

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
A common potential problem with traditional canal wall down (CWD) mastoidectomy procedures in treating cholesteatoma is the long-term morbidity associated with discharging cavities [1]. CWD is a destructive approach, insofar as it involves creating an open cavity and altering the anatomy and physiology of the middle ear and mastoid. This can result in frequent ear discharge, difficulty in fitting a hearing aid, the need for water precautions and a potential lifetime of visits to outpatients for aural care with significant socioeconomic impact [2]. Several surgical techniques have been described with modifications and today there is no general consensus about the optimal procedure.
A canal wall up (CWU) technique eliminates the need to destroy the middle ear and mastoid, but it is associated with a higher rate of residual cholesteatoma [34]. In 2002, we decided to find out whether it is possible to combine the advantages and, at the same time, avoid the disadvantages of both the CWU and CWD techniques. Our approach was mastoid and epitympanic bony obliteration followed by posterior bony canal wall reconstruction (CWR) and ossiculoplasty without staging. According to the preliminary results, this technique is promising; however, longer follow-up is necessary to assess the durability of the procedure.
In this study, we studied the long-term condition of ears that underwent CWD mastoidectomy with mastoid and epitympanic obliteration and posterior wall reconstruction using a free bone-connective tissue composite graft, autogenous bone chips, bone pâté and a rectangular superiorly meatal pedicle flap. All the patients that participated in the study were followed at least for 4 years. The surgical results, the degree of hearing restoration and the changes of the configuration of the cavity will be discussed in our report.
MATERIALS AND METHODS
The study was performed as a retrospective chart review between January 2002 and October 2009 in the Tri-Service General Hospital, Taiwan. Our clinical database included a total of 103 patients who underwent mastoidectomy, with ages ranging from 16 to 72 years. Patients were included in this study if they underwent CWD mastoidectomy, mastoid and epitympanic obliteration, CWR, and ossicular chain reconstruction without staging. Seventeen patients in the study received surgery for the first time in the involved ear (primary cases) and 27 patients had previously received surgery in the involved ear (revision cases). Patients with follow-up period less than 48 months were excluded from this study. All surgeries were performed by the corresponding author, a senior otolaryngologist. A database was created which included: patient age, gender, etiology, operative details, and surgical complications. They also underwent high-resolution computed tomography (HRCT) scans of the temporal bone before surgery. All patients were evaluated postoperatively by follow-up surgical microscopy. Perioperative pure tone audiometry thresholds (0.5, 1, 2, and 4 kHz pure tone average [PTA]) via air conduction (AC) and bone conduction (BC) were determined and the air-bone gap (ABG) was calculated. Both the paired t-test and McNemar test were used for statistical analysis; differences were assumed significant at P<0.05.
Surgical technique
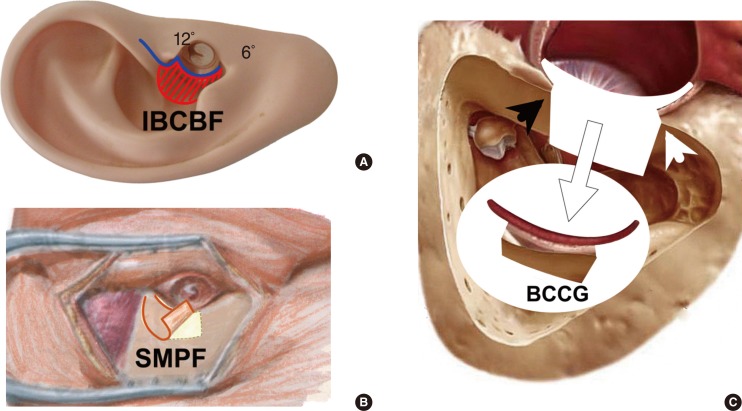
Under general anesthesia, an endoaural incision was made as Heermann B incision (Fig. 1A) and the posterior canal skin was elevated from medial to lateral direction. Then, the skin and subcutaneous tissues about 1-2 cm behind the postauricular sulcus were incised sharply down to the temporalis fascia and the periosteum overlying the mastoid cortex. The incision went behind the postauricular muscle and the perosteum was elevated around the ear canal to meet the Heermann's incision at 12 o'clock to become an aurical-canal skin flap, using self-retaining retractor to push it forward and expose the tympanic membrane.
