

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Orbital floor fracture is one of the most common facial skeleton fractures after mid facial trauma, accounting for up to 40% of craniofacial injuries [12]. Patients may complain of ocular symptoms, aberration of aesthetic appearance, and dysesthesia around the damaged cheek. The goal of treatment is restoration of the anatomic and functional defects of the globe. Recently, numerous approaches for reduction of orbital floor fractures have been proposed including transorbital, transantral, and transnasal using endoscopy [3456]. Various materials have been introduced to cover the floor defect, or support the prolapsed orbital contents from the maxillary sinus [578]. Several alternate materials used to support the orbital floor in the maxillary sinus via a transantral approach, include hydroxyapatite block, silicone block, and balloon and gauze soaked with iodine formaldehyde. Potential problems with these methods are instability, implant displacement, inadequate reduction, infection, and cost [91011]. We propose the use of a silicon tube for the reduction of blowout fractures of the inferior orbital wall via a transantral approach. The aim of this study was to evaluate the usefulness, advantages and limitations of the proposed technique.
MATERIALS AND METHODS
Patients
Fifty-one patients with pure blowout fracture of the inferior orbital wall from January 2000 to December 2011, at the Department of Otolaryngology-Head and Neck Surgery of Maryknoll Medical Center were included in the study. All enrolled patients underwent reduction surgery using folded silicon tube placement via the transantral approach. Clinical indications for fracture repair included persistent diplopia (>2 weeks), extraocular muscle entrapment on face computed tomography (CT) scan, a large posterior fracture (>50% of the orbital floor), or early enophthalmos [581213]. Exclusion criteria were as follows: (1) patients with orbital floor fractures, who did not undergo reduction surgery; (2) patients with accompanying ethmoidal, maxillary, or zygomatic bone fractures; (3) insufficient medical data (preoperative and postoperative CT scans, operation, and medical records); (4) patients, who underwent surgery with other implanted materials; (5) patients, who did not follow up for more than three months despite persistent orbital symptoms; (6) patients, who underwent reduction surgery via both transantral and transorbital approaches; (7) patients, who underwent simultaneous reduction surgery for both orbital floor and medial wall fractures. All protocols were approved by the Kosin University Institutional Review Board (IRB No. 12-104).
Analysis
All patients received a complete, preoperative and postoperative ophthalmic examination for visual acuity, diplopia, extraocular muscle limitation, and enophthalmos. Diplopia in the cardinal fields of gaze was considered significant. Enophthalmos was regarded as significant if a 2-mm discrepancy between eyeballs existed. A Hertel exophthalmometer was used for measurements a day presurgery and 4 weeks postsurgery. Facial CT was performed in all patients, preoperatively and postoperatively. The mean displacement between fractured bone chip and intact orbital floor was based on anatomic positioning on CT scans. Displacement was classified as: grade I, an exact anatomic position of reduced orbital floor or minimal displacement; grade II, discrepancy of displacement below 2 mm; and grade III, a discrepancy of displacement above 2 mm. Complications and management strategies were evaluated by chart review.
Operation technique
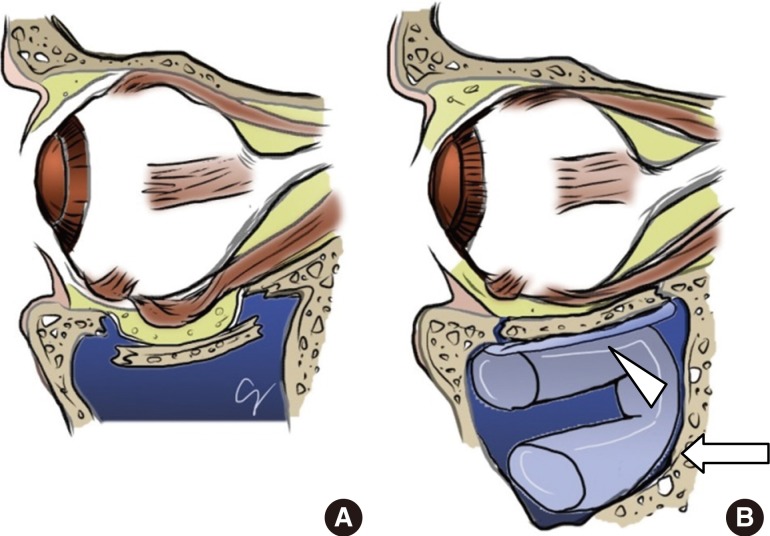
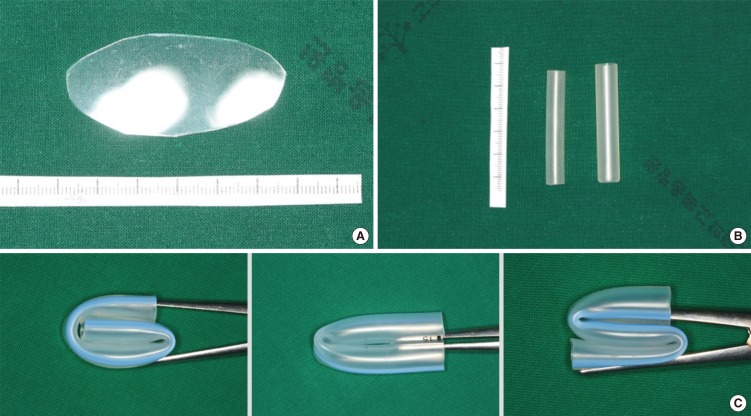
