

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Sinonasal malignancies involving the anterior skull base (ASB) are challenging due to the complex anatomy and important structures that may be involved (1). Many surgical techniques for approaching this area have been developed for complete resection of these tumors. Since Ketcham (2) first described the combined transcranial and transfacial approach, the craniofacial resection has been the standard surgical approach to sinonasal malignancies involving the anterior skull base. However, a new technique is needed because of the high rate of surgical complications and morbidity associated with the current approach (3, 4). In 1997, Yuen et al. (5) first described an endoscopic technique for the resection of an olfactory neuroblastoma (ONB) involving the ethmoid sinus and cribriform plate. They used the term "cranionasal resection" to distinguish it from a "craniofacial resection". Since then, many articles on endoscopic resection have been published internationally (6-9). However, because of the rarity of sinonasal tumors involving the anterior skull base, a long term follow-up study on a large number of cases has not been carried out in Korea (10).
We retrospectively reviewed 46 patients diagnosed with sinonasal tumors. The clinical features were analyzed and the surgical complications and morbidity were compared according to the surgical technique used, which included the traditional craniofacial resection (TCFR) or the endoscopic craniofacial resection with craniotomy (ECFR) (11).
MATERIALS AND METHODS
A retrospective chart review was performed on 46 patients who were diagnosed with sinonasal tumors with involvement of the ASB that underwent craniofacial resection between January 1989 through December 2006 at the Seoul National University Hospital and Bundang Hospital. The patient records were reviewed for demographic data, clinical presentation, operative procedures, postoperative course, histopathological findings, immediate/delayed complications, morbidity and mortality. Twenty-four patients were male and 22 patients were female. The average age of the patients was 43 yr, with a range of 5 to 70 yr. The mean follow-up period was 31 months, with a range of 2 to 202 months. The preoperative evaluation consisted of sinonasal endoscopy, CT/MR scans and screening for distant metastasis: bone/liver scans or positron emission tomography (PET). Patients who had resectable lesions with no systemic metastasis underwent surgery. Up until 1998, 18 cases of TCFR were performed; since 1999, in cases without involvement of the orbit, skin or facial bones, ECFR (10 cases) was performed; in patients with involvement, TCFR (18 cases) was performed. In cases with malignant tumors, ECFR was performed in 9 patients with ONB; for benign tumors, ECFR was performed in 1 case with a meningioma. Our Institutional Review Board approved the protocol for this retrospective analysis.
Endoscopic craniofacial resection with craniotomy
In all patients, CSF drainage was performed to minimize injury to the frontal lobes during the retraction. For large tumors where the origin could not be defined, the procedure began with margin clarification after tumor volume reduction with the use of a microdebrider. The incision had a minimum margin of 1 cm from the tumor attaching site. In cases where en bloc resection was feasible, intranasal structures were included in the extent of the resection after an accurate delineation of the tumor margin with the use of an endoscope. A safe margin around the tumor was ensured with a 1 cm incision. In the areas more apart from the tumor margin a frozen section biopsy was done around the region of the incision site. Then, subperiosteal dissection was performed to identify the nasal septum, skull base and orbit. In areas such as ethmoid sinus where the subperiosteal dissection was difficult, the microdebrider was first used to reduce the mass volume and then the mucosal dissection followed. For visualization, the septum was removed and the frontal or sphenoid sinus was opened. An osteotomy was created at the lesion and the tumor was delivered through the craniotomy site. A pericranial flap was used for reconstruction. No facial incision was made with this surgical technique in contrast to the TCFR.
Adjunctive treatment for ONB
Ten patients underwent TCFR, all were classified as Kadish type C. Among them, eight patients had postoperative radiotherapy, and chemotherapy was provided to one patient. In the nine patients that had ECFR, six (Kadish type A: 1, B: 1, C: 4 cases) underwent neoadjuvant chemotherapy and postoperative radiotherapy. Two patients (Kadish type C) had postoperative radiotherapy only. One patient with Kadish type C who showed partial remission after neoadjuvant chemotherapy, was reluctant to receive surgery, and had radiotherapy instead. However, there was no improvement after the radiotherapy, and finally surgery with chemotherapy was performed. The chemotherapy regimen consisted of etoposide (75 mg/m2/day, days 1-5), ifosfamide (1,000 mg/m2/day, days 1-5) and cisplatin (15 mg/m2/day, days 1-5). At first, two cycles of chemotherapy were administered and additional cycles were planned according to the response to the first two chemotherapy cycles.
The initial symptoms, tumor involvement and the histopathology were reviewed and the morbidity and complications were assessed according to the surgical technique. The Mann-Whitney U test and the Kaplan Meier method were used to identify the surgical outcomes and morbidity of the patients receiving the TCFR compared to those who had an ECFR. The data were analyzed using SPSS 12.0 for Windows (SPSS Inc., Chicago, IL, USA). P-values ≤0.05 were considered statistically significant.