From the postaural region, a large piece of temporalis fascia about 10 mm×15 mm was harvested. A rectangular superiorly meatal pedicle flap about 15-mm width and 25- to 30-mm length was elevated (Fig. 1B). In the same plate, a free bone-connective tissue composite graft 20 mm×20 mm was harvested with a 6-mm osteotome from the mastoid cortex around the mastoid tip (Fig. 1C). This composite graft was composed of subcutaneous tissue and fractured bone with/without periosteum; depended on its previous surgical condition. Bone chips also collected with the same osteotome. We collected bone pâté as we drilled the mastoid cortical bone using 4- to 5-mm cutting burr until the first mastoid air cell is opened. The bone pâté and chips are extensively irrigated with physiologic water until it is free of blood and is soaked with antibiotic solution (Gentamicin; 40 mg/mL, 2 mL in 20 mL physiologic water; Winston Medical Supply Co., Tainan, Taiwan) to decrease the risk of infection.
Following the elevation of the tympanomeatal flap, a retroauricular tympanotomy was made to remove all diseased tissues in middle ear. A complete CWD mastoidectomy is then performed, including the exenteration of the sinodural, retrofacial, retrosigmoid, and mastoid tip cells but some portion of anterior and posterior buttress of facial ridge was preserved as a guideline for keeping the reconstructed posterior canal wall in the nearly natural position. All of cholesteatoma, diseased soft tissues, and polyps were cleaned. The incus and malleus head are removed using a malleus nipper, and the malleus handle is cleaned free of connective tissue and mucosa and preserved for later reconstruction. The oval window niche, including the stapes or its remnants, is carefully cleaned.
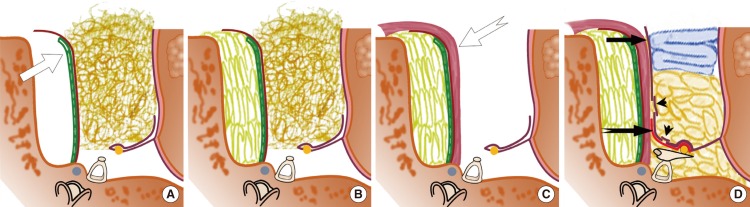
Reconstruction starts by reconstructing the posterior bone canal wall with a free bone-connective tissue composite graft. To keep it firmly in the desired position, we packed an ear mold inside the external ear canal made from wet cotton (Fig. 2A), which was shaped to closely mimic the normal anatomic dimensions. Next we completely fill the mastoid cavity and the entire attic region with bone chips and pâté, using the method we called "parallel overlapping stacking method" (Fig. 2B). The superiorly meatal pedicle flap was used to shield the anterior surface of the free bone-connective tissue composite graft (Fig. 2C). The ossicle chain was reconstructed with autologous incus or autologous bone fragment in one stage. The tympanic membrane was then reconstructed by temporalis fascia graft (Fig. 2D). In cases with obvious canal skin loss during CWD procedure, the split-thickness skin graft is used to enhance the canal epithelization. The final step of reconstruction is to insert gelfoam in the middle and external ear canal to keep the temporalis fascia graft and ossicle prosthesis in place. External auditory meatoplasty was performed to prevent postoperative stenosis of meatal orifice by using Wolfensberger's Inferiorly based conchal bowl flap (Fig. 1A) [5]. This flap also was used to overlap most of the superiorly meatal pedicle flap (Fig. 2D) and was fixed in place with Sofra-tulle dressing (Hoechst Marion Roussel, Zürich, Switzerland).
