

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Allogeneic corneal transplantation is important; it is very effective, it is the only treatment for blinding corneal disease, and it is a large part of global tissue transplantation [1]. However, several problems with this method have become apparent in past decades. The supply of donor corneas is much lower than the demand. Second, immune-mediated corneal allograft rejection is likely to develop with high-risk corneal transplantation, including an infectious recipient bed, refractory neovascularization, and limbal stem cell deficiency (LSCD). Although corneal transplantation has a high survival rate of 90% when performed in low-risk recipients [2], in cases of high-risk corneal transplantation, pathologies such as LSCD and autoimmune disease may lead to a poor surgical outcome including decreased visual acuity (VA) due to recurrent corneal opacification, neovascularization, and persistent epithelial defect (PED) with ulceration.
Deep anterior lamellar keratoplasty (DALK) is advantageous over penetrating keratoplasty (PK) because DALK eliminates the possibility of endothelium rejection and using lower-quality tissues [3,4]. However, there is still a possibility of epithelial and stromal rejections after DALK because of f resh corneal tissue cellular components, including the epithelium, keratocytes, and bone marrow-derived cells, which are sources of major histocompatibility complex antigens [5]. One way to overcome this limitation may be by decellularizing corneal substrates. Previous studies reported that glycerin cryopreservation was a practical and effective technique for decellularization [6]. Decellularizing corneal tissues could prevent an immune transplant rejection pathway because of the absence of antigen-presenting cells, which would reduce the amount of sensitization in the recipient's T cell levels. In this study, we used the VisionGraft (Tissue Banks International, Baltimore, MD, USA), a sterile gamma-irradiated acellular cornea that has recently been made available for use by ophthalmic surgeons.
Amniotic membrane transplantation (AMT) is a widely used method in ocular surface disease. AMT contributes to the restoration of an intact basement membrane, and supports facilitation of epithelialization [7]. Another beneficial effect of AMT is that it suppresses T cell proliferation, which can reduce immune-modulatory effects in intractable ocular surface disease [8]. Thus, AMT may play an important role in high-risk corneal transplantation by facilitating epithelialization and lowering immune rejection. In this paper, we report our experience with DALK in combination with AMT in a small group of intractable ocular surface disease cases, using sterile gamma-irradiated acellular corneal tissues.
Materials and Methods