RESULTS
Clinical features of the tumors
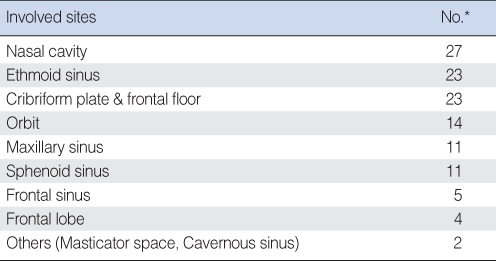
The patient presentation most commonly included a history of nasal obstruction and unilateral epistaxis. The average duration from symptom development to diagnosis was 4.3 months. The sites commonly involved included the nasal cavity, ethmoid sinus and cribriform plate. In addition, the sphenoid sinus, frontal lobe and cavernous sinus were also involved (Table 1).
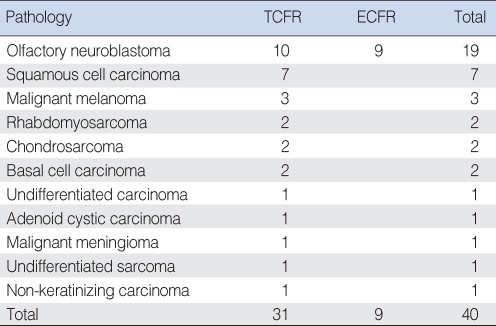
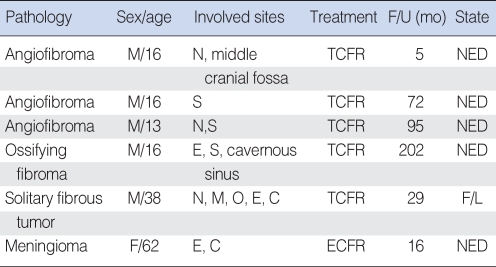
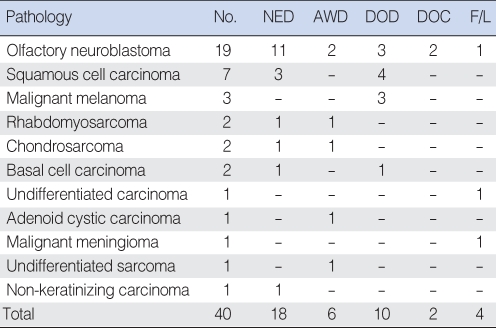
A list of the histopathological diagnoses is given in Table 2 and 3. The patients with benign tumors were followed with no evidence of disease except one patient with a solitary fibrous tumor that underwent malignant transformation (Table 3). For the 40 patients with a malignant tumor, 18 were followed with no evidence of disease, and the survival outcomes depended on the histopathological type of tumor (Table 4).
Treatment outcomes
Thirty-one patients out of 40 patients who were diagnosed with malignant tumors, underwent a TCFR, of which 17 patients (55%) developed disease recurrence; 11 had a local recurrence (35%), 4 had brain metastases (13%) and 2 had spinal metastases (6%). One patient (11%) out of 9 who underwent an ECFR had a local recurrence. For malignant tumors, the follow-up period ranged from 2 to 116 months, with a mean of 25.4 months. The overall 5-yr survival rate for the sinonasal tumors involving the anterior skull base was 47.4%.
Complications and morbidity
There were nine complications related to the surgery. Eight occurred after the TCFR, and 1 case of an epidural hematoma occurred after an ECFR. Complications related to the TCFR included CSF leakage, meningitis, hematoma, and flap necrosis at the facial incision site. Seven cases with complications were managed by surgery such as a craniotomy and wound revision; one patient expired due to complications and one patient had persistent facial paralysis. Another two patients with complications were treated with conservative antibiotic management.
A subset of the patients who underwent an ECFR was selected and compared to a group that underwent a TCFR. The groups were compared with respect to operation time, intraoperative blood loss, length of hospital stay and length of ICU stay. The ECFR group had a shortened length of stay and operation time; these differences were statistically significant (P-value: 0.016 and 0.002 respectively). With respect to the length of the ICU stay and the operation time, the differences did not reach statistical significance (P-value: 0.679 and 0.059 respectively) (Fig. 1).
Postoperative course
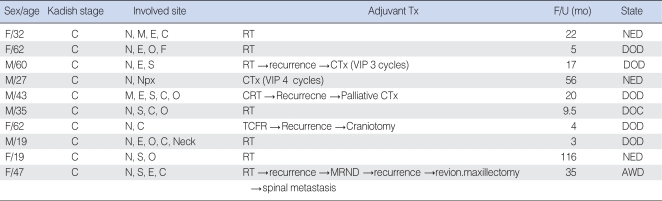
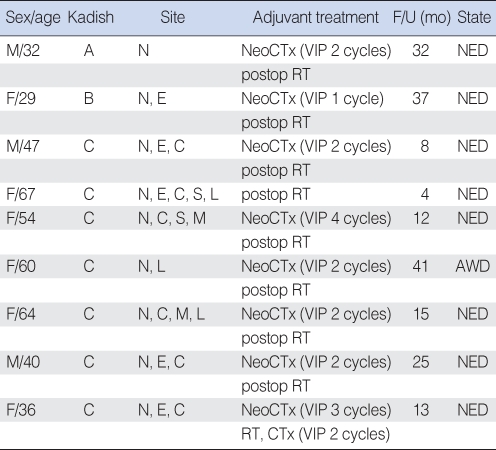
In 19 patients with ONB, 10 patients underwent a TCFR, while nine patients underwent an ECFR. For the patients with a TCFR, the mean follow-up period was 28.8±34.7 months and six of the 10 patients died of their disease (Table 5). For the patients who had an ECFR, the mean follow-up period was 20.7±13.4 months and all nine patients are still alive (Table 6).