In revision cases with previous CWD mastoidectomy, the technique was the same for primary cases, except in revision cases, the medial circumferential incision was made on the bony facial ridge instead on the posterior canal wall because the ears in revision cases no longer had any posterior bony wall. An additional bone plate was harvested for posterior wall reconstruction and bone chips or pâté were collected from the lateral cortical bone as those mentioned above. In revision cases, most of the cases still had high facial ridge with sharp anterior and posterior buttresses, which was important for posterior wall fixation. The superiorly meatal pedicle flap was designed mainly as the primary patients, although the fibrosis might impede this step. The wound was closed as usual. An intravenous antibiotic was administered perioperatively, and amoxicillin-clavulanate tablets were prescribed for 10 days postoperatively. Careful follow-up included repeated clinical examinations, and referral for HRCT if suspicious recurrence.
RESULTS
Forty-four patients met the study criteria, 21 men and 23 women with average age of 45 years (range, 17 to 69 years). The mean postoperative follow-up was 88 months (range, 49 to 741 months). This was the first operation on the involved ear for 17 patients (primary patients), and 27 patients previously received surgery in the involved ear (revision patients) (Table 1). The middle ear was well healed and aerated in 17 of the primary patients (100%) and in 23 of the revision patients (85.2%). The tympanic membrane was intact in 17 of the primary patients (100%) and in 25 of the revision patients (92.6%) (Table 2). Recurrent cholesteatoma was found on postoperative follow-up in two of the revision patients (7.4%) but none in the primary patients.
Six of the revision patients and one of the primary cases were found on follow-up to have partial canal bone absorption, but revision surgery was not required. The facial nerve was dehiscent in its tympanic portion in five patients. One patient suffered from delayed temporary facial weakness for 10 days postoperatively, but returned to normal function 3 weeks later. No other major complication was encountered.
All patients underwent complete hearing evaluation and the mean AC, BC, and ABG values (±standard error of the mean) at different time points shown in Table 3. The mean preoperative PTA-AC was 44.7 dB with a mean preoperative PTA-ABG of 25.0 dB. Postoperative hearing results were assessed after 1 and 4 years and revealed a mean gain on PTA of 4.5 and 2 dB, respectively. The mean improvement in the ABG at 1 and 4 year postoperative follow-up was 4.4 and 2.2 dB, respectively. The PTA-ABG improvement at 1-year follow-up was statistically significant (paired t-test, P<0.05), as compared to the preoperative value. Thirty-one patients (70.4%) had excellent (0 to 10 dB) or a good (11 to 20 dB) gap closure one-year after the evaluated surgery. Finally, 28 patients (63.7%) had excellent or good gap closure in the operated ear at the 4-year follow-up (Table 4). Those improvements, both 1 and 4 years after surgery, were statistically significant as compared to that before surgery (McNemar test, P<0.05). Conductive hearing loss persisted in some individuals because of continued eustachian tube dysfunction. No attempt was made to offer ventilation tubes to this population because a dry, safe ear was the primary goal. None of the patients in this series experienced complete hearing loss.
DISCUSSION
The CWD procedure involves taking down the posterior canal wall to the level of the vertical segment of facial nerve and marsupializing the mastoid into the external ear canal. As compared to the CWU procedure, the removal of the bony canal during the CWD procedure improves exposure and facilitates the complete removal of all cholesteatoma [6]. However, it is also known that this approach will lead to the creation of an open cavity with numerous disadvantages. It is less performed today but in patient with a cholesteatoma and poor eustachian tube function as evidenced by absence of middle ear aeration and a sclerotic mastoid, the CWD procedure remains an option [7].