We retrospectively reviewed the medical records of fifteen patients operated on at the Chung-Ang University Hospital between November 25, 2010 and October 19, 2012. The study protocol was in accordance with the Declaration of Helsinki and was approved by the institutional ethics committee of Chung-Ang University Hospital, Seoul, Korea. All participants gave informed consent after a detailed explanation of the study design, ancillary investigations for scientific purposes, and related imaging procedures.
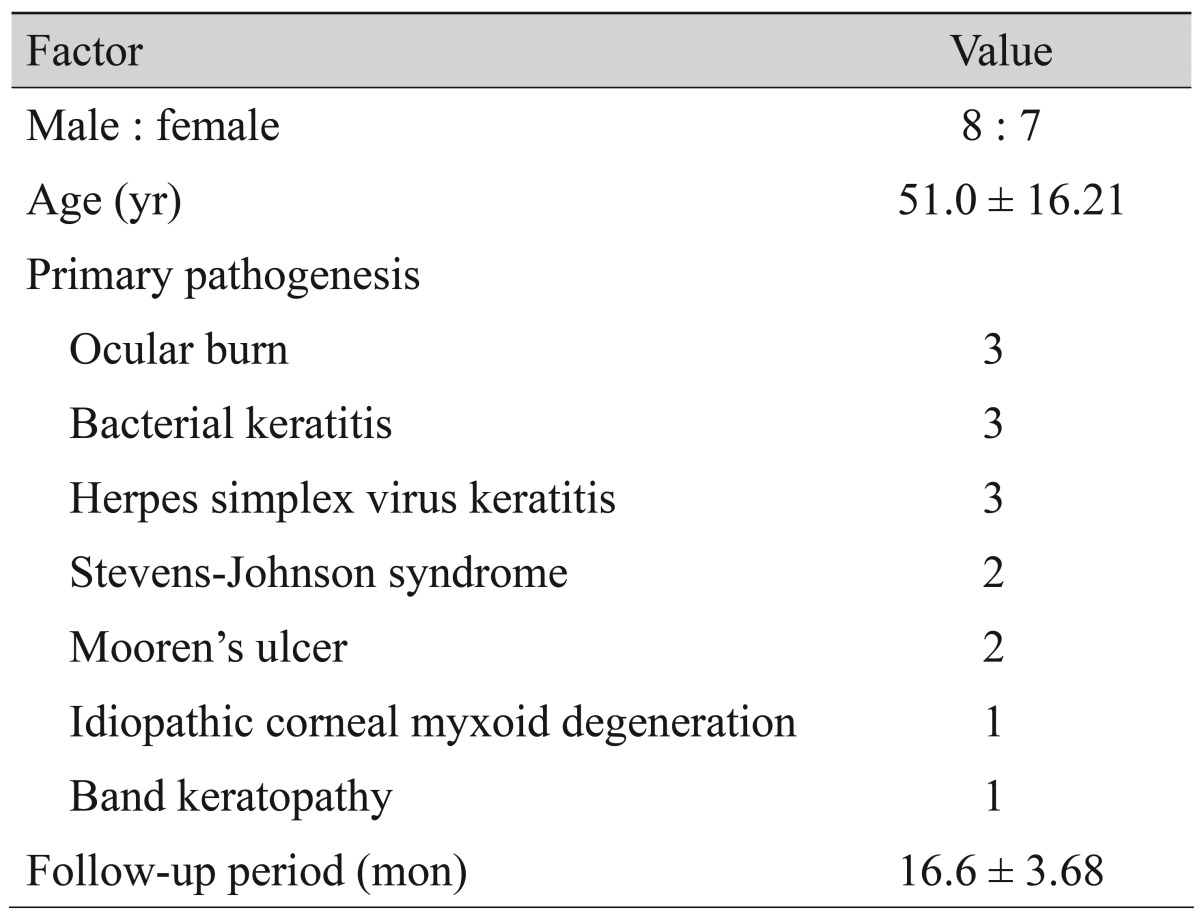
Indications for surgery included ocular burn (n = 3), bacterial keratitis (n = 3), herpes simplex virus keratitis (n = 3), corneal opacity with Stevens-Johnson syndrome (n = 2), Mooren's ulcer (n = 2), idiopathic myxoid degeneration of corneal stroma (n = 1), and recurrent band keratopathy (n = 1). The majority of the patients had a history of graft failure despite previous multiple PKs and ocular surface stabilization failure despite sole AMT, which resulted in corneal opacification, neovascularization, PED with ulceration, and infection.
All DALK procedures were performed by the same surgeon (JK) under retrobulbar anesthesia in a similar fashion using the modified big bubble technique [9]. The Hessburg-Barron disposable vacuum trephine (Katena Products, Denville, NJ, USA) was used and the host cornea was trephined to a level of 70% to 80% of its original thickness. The size of trephination ranged from 7.0 to 8.5 mm, and was 0.5 mm bigger than the size of the recipient bed. The air was injected into the deep stroma of the central cornea with a 30-gauge needle inserted on a 2-mL syringe with the bevel facing down. This procedure formed a large bubble between the Descemet's membrane and stroma, and separated the Descemet's membrane. Air injection was stopped when the big-bubble reached the trephination line. Air was injected into the anterior chamber after incising the corneal limbus with a diamond blade. Then the anterior lamellar stroma (about 80% in thickness) was removed by a 360-degree lamellar dissection technique using Vanna scissors. The remaining anterior stromal fibrous tissue was removed with additional dissection using viscoelastic substance injection and repeated dissections until the Descemet's membrane was exposed. The host bed was irrigated to remove any remaining viscoelastic substance using a balanced salt solution (Alcon Laboratories, Fort Worth, TX, USA). The sterile acellular corneas were kept in sterile glass bottles and stored in albumin solution. The tissue consisted of a 350-µm partial thickness, clear, corneal lenticule without endothelium and Descemet's membrane. The sterile acellular cornea was sutured in place using 24 interrupted 10-0 nylon. Air was injected into the anterior chamber again to facilitate linkage between the host's Descemet's membrane and grafted corneal stroma.
