

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Giant cell arteritis (GCA), or temporal arteritis, is a vasculitis of medium-to-large-sized arteries that is confirmed with temporal artery biopsy. In GCA, the arterial walls are infiltrated with inflammatory cells such as lymphocytes, epithelioid histiocytes (giant cells), macrophages and fibroblasts. Ophthalmic involvement can occur in up to 50% to 70% of the GCA patients, and this represents an ocular emergency [1,2]. Arteritic anterior ischemic optic neuropathy (AAION) is the most common type of ophthalmic involvement in GCA and can cause permanent visual loss. Therefore, prompt diagnosis and treatment with a high dose of steroids is essential for these patients.
Patients with GCA typically present with headache, jaw claudication, fever, weight loss, myalgia, arthralgia, or malaise [1]. Conversely, patients with silent GCA, first described by Simmons and Cogan [3], present with sudden visual loss without systemic symptoms and signs. Thus, due to the lack of symptoms, diagnosis and treatment of silent GCA may be considerably delayed when compared to typical GCA [4]. An elevated erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) level and platelet count can serve as sensitive indicators in the diagnosis of silent GCA [2]. There have only been a few reports of silent GCA patients in Asia [5,6], and no reports on patients with GCA-accompanied AAION in Korea. Here, we report a case of silent GCA in an elderly Korean woman, as confirmed by temporal artery biopsy.
Case Report
An 83-year-old woman presented with sudden visual loss that had developed in both eyes (oculus uterque, OU) the previous day. Her past medical history was unremarkable. She did not complain of any associated headache, scalp tenderness, jaw claudication or constitutional symptoms such as weight loss, fever, malaise or sweats. Her visual acuities included perception of light in the right eye (oculus dexter, OD) and perception of hand motion in the left eye (oculus sinister, OS). The anterior segment examination revealed advanced nuclear sclerosis OU. A relative afferent pupillary defect OD was detected. Fundus examination revealed mild retinal arterial narrowing and chalky-white disc swelling OU (Fig. 1). The results of the Hardy-Rand-Rittler test and Ishihara test showed total dyschromatopsia OU. The Goldmann perimetry test revealed a total field defect OD and paracentral island OS. Although electroretinography findings were within normal limits, visual evoked potentials showed delayed P100 latency OU. Cerebrospinal fluid tapping revealed normal intracranial pressure and cell counts. Brain magnetic resonance imaging scans and angiography results showed diffuse bilateral stenosis of vertebral arteries and external carotid arteries without significant intracranial vessels stenosis. The CRP level, ESR and platelet count were elevated and measured to be 5 mg/dL (upper normal limit, 0.5 mg/dL), 55 mm/h (upper normal limit, 20 mm/h), and 510 K/µL (upper normal limit, 400 K/µL), respectively.
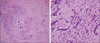
Following a presumptive diagnosis of silent GCA-associated AAION OU, the patient was hospitalized and treated with intravenous 250 mg methylprednisolone every 6 hours for 3 days. Biopsy of the left temporal artery was performed, and 3 cm of the temporal artery was acquired. Lymphocytes, epithelioid histiocytes, and multinucleated giant cells had diffusely infiltrated into the entire vessel wall, especially in the arterial wall media (Fig. 2). GCA was confirmed, and a high dose of steroid therapy was maintained.
After 7 days, the patient's visual acuity OS improved slightly to being able to count fingers. Disc swelling OU had decreased. The CRP level and ESR decreased to 1.07 mg/dL and 30 mm/h, respectively. Oral prednisolone therapy was slowly tapered down from 60 mg per day, and steroid treatment was maintained with deflazacort 30 mg per day. However, after 4 months, the patient's visual acuities deteriorated to no light perception OD and light perception OS.
Discussion
GCA predominantly affects elderly Caucasian females. GCA should be strongly suspected when patients greater than 50 years of age present with headaches. The incidence of GCA in Scandivian countries and North America ranges between 6.9 and 32.8 per 100,000 [7]. However, the occurrence of GCA is rare in African Americans, Hispanics, and Asians [8-10]. There have only been a few reports of GCA among Asians [5,6,11-15]. In Japan, a nationwide GCA survey revealed an extremely low prevalence of 1.47 per 100,000 population, which is approximately 1 / 140 of that reported in the US [10]. Pereira et al. [16] reported that GCA was seen 20 times less frequently in Asians than in Caucasians. Chaudhry et al. [17] stated that, for over a period of 22 years, only 7 patients were diagnosed with GCA by temporal artery biopsy in a tertiary medical center in Saudi Arabia.
The incidence of GCA in Asians was far lower than that in Caucasians; however, the incidence is now increasing in the Asian population. After 36 years of no reported cases of GCA, in 2010, Aui-Aree et al. [6] reported 4 GCA cases in Thailand. Cullen et al. [5] noted that of the 7 biopsy-confirmed GCA cases reported over the past 10 years in Singapore, 3 were reported in 2009. This trend may be associated with an increase in the maximum life span of the Asian population [7]. Suspected diagnosis of GCA by rheumatologists and ophthalmologists, along with extensive laboratory tests, may be other important factors. However, a nation-wide epidemiologic study would be needed to clarify the association of life span and GCA incidence in Asians.
In Korea, only a few biopsy-confirmed GCA cases have been reported [18,19]; however, there have been no GCA-associated AAION cases so far. To our knowledge, this is the first biopsy-confirmed report of GCA-associated AAION in Korea. Our patient was diagnosed with silent GCA, and the clinical features overlapped with non-arteritic AION. When Asian patients aged >50 years present with acute visual loss and disc swelling and no other symptom, non-arteritic AION accounts for more than 90% of these cases. In such circumstances, laboratory parameters, such as ESR, CRP level and platelet count can serve as indicators in the diagnosis of GCA. Hayreh et al. [20] reported that the CRP level has a sensitivity of 100% for GCA, and the combination of CRP level and ESR has a specificity of 97%. In a large population-based cross-sectional study, Walvick et al. [21] documented that the odds of a positive biopsy were 1.5 times greater with an ESR of 47 to 100 mm/h, 5.3 times greater with a CRP of >2.45 mg/dL, and 4.2 times greater with a platelet count of >400,000 µL. The above 3 parameters were elevated in our patient (CRP, 5 mg/dL; ESR, 55 mm/h; and platelet count, 510 K/µL). These test results are known to be normal in non-arteritic AION.
In conclusion, although this disease is rare in Asians, GCA-associated AAION should be considered when an elderly patient presents with sudden visual loss and disc edema. GCA should be suspected and laboratory tests should be performed, even in the absence of typical symptoms.

 XML Download
XML Download