

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Papillary thyroid carcinomas (PTCs) may occur as two or more separate foci within the thyroid gland. The frequency of such multifocal PTCs has been reported as 18%-87%, varying depending on the diagnostic techniques [1,2,3,4,5,6]. Multifocal PTCs have been associated with the increased risks of lymph node metastasis, distant metastases, persistent local disease after initial treatment and regional recurrence [1,3,4,6,7]. All these features warrant more aggressive treatment for multifocal PTCs [8,9,10].
However, additional tumor foci are smaller than the representative tumor and frequently not diagnosed preoperatively. In many cases, those multifocal tumors are incidentally found by pathological analysis. Importantly, preoperatively undiagnosed contralateral tumor foci can lead to undertreatment and remnant disease after initial surgery, especially, in cases of papillary thyroid microcarcinomas (PTMCs) which are frequently managed with lobectomy alone. However, the diagnostic accuracy of preoperative radiologic tests for multifocal PTMCs has not been not well investigated and there are no known predictor for multifocal or bilateral tumors.
In this study, we aimed to study the incidence of multifocal PTMCs, diagnostic accuracy of preoperative radiologic evaluation, predictive factors, and the chance of bilateral tumors.
MATERIALS AND METHODS
Patients
A total 300 patients with PTMC underwent thyroidectomy at Samsung Medical Center, Seoul, Korea, from January 2008 to December 2008. Of those patients, 13 patients who received thyroid lobectomy and 10 patients without available preoperative radiologic tests were excluded. As a result, 277 patients with PTMC who underwent total thyroidectomy were included in this study. Central neck dissection was performed for 253 patients and lateral neck dissection for 2 patients. Diagnosis of PTMC was reconfirmed by the surgical pathology for all patients. Ultrasound (US)-guided fine needle aspiration was performed for the representative largest tumor and contralateral suspicious nodule. Radiologic accuracy was studied in 274 patients, excluding 3 for whom the exact number and location of tumors are not clearly described on the radiologic reports. Preoperative US reports were available in 235 patients. For 39 patients without available US reports, computed tomography (CT) reports were reviewed.
Clinicopathological parameters
The mean age of the patients was 49.3±9.4 years. The study included 225 females and 52 males. Medical records, pathologic reports and radiological reports were reviewed for analysis. Clinicopathological characteristics of the 227 patients are presented in Table 1.
Statistical analysis
Descriptive statistics was presented regarding to multifocal tumors and bilateral tumors. For 274 patients excluding 3 patients for whom the exact number and distribution of tumors are not definitely described on the radiologic reports, sensitivity, specificity, positive predictive values and negative predictive values of CT/sonography for multifocal tumors and bilateral tumors are calculated. Including those 274 patients, correlation between unilateral multifocal tumors and bilateral tumors was analyzed using Fisher exact test. Paired t-test was performed to compare the size of largest primary tumors and secondary tumors in each case, including 94 patients for whom the size of primary and secondary tumors are available. Chi-square test and Fisher exact test were used to analyze the significance of difference in the proportion of variables (univariate analysis). Logistic regression analysis was performed for multivariate analysis to determine significant factors associated with multifocal tumor. All statistical analyses were performed using SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA) and significance was accepted at P<0.05.