At the end of the DALK operation, the temporary amniotic membrane patch was secured with interrupted 10-0 nylon sutures with episcleral bites in the stromal side up position which covered most of the ocular surface. Preserved human amniotic membrane (Amnisite; Bioland, Cheonan, Korea) was obtained from donors that were seronegative for the human immunodeficiency virus, human T cell leukemia virus, hepatitis B virus, hepatitis C virus, and syphilis at delivery. Also administered were subconjunctival injections of gentamicin and betamethasone.
Topical treatment, administering the third-generation fluoroquinolone (Cravit; Santen, Osaka, Japan) four times per day for 1 month and a 1% prednisolone acetate (Predforte; Allergan, Irvine, CA, USA) was administered four times daily for the first week and tapered over 3 months before being discontinued. Oral antibiotic treatment was prescribed for 2 weeks and oral steroid treatment was administered with a dose of 0.5 mg/kg/day and tapered over 3 weeks.
Temporary amniotic membrane patches were removed at postoperative 1 to 2 weeks, and corneal sutures were removed at the end of postoperative 3 to 12 months according to the state of the grafts. All patients were observed closely for inflammation, infection, graft rejection, epithelialization, and clarity. Immunologic stromal rejection was diagnosed clinically and determined by the presence of decreased vision and stromal edema with or without corneal neovascularization. Graft failure was defined as an irreversible loss of central graft clarity for a minimum of 3 consecutive months, and required additional PK. The residual acellular cornea was fixed with 10% formalin for 24 hours and stained with hematoxylin-eosin to verify the acellularity of the product.
Results
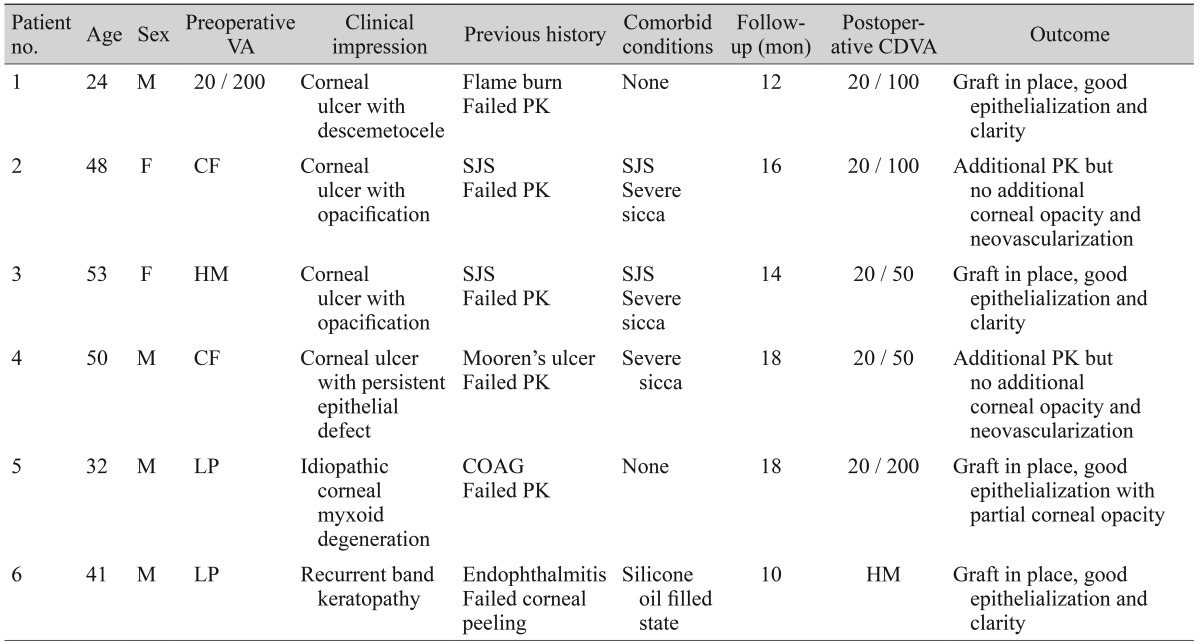
Patient demographics are summarized in Table 1. There were eight male and seven female patients, with a mean age of 51.0 ± 16.21 years (range, 19 to 78 years). The mean follow-up period was 16.6 ± 3.68 months (range, 10 to 24 months). Ten patients experienced multiple failed PKs even though fresh donor corneas were used. The multiple PK failures exhibited ocular surface stabilization failure with sole AMT, resulting in PED with corneal ulceration. These cases with failed PK and AMT had previous histories that included ocular burns, herpes simplex virus keratitis, Stevens-Johnson syndrome, Mooren's ulcer, and idiopathic corneal myxoid degeneration. Detailed demographic data, clinical characteristics, and postoperative outcomes of the representative six patients are summarized in Table 2.
