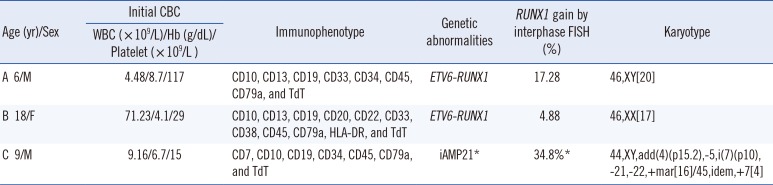
 | Fig. 1FISH analysis using ETV6-RUNX1 dual fusion probe revealed increments of the RUNX1 signal in three patients (A, B, and C). The RUNX1 signals are indicated in orange, and the ETV6 signals are indicated in green.
|
 | Fig. 2Multiplex ligation-dependent probe amplification analysis of three patients (A, B, and C). The control peaks are indicated in red, and the patients' peaks are indicated in blue; amplification of multiple probe sites on 21q21.1-21q22.3 was observed in patient C.
|
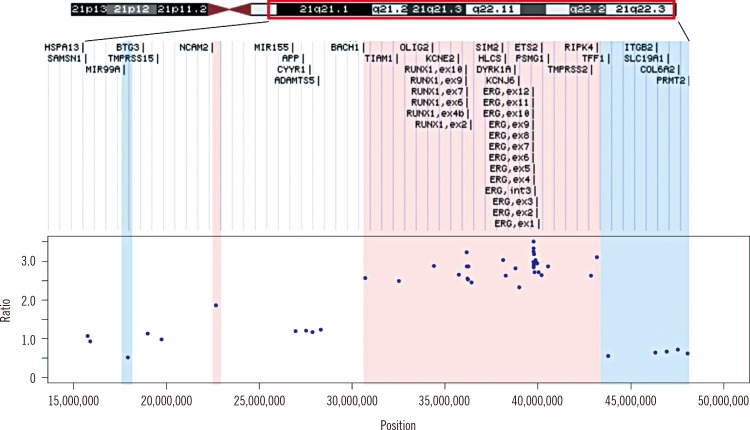 | Fig. 3Schematic representation of regions of amplification and deletion on chromosome 21. The x-axis in the graph indicates the genomic position of the multiplex ligation-dependent probe amplification (MLPA) probe site mapped to the human reference genome hg19. The y-axis indicates ratios of the patients' fluorescence peak height relative to the controls' peak height, as determined by MLPA analysis. Regions of amplification are highlighted in red and regions of deletion are highlighted in blue.
|
Table 2
Clinical presentation at diagnosis of the three patients with RUNX1 signal increment by FISH
![]()
2. Clinical presentation and course of the patient with iAMP21
A 9-yr-old boy, the patient C, was admitted because of general weakness for three weeks. At initial diagnosis, he showed the complex karyotype 44,XY,add(4)(p15.2),−5,i(7)(p10),−21, −22,+mar[16]/45,idem,+7[4]. At follow-up one week after the initiation of high-risk chemotherapy comprising the drugs vincristine, prednisolone, and L-asparaginase, a bone marrow examination revealed 76.9% residual blasts in the observed marrow cells and the FISH analysis revealed a 34.8% RUNX1 signal amplification of interphase cells. Chemotherapy with vincristine was maintained for three years after diagnosis; however, a bone marrow examination showed relapse of B-ALL, and the amplification of the RUNX1 signal was also observed. High-risk chemotherapy with vincristine was reinitiated to treat the relapsed B-ALL and bone marrow transplantation from a sibling donor was performed after conditioning chemotherapy. The patient remained in complete remission for eight months; however, a follow-up bone marrow examination revealed a second relapse of B-ALL. After completion of the clofarabine-based reinduction therapy, a complete hematological remission was achieved. The clinical course of the patient is summarized in Fig. 4.
