

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Laryngotracheal separation (LTS) is the most immediately life-threatening airway injury caused by any of various injuries to the neck including automobile accidents, attempted hanging, and direct blows to the anterior neck [1, 2].
Because LTS is very so rare, emergency physicians and otolaryngologists have limited experience with it and there is no consensus on its management [2]. Therefore, LTS is a diagnostic and therapeutic challenge in airway injuries. A high index of suspicion and immediate reconstruction with restoration of the laryngotracheal framework and mucosal integrity enables patients to recover a patent airway, functional voice, and normal swallowing.
We report a case of complete LTS and review the relevant medical literature.
CASE REPORT
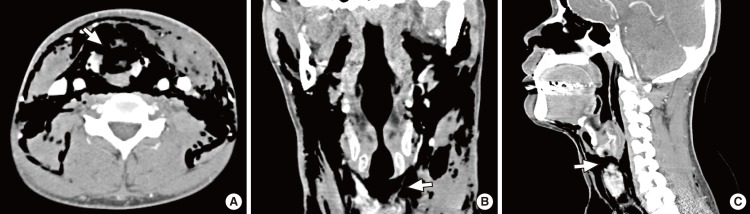
A 37-year-old man was transferred to the emergency room. The patient had attempted to hang himself from a height of three stories and was immediately rescued by an eyewitness. On arrival, the patient was fully conscious and had no neurologic impairment. The patient had a hoarse voice but no other symptoms or signs of airway distress. Transverse linear abrasion by a clothes-line was visible on the anterior aspect of the neck at the location of the larynx, and subcutaneous emphysema without any penetrating wounds of the skin was detectible by palpation over an extensive area of the neck and upper chest wall. Cervical and chest X-rays revealed cervical and upper thoracic emphysema but no other abnormality. Multi-detector computed tomography (MDCT) including multiplanar reconstruction images revealed a complete laryngotracheal separation without fractures of the thyroid and cricoid cartilage. These findings were observed most clearly in the sagittal reconstruction images (Fig. 1).
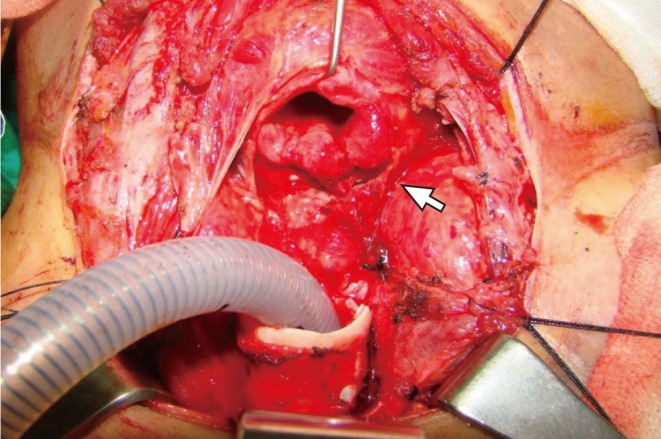
During flexible laryngoscopy for evaluating the upper aerodigestive tract, dyspnea concomitant with cough occurred suddenly and the patient became cyanotic. Tracheotomy at the suspected site of separation was performed urgently, after which the patient was transferred to the operating room. The neck was explored through a transverse incision formed by extending a tracheotomy incision laterally. The patient had complete transection between the cricoid cartilage and the first tracheal ring, and stretching of the left recurrent laryngeal nerve was observed (Fig. 2). However, the thyroid cartilage, cricoid cartilage, esophagus, and great vessels were intact.
Before anastomosis, an endotracheal tube intubated through the tracheostomy was removed and then was reintubated transorally. Release techniques such as suprahyoid release were not used in this patient because of the absence of tracheal cartilage loss. Right side tracheal wall was dissected to avoid damage to the right recurrent laryngeal nerve with great care because stretching injury of left recurrent laryngeal nerve was suspected strongly.
Neck extension was eliminated with removal of shoulder roll and the trachea was anastomosed to the cricoid cartilage using interrupted 4-0 Vicryl sutures. The sutures began in the posterior midline and proceeded laterally in a symmetric fashion. Each suture was passed from extraluminal side to intraluminal side submucosally, with the knot placed extraluminally to minimize the risk of infection, granuloma, and stricture formation.
Following complete closure, the wound was flooded with saline and a Valsalva maneuver was performed after the deflation of the cuff of the endotracheal tube to assure an air-tight closure. The strap muscles were re-approximated in the midline over suction drains, followed by closure of the platysma and skin. To lessen the tension over anastomosis in the postoperative period, the head was kept in flextion position with a nylon suture from the chin to the anterior chest wall.