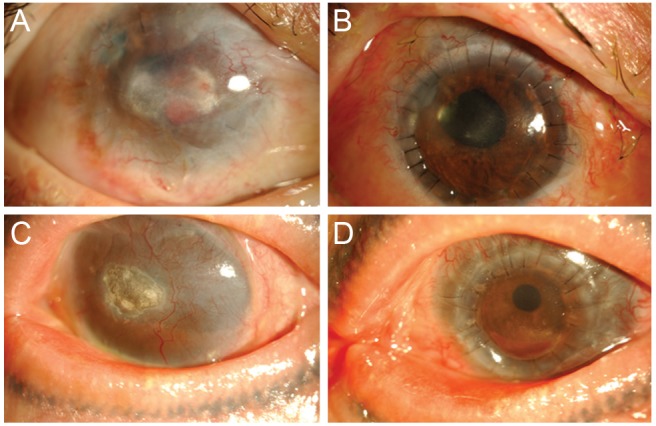
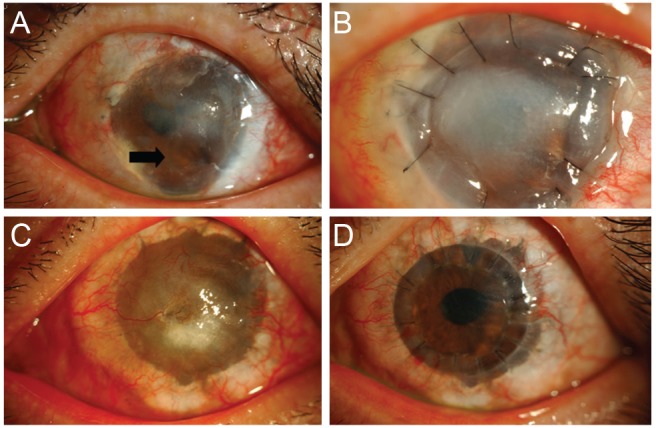
All cases that underwent DALK with AMT became epithelialized within 2 postoperative weeks. PED was not associated with corneal ulceration. Twelve patients showed favorable outcomes without graft rejection, corneal opacification, or neovascularization (Fig. 1). The other three patients developed corneal opacification, neovascularization, and eventually decreased VA, which required additional PK. These three cases had underlying comorbidities which included Stevens-Johnson syndrome and Mooren's ulcer. However, unlike the results of previous PKs, corneal opacification and neovascularization did not occur in these three patients during a follow-up period of 8 months (Fig. 2). No mechanical complication developed with the DALK procedure, including Descemet's membrane microperforation or pseudochamber formation.
Nine patients had preoperative VA that was worse than 20 / 200, and most of the cases showed postoperative VA that was less than 20 / 200 except two cases with hand movement VA.