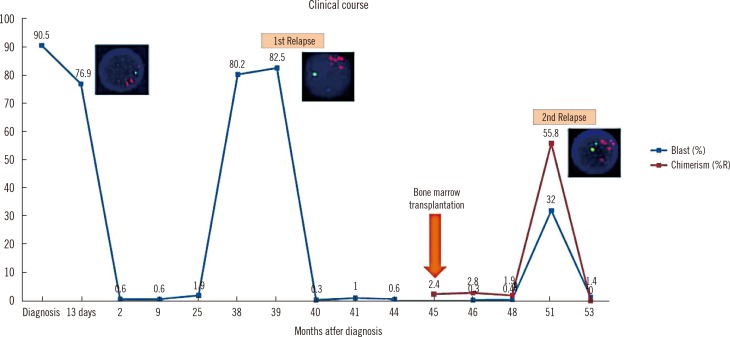 | Fig. 4Clinical course of patient C. The x-axis in the graph indicates the time (months) after diagnosis. The y-axis indicates the percent of blast count in bone marrow (blue line) and percent recipient chimerism as measured by short tandem repeat analysis (red line). RUNX1 signal amplification by FISH analysis was detected at 13 days after diagnosis, first relapse, and second relapse.
|
Go to :
DISCUSSION
iAMP21 is a primary cytogenetic change, which remains constant in structure between diagnosis and relapse [10]. The ALL patients with iAMP21 showed inferior outcomes than those from the other ALL subgroups, including t(9;22), low hypoploidy, and MLL translocation [6]. Our patient also showed an aggressive course, with the first relapse occurring after chemotherapy and the second relapse after bone marrow transplantation, suggesting that one of the effects of iAMP21 is a poor prognosis.
Previous studies reported a common region of amplification spanning 6.6 Mb of chromosome 21 that almost always contained RUNX1; however, other involved regions varied among patients [811]. In addition, a 3.3-Mb deleted region in the telomere was found in a large proportion of patients [10]. The amplified regions of our patient overlapped with the commonly reported amplified regions, including RUNX1 and ERG [8]. The mechanism of this copy number alteration has been explained as chromothripsis following breakage-fusion-bridge cycles, which is often combined with deletions of RB1, ETV6, CDKN2A/B, and IKZF1 [9].
Currently, the recommended laboratory test to detect iAMP21 is FISH, which can also determine copy number, with probes specific for RUNX1 [12]. However, the stratification of patients with interphase cells should be made with caution, because additional RUNX1 signals are also seen in extra copies of chromosome 21, which are characteristic of high-hyperdiploid ALL [7]. The characteristic signal patterns of iAMP21 are noted as clustered RUNX1 signals, with one signal, located apart, representing the normal chromosome 21 [4]. However, because concerns are still present, a distinctive genomic profile of chromosome 21 needs to be used to confirm the accuracy of iAMP21 diagnosis, such as by single nucleotide polymorphism array analysis [13] or FISH with the addition of a subtelomeric probe specific for chromosome 21 [11]. We suggest that MLPA is also helpful to verify iAMP21 in clinical settings.
MLPA is a rapid multiplex PCR-based technique that allows the relative quantification of multiple gene sites in a single test [14]. Although MLPA has a challenge in detection of a low percentage of positive cells in sample, it targets very small sequences and can distinguish between those differing by a single nucleotide.
To our knowledge, no study has reported a case of iAMP21 in Korea. The prevalence of iAMP21 in childhood leukemia in our study (1/102 patients, 1.0%) is comparable to that of previous reports [5712]. In our report, the impact of the iAMP21 on disease course appeared to be very unfavorable. To determine the exact frequency and clinical impact of iAMP21 in Korean patients, appropriate test strategies to detect iAMP21 are warranted. To consider the prognostic implications of iAMP21 in patients with ALL, we suggest the inclusion of the MLPA test to detect iAMP21 in the initial diagnosis of ALL.
Go to :
 XML Download
XML Download