RESULTS
Characteristics of multifocal PTMC
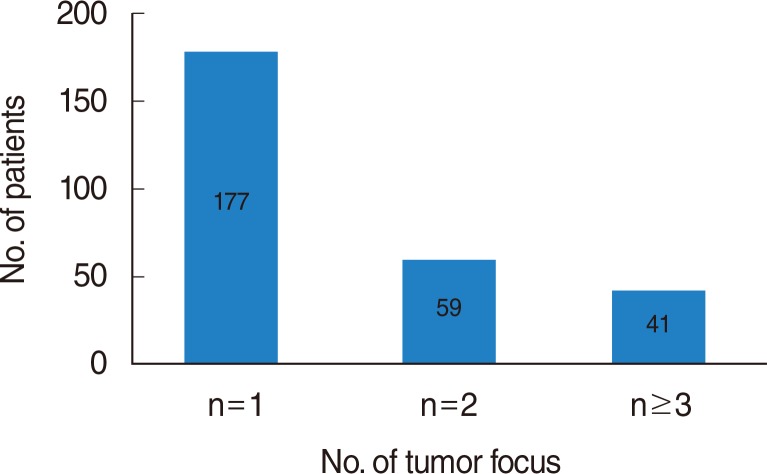
Multifocal PTMCs were detected in 100 of 277 patients (36.1%). The mean number of tumors in each patient was 1.6±1.1, ranging from 1 to 10. One hundred seventy seven patients (63.9%) had single tumor focus, 59 (21.3%) had 2 foci, and 41 (14.8%) had 3 or more foci (Fig. 1). The mean size of the largest primary tumor in each patient 0.6±0.2 cm. The other tumors of each patient were much smaller and had not been preoperatively detected by US±CT in most cases. In 94 cases of available size data on multifocal tumors, the mean number of secondary tumors of each patient was 0.32±0.18 cm. in these 94 cases, the mean size difference between primary and secondary tumors was 0.30±0.23 cm (paired t-test, P<0.001) (Table 2).
Extrathyroid extension was significantly more frequent in multifocal PTMC group than in unifocal PTMC group (71% vs. 52%, P=0.001). Similarly, lymph node metastasis was more frequent in multifocal PTMC group, albeit without statistical significance (38.0% vs. 28.2%, P=0.062).
Bilateral tumors
Bilateral PTMCs were detected in 63 of 277 patients (22.7%). There was no significant relationship between primary tumor size and the presence of contralateral tumors; the mean size of primary tumor was 0.58±0.23 cm in 214 patients without contralateral tumors and 0.63±0.22 cm in 63 patients with contralateral tumors (t-test, P=0.117).
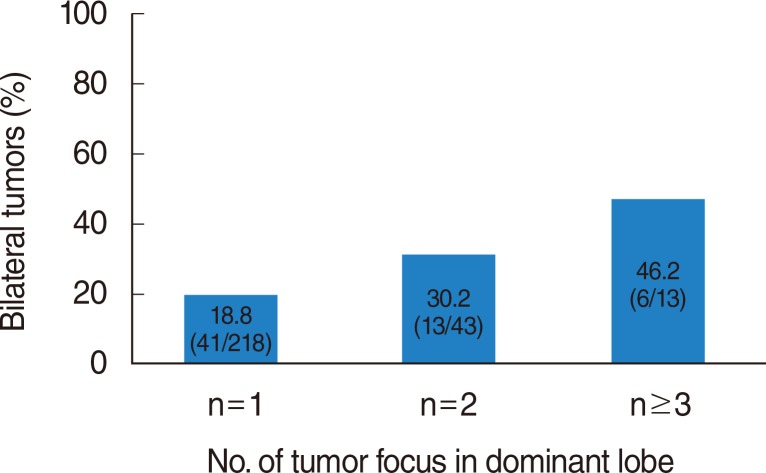
With more tumors detected in dominant lobe (in which the largest primary tumor is present), there was greater chance of contralateral tumors (Fisher exact test, P=0.024). Contralateral tumors were detected in 41 of 218 cases (18.8%) with single tumor focus, in 13 of 43 cases (30.2%) with 2 tumor foci, and in 6 of 13 cases (46.2%) with 3 or more tumor foci in dominant lobe (Fig. 2).
Accuracy of preoperative radiologic examination
Sensitivity and specificity of preoperative US were 42.7% and 92.2% for multifocal tumors. Sensitivity and specificity of preoperative CT were 29.4% and 95.5% for multifocal tumors (Table 3). Sensitivity and specificity of preoperative sonography were 49.0% and 93.5% for bilateral tumors. Sensitivity and specificity of preoperative CT were 28.6% and 100% for bilateral tumors (Table 3).
Relationship between multifocal tumors and other clinicopathological characteristics
Multivariate analysis involving clinicopathological parameters (age, sex, primary tumor size, presence of nodular hyperplasia, presence of lymphocytic thyroiditis) showed that nodular hyperplasia was predictive of multifocal tumors (logistic regression test; odds ratio, 3.396; P<0.001) (Table 4). The incidence of multifocal tumors was higher in the cases with primary tumor >0.5 cm (40.1%) than in cases with primary tumor ≤0.5 cm (31.5%), albeit without statistical significance (logistic regression test, P=0.064).