Aimed at solving these problems mentioned above, surgeons have attempted reconstruction with a variety of techniques and materials [8]. Two general strategies have been attempted: reconstruction of an anatomically correct canal wall and complete obliteration of the mastoid cavity [89]. Several surgeons performed staging in CWD procedures with reconstruction, due to the risk of residual cholesteatoma [2910]. A disadvantage with this technique is the delay in hearing reconstruction. Another disadvantage is the additional surgery. Our preference is to perform the CWD procedure where the mastoid cavity and epitympanic spaces are widely exposed and hermetically sealed with autologous materials. The ossicular chain and posterior canal wall is reconstructed consequently without staging. Long-term stable hearing can be obtained using this approach. The results of the current series demonstrate that our technique has an advantage over other CWD procedures in terms of water safety. Specifically, 86.4% of the postoperation ears were water-safe, 95.5% had intact tympanic membranes, and 90.9% had aerated tympanic cavities. Subsequently, eardrum retractions were found in 3 patients (6.8%) with surgical microscope at the regular clinical examination.
Negative pressure in the middle ear and mastoid likely contribute to the recurrence of cholesteatoma. Inflammatory conditions will result in more negative middle ear pressures because more gas is absorbed from diseased mucosa [78]. Exenteration of the mastoid epithelium, followed by obliteration, can minimize the potential problems by reducing the size of the mastoid cavity and promoting epithelialization over the exposed mastoid bone [1112]. It may decrease the volume of air absorption from the middle ear and mastoid [1314]. Roberson et al. [8] found that mastoid obliteration often normalized eustachian tube function and aeration of the mesotympanon in a majority of patients. This could prevent development of retraction pockets and reduce the incidence of recurrent cholesteatoma compared with CWU techniques. In this series, no patients had residual cholesteatoma but the recurrence rate was 4.6% (2/44), which is similar to low recidivism rates published for CWD mastoidectomy, after a mean follow-up of 88 months.
We prefer to use autologous material such as bone chips, bone pâté and the free bone-connective tissue composite graft in mastoid obliteration. These materials are readily available in primary and revision cases and in our experience produce excellent results. To avoid collecting the fillers contaminated with infected mucosa or squamous epithelium, it is best to collect them from the lateral cortical bone. It is our experience that sufficient bone is available at the mastoid cortex; if not, as may be the case in revisions, exposure of the temporal squamous bone or postsigmoid bone can provide sufficient bone chip or pâté. Meanwhile, the autologous filler is impregnated with antibiotic solution, the gentamicin solution, at the time of harvest to decrease the risk of infection. The epitympanum and antrum are specifically addressed and obliterated to closely mimic the normal anatomic dimensions of the external auditory canal. This maneuver prevents a recurrent pocket for debris trapping or cholesteatoma to recur. Once the chip or pâté is placed, it is important to ensure complete coverage with the pedicle flap to prevent its dissolution. Black [15] reported an infection rate of 16% in a series of 55 patients using autologous bone and reported a long-term failure rate of 52%. Roberson et al. [8] reported an infection rate of 13.8% in 62 patients and a resorption rate of 4.8% when using bone pâté washed with antibiotic solution. In this study, there were two patients (4.6%) who suffered from postoperative infection and partial obliteration material resorption was observed in seven patients (15.9%). Both the cortical bone chips, pâté, and soft tissue flap atrophied with a resultant increase in the size of the cavity but tend to be stabilized within one year after surgery. The reconstructed canal might enlarge progressively, but the result was acceptable and they were all well tolerated to hearing aid. Only one patient in this series suffered from flap breakdown and near-total graft absorption. A rotation flap was used in salvage surgery.
Our approach improves exposure and removal of cholesteatoma as in a CWD only approach while retaining the benefits of an intact canal wall for improved hearing and avoidance of the bowl cavity. Reconstruction is often done with bone plate, cartilage or prosthetic material. Some reports describe removing the posterior bony wall and reinforcing it with fascia or other materials when it is replaced [9]. Long-term, stable canal reconstruction is achievable in 75% of patients as demonstrated by Grote and van Blitterswijk [16] in a 15-year follow-up of 60 patients undergoing reconstruction with a preformed hydroxyapatite prosthetic external auditory canal prosthesis. In our experience, reconstruction of the posterior wall to closely mimic the normal anatomic dimensions is possible in all patients by using the free bone-connective tissue composite graft and the pedicle flap. One of the benefits of our procedure is the use of the patients' own tissue to accomplish the result. When an autologous free graft is covered by a piece of living tissue, it can get nourishment directly. However, if grafts are placed over nonvascular materials, they could break down and lead to exposure of the underlying materials and become infected. The goal of the CWR technique is to produce an epithelium-lined skin rich in blood supply inside the external auditory canal, which is critical for producing a healthy canal. To promote epithelialization, we use the superiorly meatal pedicle flap then overlaid it with the inferiorly based conchal bowl flap.