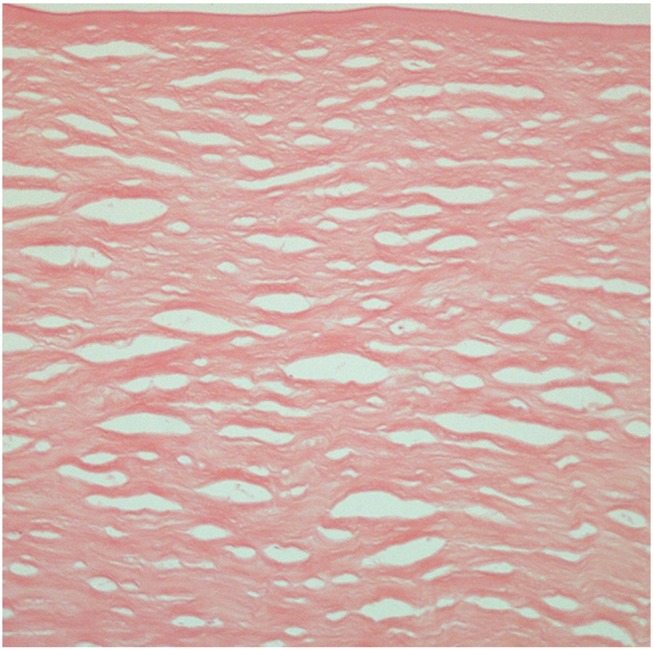
Hematoxylin-eosin staining of the sterile acellular cornea revealed a relatively loose corneal stroma with thinned epithelium that showed significant acellularity. There was no endothelium and Descemet's membrane beneath the stromal tissue in the product (Fig. 3).
Discussion
Fifteen patients with intractable ocular surface diseases were enrolled in this study. We used the sterile acellular cornea (VisionGraft) to perform DALK, this technique is advantageous because it applies decellularization to minimize the risk of allograft rejection, and has been associated with good clinical outcomes.
The sterile acellular cornea, which is irradiated human donor corneal tissue, is indicated for use in various corneal procedures that do not require a viable endothelium. Sterility is verified via periodic microbiology testing [10] and several previous small-group studies have used the sterile acellular cornea [10,11,12], which has several advantages compared with fresh donor cornea. First, gamma irradiation depletes antigen-presenting cells, thereby minimizing the risk of allograft rejection by preventing direct sensitization [13]. Additionally, this product can be stored at room temperature with a shelf life of 1 year, therefore it can be used in emergency procedures as well as scheduled operations.
Moller-Pedersen [14] and Moller-Pedersen [15] reported that corneal keratocytes support the stroma and presumably the stromal clarity, and are also involved in wound healing and collagen formation. According to a previous study, confocal microscopy confirmed that glycerin-cryopreserved corneas were acellular, while dendrite-like cells and keratocytes were found in the fresh cornea group 2 weeks after DALK. At 3 months after DALK, keratocyte density increased significantly in the glycerin-cryopreserved group, whereas it decreased significantly after surgery in the fresh cornea group [10]. Thus, in our study, like glycerin-cryopreserved corneas, keratocytes would repopularize and could help to maintain transparency of the transplanted cornea after DALK.
We combined AMT with DALK to prevent the possible complications of DALK, such as delayed epithelialization and inflammatory reaction. In this study, there were ten patients with multiple failed PKs and a sole AMT that resulted in PED with corneal ulceration. These patients had partial to complete LSCD because of accompanying ocular burn, herpes simplex virus keratitis, Stevens-Johnson syndrome, and Mooren's ulcer. The tendency of PED and corneal ulceration may contribute to grafted tissue failure, as in these cases. Therefore, we proposed that combining AMT with DALK could facilitate epithelialization of the corneal graft, and lead to a more favorable surgical outcome.
In a previous study [8], the amniotic membrane promoted rapid corneal healing in the majority of patients with PED. The epithelialization effect of the amniotic membrane is considered to be due to the restoration of an intact basement membrane. The basement membrane of the amniotic membrane is an ideal substrate to support the growth of epithelial progenitor cells by prolonging their life span and maintaining their clonogenicity [16,17]. This action may help facilitate epithelialization for PED with corneal ulceration. Even in partial LSCD, AMT was reported to produce a beneficial effect to restore the ocular surface in intractable diseases [18].