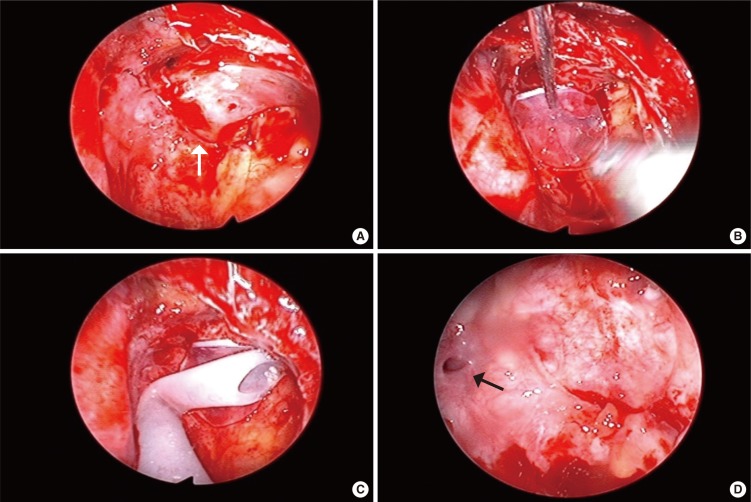
Surgical procedures were performed under general anesthesia. Typically, 1% lidocaine with 1:100,000 dilution of epinephrine was injected into the upper gingivobuccal sulcus. A 3- to 4-cm horizontal incision was made just superior to the sulcus. The periosteum and overlying soft tissue were gently elevated from the underlying maxillary bone to the infraorbital foramen using a periosteal elevator. An antral window (2 cm×1.5 cm) was made into the maxillary sinus with an electric saw. The bone fragment was preserved in saline solution for repositioning at the end of surgery. The maxillary sinus and prolapsed orbital contents were visualized employing a 0-degree endoscope, through the antral window. The herniated orbital contents were reduced by digital manipulation or by using surgical instruments like an elevator, without removing the mucosa and fractured bone chip. A silastic sheet (1 mm), slightly larger than the fractured area, was inserted into the maxillary sinus and placed below the orbital floor. A silicon tubing (1 mm in adult and 0.5 mm in pediatric cases) was bent one or two times, and inserted into the maxillary sinus under the silastic sheet (Fig. 1). When placed into the maxillary sinus, the tube recoiled automatically and adjusted to the sinus wall to firmly support the reduced orbital floor with its elasticity (Fig. 2). Care was taken not to obstruct the natural ostium of the maxillary sinus (Fig. 3). A forced duction test was performed to confirm correct positioning of the orbital floor and to avoid entrapment of the orbital contents before closing. The antral wall fragment, stored in saline, was fixed in its original position using a plate and screws. The gingivobuccal incision was closed, and postoperative antibiotics were continued for 14 days. The silastic sheet and tube were removed 6 to 8 weeks postsurgery under local anesthesia through the same antral maxillary window, created during the first surgery (Fig. 4). The second surgery was performed under general anesthesia in all children and some adults.
RESULTS
Among the 51 patients included, 39 were male and 12 were female. The mean age of the patients was 31 years (range, 12 to 69 years). Trauma occurred on the right side in 24, the left side in 26, and on both sides in one patient. The patient with both orbital wall fractures had surgery performed through the more grossly damaged side. Forty-three patients had inferior orbital wall fractures. Eight patients with combined inferior and medial orbital wall fractures underwent reduction surgery for orbital floor fractures only, because of disregarded medial wall fractures. The most common causes of fracture were falls, assaults, sports injuries, and industrial accidents. The mean interval between injury and repair was 8.5 days (range, 2 to 35 days) and the mean length of follow-up was 87 days (range, 28 to 401 days).
Ophthalmic symptoms
Twenty-five patients reported diplopia before surgery, of which postoperative improvement was seen in 18 patients. In seven patients, diplopia persisted at extreme upper gaze postsurgery, but disappeared within the 3-month follow-up period. Thirteen out of 15 patients had improved extraocular muscle limitation postoperatively. Enophthalmos resolved postoperatively in four of five patients (Table 1).
Discrepancy between fractured bone chip and orbital floor based on CT scan
Preoperatively, there were three cases of grade II and 48 cases of grade III displacement. All three preoperative grade II cases were restored to grade I postoperatively. Among 48 patients with a preoperative status of grade III, 16, 25, and seven cases had grades I, II, III, respectively, postoperatively (Table 2).