The endotracheal tube was removed on day 3 in the intensive care unit, and left vocal cord paralysis was observed upon flexible laryngoscopy. The remaining postoperative period was uneventful. Neck computed tomography (CT) scan taken at 10 days after the operation demonstrated complete resolution of subcutaneous emphysema and appropriate reconstruction of laryngotrachea (Fig. 3). The patient was discharged 2 weeks later without a tracheostomy and was lost to follow-up.
DISCUSSION
Airway trauma may be life-threatening, immediately or within several hours after acute injury. Although laryngotracheal injuries represent less than 1% of all traumatic injuries, they account for more than 75% of immediate mortality [3]. Motor vehicle accidents are the most common cause of blunt trauma to the airway, with hanging as a method of attempting suicide increasing in incidence [3, 4]. Laryngeal injuries were observed in 35% to 45% of victims of hanging at autopsy [5]. Because laryngotracheal separation caused by hanging usually results in early death at the scene, the true incidence is unknown [2, 3, 5].
Typical LTS occurs with clothes-line type injuries, as in the present case. Sudden neck extension, fixation of the larynx, and anteroposterior compression of tracheal rings creates shearing forces tearing the cricotracheal membrane. Direct upward pressure by hanging elevates the larynx superiorly and, as a result, larynx, and trachea are separated [6].
Admitted patients with laryngotracheal injury exhibit characteristic signs including hoarseness, dyspnea, subcutaneous crepitus, and skin abrasions over the anterior neck, but their presence vary according to the degree and extent of injury [1].
Respiratory distress may be absent, as in the present case, if the separation between the cricoid cartilage and the ends of trachea is not large, allowing adjacent soft tissue around the trachea to form a pseudo-airway and make ventilation possible. Sudden airway obstruction may occur by trial of endotracheal intubation, neck extension or coughing [2, 5, 7].
Fiberoptic laryngoscopy of the upper airway may be helpful for evaluating the site and extent of injury. However, in the case of highly suspected LTS, fiberoptic laryngoscopy should be performed cautiously and with the preparation of a tracheotomy. Irritation by instrumentation may induce effortful cough and disrupt this unstable airway, resulting in abrupt dyspnea.
CT can provide important information regarding the laryngotracheal skeleton and soft tissue integrity. Cephalocaudal separation between cricoid and trachea, abrupt change in position, diameter, and shape of the airway and an extraluminal position of the distal endotracheal tube are the suggestive CT findings of LTS [8]. As shown in this case, sagittal reconstructive image may be useful to evaluate the integrity of laryngotrachea.
Initial management should ensure an adequate airway. Tracheotomy is recommended as the method of choice to secure the airway by many authors, because endotracheal intubation may pass into a false track at the site of tracheal separation and obstruct the airway completely [2, 4, 9]. Cricothyroidotomy is not recommended after blunt laryngotracheal injuries, as this may further injure the laryngotrachea [2]. Tracheotomy at the suspected site of separation may be performed rapidly without further tracheal cartilage injury, as in the present case. After airway is secured, definite surgical repair should be considered as early as possible. Early repair within 48 hours shows improved outcomes with respect to airway and voice and also lower incidence of subglottic stenosis [10, 11].
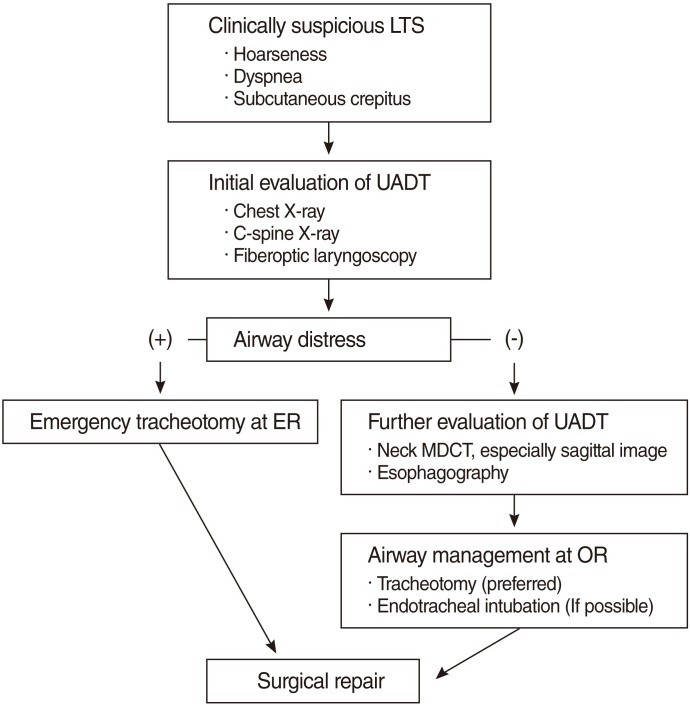
In conclusion, a high index of suspicion, adequate imaging, prompt airway establishment, and early surgical repair are the most vital factors in managing the patient with LTS (Fig. 4).

 XML Download
XML Download