Another reason why the amniotic membrane supports a successful DALK is that the stromal side of the amniotic membrane contains a matrix component that has an antifibrotic effect. Several factors, including transforming growth factor β were down-regulated, and fibroblastic activation responsible for critical wound healing was also suppressed with AMT in a previous study [19]. Furthermore, the stromal matrix of the amniotic membrane can reduce the inflammatory response by regulating various growth factors [20]. AMT contributes to reducing the risk of graft failure by down-regulating fibrotic changes, scar formation, and immune-modulation with a lowered inflammatory response.
We combined AMT with DALK and used sterile acellular cornea; we observed good epithelialization in all fifteen patients. Considering that most of our cases had experienced multiple graft failures after PK and ocular surface stabilization failure with sole AMT, our procedure that combined AMT with DALK had a better outcome and facilitated epithelialization and down-regulation of fibroblast activation and immune rejection.
Three patients developed corneal opacification and neovascularization after DALK with AMT, resulting in additional PK; these patients had experienced multiple failed PKs before this procedure. However, unlike the results of previous PKs, there was no corneal opacification or neovascularization after the DALK and subsequent PK were performed. We hypothesize that DALK may contribute to ocular surface stabilization by reducing neovascularization and the infiltration of inflammatory cells, and thus DALK can be useful as a temporary measure before other reconstructive procedures including PK, to achieve better outcomes than just PK alone.
There have been studies about combining primary lamellar keratoplasty and a secondary optical PK in patients with high-risk corneal transplantation [21,22]. There are two main reasons for the prolonged survival of transplants when sterile acellular cornea is used for DALK. First, a sterile acellular cornea has lower immunogenicity and is less likely to induce an immune rejection. In a previous study [2], sterile acellular cornea derived from xenogeneic corneas had lower immunogenicity and a reduced ability to induce neovascularization and inflammatory cell infiltration than did fresh cat corneal lamellae. Second, DALK, using sterile acellular cornea, partially blocks both afferent and efferent corneal immune rejection and prolongs transplant survival. The collective data reinforce the view that DALK combined with an optical PK as a single-stage procedure may be a good therapeutic alternative with patients that experienced multiple failed PKs.
In this study, AMT with DALK, using sterile acellular cornea, showed more favorable outcomes in high-risk corneal transplantation cases. Therefore, this method could be used as an alternative choice to regular PKP, especially with patients that have a high risk of rejection. The main disadvantage of DALK is that it is technically more challenging and time-consuming compared with regular PKP [23]. If Descemet's membrane perforation occurs during DALK, it requires that 10% to 20% of keratoconus patients convert to PKP [24]. Additionally, until now, DALK has not been technically standardized. Therefore, it can be difficult DALK to apply with acellular cornea to replace regular PKP cases.
Our postoperative enrolled patients' outcomes should be compared with control group outcomes, such as patients undergoing sole DALK or AMT, to further elucidate the efficacy of combining AMT with DALK. However, the authors had a difficult time establishing the control groups because the patients enrolled in this study had high-risk corneas that had experienced multiple failed PKs and AMT. In addition, the small number of patients enrolled in this study and relatively short follow up period were limitations. In spite of these limitations, we identified that DALK with AMT may prove to be a good therapeutic option in intractable ocular surface diseases with multiple failed PKs and ocular surface stabilization failure with sole AMT. This study also found that this method could possibly decrease the rejection risk of corneal transplantation.
In conclusion, DALK, using sterile gamma-irradiated corneal tissues, in combination with AMT may be considered as a good therapeutic strategy in intractable ocular surface diseases, because of lowered immune rejection, fibroblast activation, and the facilitation of epithelialization. Additionally, DALK preceding PK can help stabilize the ocular surface and prolong graft survival by lowered immunogenicity, and reduce induction of neovascularization and inflammation. Therefore these results indicate that more favorable outcomes could be achieved if DALK is combined with subsequent PK.
 XML Download
XML Download