We observed obvious retraction of the reconstructed canal wall towards the posterior in seven patients (15.9%) in our current series. To measure the ear canal volume, we had used 37℃ normal saline and put it into the ear canal, before canal packing and three months after operation. The canal shape changed time to time, from nearly cylindrical shape to conical shape. The canal volume changed from 1.0-1.2 mL to 1.6-1.7 mL in four of revision cases (not shown in this paper). There were some cases having shallow retraction but no pocket or deep cavity formation in the attic and posterior tympanic region. The retraction is caused by the reduction in volume of the filling in the mastoid cavity. Recall that during reconstruction we fill the mastoid cavity and the entire attic region with bone chips and pâté. We believe as surrounding tissues absorb nitrogen, the space surrounding each added bone material decreases, thereby causing a reduction of the total volume of the filling [1]. Another potential cause of such shrinkage may be the absorption of the added bone material [17]. In order to minimize the retraction of the reconstructed canal wall, the surgeon should fill in the mastoid cavity with care to decrease the spacing between added bone materials.
Achievement of middle ear aeration is necessary for successful hearing reconstruction. Our technique of CWR is able to re-create a more lateral tympanic ring, allowing formation of an adequate middle ear space for ossicular reconstruction, resulting in hearing improvement. Brown [18] found that only 34% of adults and 28% of children who received a traditional modified radical mastoidectomy had "serviceable" hearing, defined as an AB gap of ≤20. In contrast, 62% of adults and 66% of children with CWU mastoidectomy had serviceable hearing. Likewise, Tos and Lau [19], in a study with a mean observation time of 9.3 years, found that although 36% of patients with a CWD mastoidectomy had an AB gap ≤20, 50% of patients with an CWU mastoidectomy had an AB gap ≤20. Our overall long-term hearing outcomes are comparable to other authors' results for CWU mastoidectomy with 70.4% (31/44) and 63.7% of patients (28/44) having an ABG of 20 dB or less at 1 and 4 years postoperation, respectively. The results show that it is possible to combine the advantages of both the CWU and CWD techniques with serviceable hearing results and complete removal of cholesteatoma. No patient experienced worsening of hearing when comparing final results with presenting PTA. In those ears where hearing does not improve to functional levels, patients are able to wear a hearing device with less risk of infection and complication
Consequently, the presented surgical technique without staging seems to provide long-term dry, safe, and water-resistant ears with stable improvement of hearing. Although shrinkage of the obliterated mastoid and re-formed wall can not be avoided completely, the result was acceptable and they were all well tolerated to hearing aid. Our procedure would not be suitable for those with severe mastoid cholesteatoma. If the cholesteatoma can not be cleared from the mastoid cell tracts, obliteration is contraindicated. Finally, although the recurrence rate in our series was quite low, long-term otoscopic follow-up combined with magnetic resonance imaging/HRCT remains the standard protocol for the early detection of cholesteatoma recurrence.
In conclusion, mastoid obliteration and CWR should be considered a routine part of CWD mastoidectomy and can be performed without staging. Our results indicate good overall success for the stability of the tympanic membrane, hearing preservation/restoration, and disease control. Therefore, we recommend the presenting technique for patients with extensive or recurrent cholesteatomas involving the middle ear or mastoid cavity, for whom adequate mastoid air cells eradication is imperative.
 XML Download
XML Download