For bilateral tumors, nodular hyperplasia and number of tumors in dominant lobe were the significant predictors. There was a tendency of increased bilateral tumors in cases with thyroiditis, although without statistical significance (Table 4).
DISCUSSION
PTCs often arise as multiple tumor foci in individual thyroid glands. The clonal origin of the multifocal PTCs has been investigated, but has not been completely settled. In the past, those multiple tumor foci were considered as the result of intraglandular metastasis of a single primary tumor via intraglandular lymphatics [3,5,11]. However, with the advance of modern molecular techniques, there have been reports that the multifocal PTCs are multiple synchronous primary tumors arising from independent clones [12,13,14].
Although the multifocal PTCs can be just synchronous tumors, not the metastatic foci of the largest primary tumor, they have been associated with increased risks of lymph node metastasis, distant metastasis, persistent local disease after initial treatment, and regional recurrence [1,3,4,6,7]. Those studies suggest more aggressive treatment for multifocal PTCs, i.e., total thyroidectomy, central neck dissection, or postoperative radioactive iodine treatment. Concordantly in this study, extrathyroid extension and lymph node metastasis were more frequent in multifocal PTMCs than in unifocal PTMCs.
However, multiple small tumor foci are often undiscovered with preoperative radiologic evaluation and incidentally diagnosed by surgical pathology. In this study, the sensitivity of preoperative US for multifocal tumors was only 42.7%. The sensitivity of preoperative US for bilateral tumors was 49.0%. Because the mean size of secondary tumor was significantly smaller (0.32 cm) than the largest primary tumor (0.63 cm, P<0.001) (Table 2), those small tumors may be difficult to be diagnosed by routine US evaluation. The meticulous diagnosis of those small tumor less than 0.5 cm is not recommended according to the current American Thyroid Association guidelines [15]. Preoperatively undiagnosed tumor foci in contralateral thyroid lobes can cause postoperative remnant disease. Remnant disease not only may lead to an additional surgery, but also can be associated with regional and distant metastasis. In this study, the size of primary largest tumor was not associated with the multifocal tumors or bilateral tumors. Instead, unilateral multifocal PTMCs (number of unilateral tumor foci ≥2) have more than 30% chance of bilateral PTMCs (Fig. 2). Similarly, several studies have observed a higher rate of the contralateral tumors when multifocal disease is present in the ipsilateral lobe [16,17,18]. For unilateral multifocal PTMCs, the extent of surgery is still not determined clearly [15,19]. Although the prognosis of PTMCs is excellent [20,21], we suggest total thyroidectomy for preoperatively diagnosed multifocal PTMCs and completion thyroidectomy for multifocal PTMCs incidentally diagnosed after lobectomy, because of the high probability of contralateral tumor foci and the poor prognosis of multifocal PTCs. Though lobectomy alone may be performed, thorough and meticulous follow-up is necessary for those multifocal cases.
Additional to low sensitivity of preoperative radiologic tests for multifocal PTMCs and their undetermined prognostic significance, the predictors for those multifocal PTMCs are presently unknown. In this study, nodular hyperplasia was the only significant factor for multifocal PTMCs (Table 4), which is a novel finding to the best of our knowledge. As shown in Fig. 2, number of tumors in dominant lobe was the most significant clinicopathological predictor for bilateral PTMCs (P=0.038; Exp (B)=1.688) (Table 4). Well-verified predictive factors for multifocal PTMCs can decrease the risk of second operations.
In conclusion, in this study including 277 PTMC patients who underwent total thyroidectomy, the incidence of multifocal PTMC was 36.1%. The sensitivity of radiologic tests for multifocal and bilateral tumors were low (42.7% and 49.0%, retrospectively). The size of a primary PTMC was not associated with multifocality or bilaterality. In cases with multifocal tumors in the unilateral lobe, there were high chances of bilateral tumors. For which cases, more extensive surgery or more thorough follow-up may be warranted. Nodular hyperplasia was the meaningful predictor for both multifocality and bilaterality of PTMCs.
 XML Download
XML Download