

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Idiopathic sudden sensorineural hearing loss (ISSNHL), defined as a greater than 30 dB sensorineural hearing loss occurring in at least three contiguous audiometric frequencies over 72 hours or less (1) is a disease with unknown etiology. This hearing loss leads to permanent morbidity. Available treatments include corticosteroid, vasodilator, immunosuppressant and antiviral medications, although controversies do still exist. To date, corticosteroids are the most widely accepted, but there are no worldwide standard practice guidelines accepted for the treatment of ISSNHL (2). Various regimens of corticosteroid therapy are available, including various types, dosages, and administration routes. A high dosage of oral and intravenous corticosteroids is believed to revive hearing impairment. Oral corticosteroids are currently as administered following a tapered course over a period of 10 to 14 days (3). Nevertheless, therapy outcomes can not be considered satisfactory, as only 61% of patients are experience recovery (4). Intratympanic corticosteroid injections have been widely used to deliver corticosteroids directly into the inner ear for those whom systemic steroids have not been successful. Complications such as perforations of the tympanic membrane, myringitis and otitis media have been reported.
Hyperbaric oxygen therapy (HBOT) has been shown to provide a significant additional effect when used in combination with a steroid therapy for ISSNHL (5). Outcomes of ISSHNL are significantly improved in the combined therapy of HBOT with conventional treatment modalities (6). This case report describes a patient who experienced full recovery following HBOT, after an unsuccessful treatment attempt with oral and intratympanic corticosteroids.
CASE REPORT
Clinical presentation
A Thai 37-year-old man presented at Burapha University with a sudden bilateral progressive hearing loss. He had a known case of hypertension, well-controlled with amlodipine. He suddenly lost his left hearing and experienced tinnitus and aural fullness. A high dose of steroids (prednisolone, 60 mg/day) was administered by the first physician. He subsequently developed a right hearing loss without left ear improvement and was referred to the first author. He had no history of either otitis media or any ototoxic medication. His blood pressure was 145/85 mmHg. Ear examination was unremarkable. Weber testing with a 512 Hz tuning fork showed no hearing response by the patient in both ears. He was diagnosed as bilateral progressive ISSNHL. Magnetic resonance imaging of the brain and the cerebropontine angle was unremarkable. Venereal disease research laboratory (VDRL), treponema pallidium hemagglutination (TPHA), and anti-human immunodeficiency virus (HIV) were non-reactive. Complete blood count found no leukocytosis and no anemia. Fasting blood sugar was 95 mg/dL.
Standard treatment
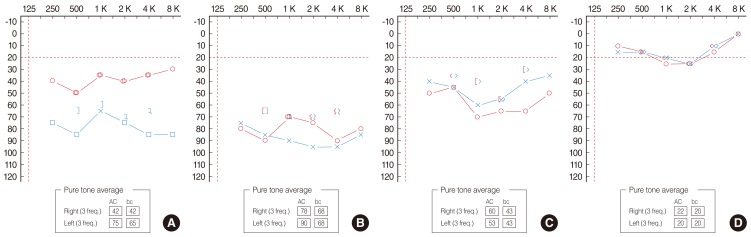
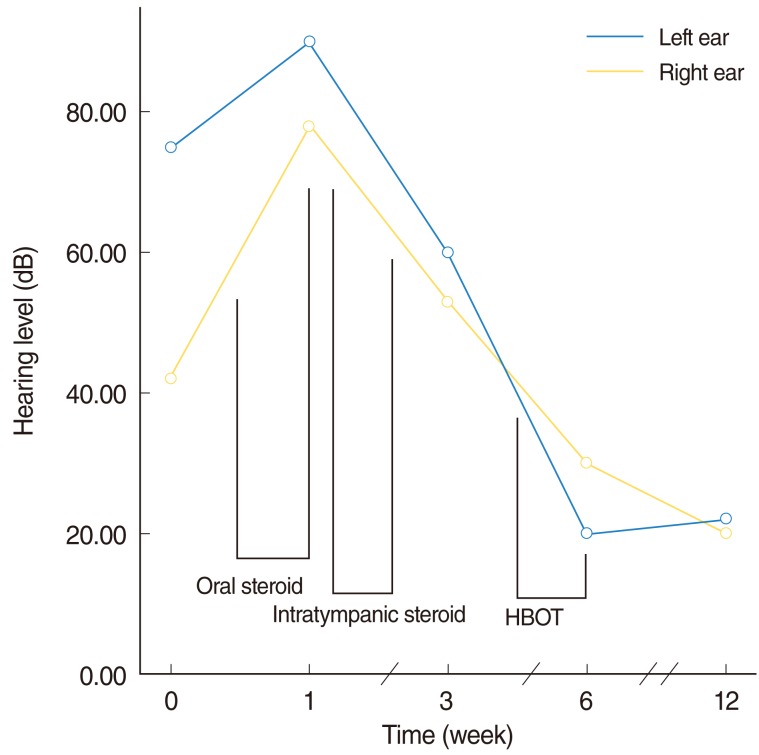
A high dose of oral steroid treatment (prednisolone, 60 mg/day) was administered by the first physician 3 days after the onset of the hearing loss. Audiogram was repeated after a week of standard treatment. The audiogram revealed right profound sensorineural hearing loss with a threshold of 78 dB and left deafness with a threshold of 90 dB. Administration of systemic steroids was then discontinued.