DISCUSSION
The incidence of sinonasal cancer has been reported to be one in 100,000 per year; it accounts for approximately 3% of all the upper aerodigestive tract malignancies and less than 1% of all cancers (12). In particular, the incidence of tumors involving the anterior skull base is too low to analyze the demographic data and survival outcome according to the histopathological type. Squamous cell carcinomas and olfactory neuroblastomas are known to be the two most common malignancies followed by primary salivary gland tumors and sarcomas; our findings confirm this (13). ONB is known to have a good prognosis. Although several adjunctive treatments have been developed, surgery is considered to be the standard treatment and postoperative radiotherapy is recommended to improve the local control rate. The standard treatment may vary according to the histopathological type of tumor. However in many cases, there is no standard treatment established to date.
Previously, craniofacial resections were associated with a high rate morbidity and mortality related to the surgical technique (2, 14, 15). However, with progress in surgical methods and reconstruction approaches such as the pericranial flap, the complication rate has decreased dramatically (16-18). Recently, noninvasive surgical techniques have created a great deal of interest. The endoscope assisted CFR has been developed and can be used clinically. Endoscopic surgery has been used in rhinosinusitis surgery since the 1980s. As the knowledge and experience with endoscopic surgery has improved, and the image guidance systems and surgical instruments for endoscopic surgery have evolved, endoscopic surgery has been increasingly used for the treatment of benign tumors (19). As experience with benign tumor surgery accumulated, endoscopic surgery was adopted for the treatment of malignant tumors (5-9, 20). Buchmann et al. (1) reported that endoscopic instruments and techniques not only allowed excellent visualization of the tumor, but also greatly aided the accurate microscopic resection, resulting in good patient outcomes and reduced surgery related morbidity. In 2006, Paolo et al. (8) reported that the major exclusion criteria for an ECFR were as follows: 1) tumors involving the lacrimal tract, 2) tumor infiltration of the hard palate, 3) tumors that involve the posterior wall of the sphenoid sinus, and 4) tumor invasion of all but the medial wall of the maxillary sinus. However, the indications for an ECFR have not yet been established. The development of imaging diagnostic tools as well as adjuvant treatments has expanded the role of the ECFR. The development of imaging diagnostic tools has enabled early detection and accurate preoperative evaluation. In addition, neoadjuvant/adjuvant chemotherapy and radiotherapy has aided in improving treatment results (1, 21).
In our study, for the malignancies, ONB was the only histopathological type where the ECFR was used. This is due to the limitations of the endoscopic approach and the advent of adjuvant therapy for ONB. The endoscopic approach is limited in lesions involving the orbit, skin and facial bones. Consequently, an ONB, which is commonly located at the interface between the superior nasal cavity and the anterior cranial fossa, is a better indication for an ECFR than squamous cell carcinoma, which commonly occurs in the maxillary sinus and is invasive to adjacent structures. The ONB originates from neuroendocrine cells similar to small cell lung cancer, and small cell lung cancer is known to respond to chemotherapy agents such as cisplatin. There is one report that confirms that ONB is responsive to cisplatin (22). Therefore, at our institution, a combined modality treatment has been adopted, in which initial cisplatin based neoadjuvant chemotherapy (VIP) is provided to reduce the tumor volume and surgery is planned to minimize the functional and cosmetic deformities. In addition, in patients with Kadish type C disease, postoperative radiotherapy is recommended (21, 23, 24). The development of adjuvant therapy has supplemented the limitations of endoscopic resection and allows for a more expanded use of endoscopy with other histopathological tumor types.
The results of this study showed that the patients who had an ECFR had a tendency to have reduced morbidity and a good survival outcome. However, in most ECFR cases, neoadjuvant chemotherapy and postoperative radiotherapy were performed, and the follow-up period was relatively short, in contrast to the TCFR cases, where neoadjuvant chemotherapy was not usually performed. Therefore, further long term follow-up studies are needed to evaluate the outcomes of the ECFR compared to the TCFR with respect to oncological safety and survival.
In conclusion, the ECFR may have the advantages of reducing the surgery related morbidity and mortality compared to the TCFR. Therefore, it should be considered as an alternative treatment option for selected sinonasal tumors involving anterior skull base.

 XML Download
XML Download