Complications and management
Inflammatory changes of maxillary sinus mucosa were observed in 21 patients upon silicone tube removal. The inflamed mucosa was either shaved using a microdebrider after removal of the implants, or left undisturbed. One patient complained of severe diplopia, ocular pain, and aggravated extraocular muscle limitation after surgery. The symptoms were attributed to overcorrection of the fractured bony fragments, and were alleviated after immediate revision surgery. A patient, 3 days postsurgery, presented extrusion of the silicon tube through the maxillary sinus window. Corrective implant repositioning was achieved by revision surgery. Another patient developed maxillary sinusitis at 4 weeks postsurgery, with symptoms of cheek pain, swelling, and nasal discharge. The sinusitis symptoms resolved on removal of the implant. These results are summarized in Table 3.
DISCUSSION
The orbital floor can be accessed through a transorbital, transantral, or endoscopic transnasal approach [3456]. The transorbital approach has a limited ability to restore large floor defects and access the posterior orbital region; it also leads to unsightly facial scars or eyelid complications [1415]. The transantral approach is clinically useful in cases involving severe fractures or posterior floor fractures; it has the advantage of providing a direct view of the defect size and configuration, and preventing injury to lower eyelid structures. However, the transantral approach can lead to entrapment of the extraocular muscle in trapdoor-type fractures, and lead to infraorbital nerve injury [101617]. Recently, an endoscopic endonasal approach for orbital floor fracture was introduced [5]. However, it is only suitable to limited cases of medial or posterior orbital floor fractures.
Reports on the transantral approach, have discussed various materials for supporting the fractured orbital floor and filling up the maxillary sinus. These materials include iodophor gauze, hydroxyl appetite block scaffolding, silicone block, and sinus balloons [79101118]. However, the techniques of implant placement within the maxillary sinus to reduce fractured orbital floors are limited due to the difficulty in restoring orbital floor anatomic positioning. Furthermore, these techniques increase the risks of extrusion, migration, and infection. The procedure can be prohibitively expensive, and requires a second surgery for implant removal [91019]. These limitations have restricted the widespread use of transantral approach.
In this study, we used folded silicon tubing to uphold the fractured orbital floor in the maxillary sinus. Implanting bent silicon tubes provided several benefits: (1) Silicon tubes were bent and easily fitted into the maxillary sinus, thus shortening operation times; (2) The elasticity of the silicon tube maintained the orbital floor in a stable anatomic location until implant removal; (3) A more physiological healing was attained because the sinus mucosa and fractured orbital bone chips were not removed; (4) The material is inexpensive; and (5) It is suitable for addressing relatively large and posterior orbital floor fractures. The shortcomings of this technique are as follows: (1) Secondary surgery is needed to remove the implant (note that the surgery can be performed easily under local anesthesia through the previously constructed maxillary window); and (2) Transient inflammatory changes of the maxillary sinus mucosa can occur.
Postoperatively, diplopia improved but persisted with maximum upward gaze in seven of the 25 patients. All diplopia symptoms resolved within the 3-month follow-up. Similarly, Folkestad and Westin [9] reported 38% postoperative diplopia in patients, who underwent operative repair using balloon and iodine formaldehyde soaked gauze via a transantral approach. Four of the five patients with enophthalmos, experienced resolution postsurgery. Ikeda et al. [5] reported two cases of postoperative enophthalmos of the 11 surgically treated cases of orbital floor fractures. Even though this study included treatments of more challenging posterior orbital bone fractures and large fractures, our results showed acceptable outcomes.
This surgery has physiological advantages, with respect to that it not only reduces periorbital soft tissue but also restores fractured bony fragments and mucosa to their original anatomic positions. Thus, overall, there is more stable restoration and a decrease in ophthalmic complications.
Entrapment of periorbital soft tissue can occur, in trapdoor-type fractures, but can be resolved by employing a combination transorbital approach [20].
Twenty-one patients in the current study had mild polypoid changes in the maxillary sinus mucosa on implant removal. This postoperative inflammatory change was not significantly different from that which occurs with other filler materials (e.g., hydroxyapatite block, silicon block, or gauze soaked with iodine formaldehyde) implanted via a transantral approach [91011], and the inflammation was supposed to be spontaneously resolved after implant removal.
There were three cases with complications that were successfully treated by revision surgery. One female patient (on no antibiotics) had acute sinusitis, which resolved after implant removal. The second case involved extrusion of implants. The third complication case was overcorrection, which occurred among the early surgeries, when surgeons were still perfecting this technique.
In summary, using folded silicon tubing to repair orbital floor fractures can yield exact positioning of fractured bone and promote physiological healing. It is an easy, economical, and safe procedure compared to previously used implant materials for transantral procedures. It is proposed that this procedure can be a novel surgical option for orbital floor fracture reduction.

 XML Download
XML Download