Salvage treatment
Intratympanic membrane steroids (methylprednisolone, 40 mg/mL) were administered in the left ear 3 times within a week (at day 9, 10, 16 after the onset). The hearing level after the third dose showed minimal improvement for both ears. The air conductive thresholds were 60 dB and 53 dB for the right and left ears, respectively. The bone conductive threshold was 43 dB for both ears.
HBOT
As HBOT is not yet standard for sudden sensorineural hearing loss, it was introduced to this patient as an alternative therapy. With no further improvement after the last audiogram (day 16), the patient decided to undergo HBOT (day 36) for a salvage treatment after a discussion with the authors.
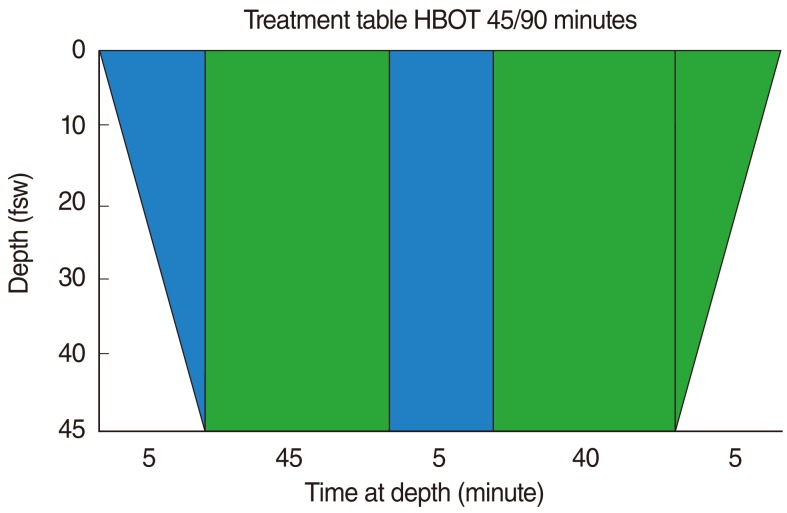
The HBOT program was scheduled for 10 sessions according to the US Navy treatment table (2 ATA 90 minutes) (Fig. 1). We used a 6-seat multi place chamber for the HBOT (Figs. 2 and 3), which was started at day 36 after the hearing loss onset. After the third session of HBOT (day 38), normal hearing returned, with no tinnitus in both ears. The following audiogram revealed normal hearing with a right threshold of 20 dB and a left threshold of 30 dB. Tinnitus was evaluated to be resolved by the visual analog scale. The patient was sent for the 4th (day 41) and the 5th sessions (day 42) as scheduled. The following audiogram 3 months after the entire treatment showed normal hearing level with a right threshold of 22 dB and a left threshold of 20 dB.
DISCUSSION
To date, the awareness of HBOT as treatment for ISSNHL is low in Thailand. Whereas Navy hospitals and a few private hospitals have been equipped with a hyperbaric chamber, only a small number of medical schools is planning for installation of HBOT facilities. Effective communication between doctors and patient is required. Patients have the right to know both the risks and benefits of the treatment, particularly when non-standard alternative treatment options are available and if they are of the first cases in the country. In addition, the criteria of salvage treatments should be discussed in terms of time course and hearing levels. In this case, the authors started HBOT at the fifth week (day 36) after the onset of hearing loss. At this stage, spontaneous improvement is no longer expected, as the process of inflammation usually does not last beyond 2 to 3 weeks. Although the administration of intratympanic steroids (last dose given at day 16) offered some benenfit, as demonstrated by the improved audiometry, additional improvement after day 36 was not expected. Bilateral moderate hearing loss is the other aspect in which patients may experience more benefit than harm from the salvage treatment.
Although we cannot ascertain the causes of hearing loss, it may be related to a lack of oxygen secondary to a vascular problem not yet identified. HBOT involves breathing in pure oxygen from a specially designed chamber. This method is used to increase the supply of oxygen to the ear and the brain to reduce the severity of a hearing loss and tinnitus (7). The HBOT in this case resulted in full recovery of the hearing thresholds without tinnitus or any complications. Others studies have demonstrated comparable outcomes of HBOT, supporting the results of our case report. Patients who received HBOT in conjunction with corticosteroids presented with enhanced clinical outcomes compared to those receiving only corticosteroids in the study by Fujimura et al. (5).
The standard regimen of HBOT for treating ISSNHL is yet to be defined. Our initial plan was to apply the treatment table 45/90 (2 ATA 90 minutes) for 10 sessions. But when the patient demonstrated returned normal hearing with no tinnitus in both ears during the third and the fifth session of HBOT, the last five sessions were believed to be unnecessary and eventually canceled. The other regimen proposed by Topuz et al. (6), which involvesundertaking HBOT 2.5 ATA for 90 minutes twice daily for the first five days and then once daily for the next fifteen days, also demonstrated good results. Patients over 50 years of age having a severe sensorineural hearing loss greater than 60 dB and receiving HBOT without delay experienced a higher rate of recovery.
Although we know that HBOT promotes oxygenation to the target tissue, its exact mechanism of action is undefined. As for ISSNHL, the inner ear apparatus and hearing ability may be revived by this mechanism. Further investigation is warranted, including animal studies to understand the molecular and histopathological aspects of HBOT and randomized control clinical studies.
In conclusion, HBOT may be used for idiopathic sudden sensorineural hearing loss as an adjuvant therapy. It may promote oxygenation to the inner ear apparatus and revive hearing ability. Patients who fail to respond to oral and intratympanic steroids may benefit from this treatment. Further investigation is warranted, including animal studies to understand the molecular and histopathological aspects of HBOT and randomized control clinical studies.


 XML Download
XML Download