

 PDF
PDF ePub
ePub Citation
Citation Print
Print


In 1896 in Germany, a man named Kuttner [1] first described the Kuttner tumor (KT), one of the common diseases involving the submandibular salivary glands, also known as chronic sclerosing sialadenitis. The tumor occurs mainly in the submandibular glands and appears as a firm and painless swelling mass. Clinically, KT is similar to a salivary gland neoplasm, which makes correct diagnosis difficult [2]. Histopathologically, KT shows the characteristics of chronic sclerosing sialadenitis, including progressive periductal sclerosis and dilated ducts with a dense lymphocyte infiltration and lymphoid follicle formations. The histopathology suggests that KT is closely related to an active local immune response [3,4]. Recent papers have presented a number of sclerosing diseases having abundant immunoglobulin G4 (IgG4)-positive plasma cells and sharing similar pathologic features with autoimmune sclerosing pancreatitis. KT is also classified under the category of IgG4-related sclerosing disease [5]. Additionally, a study by Cheuk et al. [6] has suggested that chronic sclerosing dacryoadenitis might be a part of the spectrum of IgG4-related sclerosing disease, as is chronic sclerosing sialadenitis. Regardless, most reported cases of IgG4-related sclerosing sialadenitis or dacryoadenitis show single organ involvement, except for a few case reports [6-9]. To the best of our knowledge, the present report is the first case of an unusual presentation of IgG4-related sclerosing disease involving bilateral lacrimal and submandibular glands, as well as extraocular muscles simultaneously.
Case Report
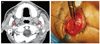
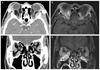
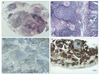
A 56-year-old male complained of mild intermittent diplopia. He also had swelling in both eyelids and proptosis that started 2 years ago, but he had not taken any special treatment (Fig. 1). He did not experience any symptoms of dry eyes or dry mouth. Exophthalmometric measurements were 21 mm in the right eye and 19 mm in the left eye. No limitation of motion was found in all extraocular muscles. His visual acuity, intraocular pressure, and fundus exams were normal. In his past medical history confirmed by his electronic medical records, both submandibular glands were enlarged five years ago. A fine needle aspiration biopsy done by an otolaryngologist revealed atypical lymphoid hyperplasia and periductal fibrosis, similar to sclerosing sialadenitis, but insufficient to diagnose KT (Fig. 2A). Despite not receiving any special treatment, currently there have been no definite changes of signs. Thyroid function and antinuclear antibody test scores were within normal limits. The level of serum IgG was elevated to 2,770 mg/dL. Other serum levels of immunoglobulins, including IgA and IgM, were normal. Orbital computed tomography (CT) and magnetic resonance imaging (MRI) demonstrated bilateral lacrimal gland enlargement and thickening of extraocular muscles, including the right inferior rectus muscle and both lateral rectus muscles, with homogeneous enhancement (Fig. 3). Orbital lymphoma was highly suspected, so incisional biopsy of the right lacrimal mass was done (Fig. 2B).
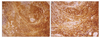
Light microscopic examination of tissue stained with hematoxylin and eosin showed dense lymphocyte hyperplasia and lymphoid follicles. In the center of the hyperplastic lymphoid follicles, atrophic lacrimal ducts and periductal sclerosis with an onion-skin appearance around the ducts were observed. An atherosclerotic vascular change was also observed in the mass. Application of immunohistochemial stains revealed that the hyperplastic lymphoid tissues were composed of polyclonal lymphoid cells, positive for CD 20 and CD 79a in the center of the follicle, and positive for CD 3 and CD45RO around the follicles. This indicates reactive lymphoid tissue without malignant process (Fig. 4). Immunostaining for IgG4 also revealed numerous IgG4-positive plasma cells (Fig. 5). The possibility of malignant lymphoma, including extranodal marginal zone B-cell lymphoma (MALT lymphoma), was ruled out. In light of overall clinical characteristics, together with histological and immunohistochmical results, KT was determined to be a reasonable diagnosis.
The patient was administered oral prednisolone 30 mg/day for 1 week with a dose taper over the course of 3 weeks. The size of the orbital lesion and submandibular gland started to decrease slowly and the intermittent diplopia disappeared. Four months later, however, the disease recurred with upper eyelid swelling. Systemic steroid therapy was restarted with a dose of oral prednisolone 1 mg/kg/day, which was gradually tapered over the course of four months. This disease showed good steroid response, but tended to recur after steroid medication stopped. A third attack of the disease appeared 8 months after the last steroid treatment. Again the patient took high-dose systemic steroid medication, and after completion of the steroid-tapering schedule was administered azathioprine, a low-dose immunosuppressive agent. During the 1-year period of follow-up there was no recurrence of disease with the use of low-dose immunosuppressants.
Discussion
KT is usually diagnosed by clinical and histological features, however, its etiology remains unclear. Sialolithiasis, change of ductal secretion, and local inflammation have been suggested as possible causes of KT [4,10]. KT is sometimes associated with retroperitoneal fibrosis or sclerosing cholangitis, which undermines assertions that the pathogenesis of the disease is related to immunologic processes [7,8]. Recent reports have used immunologic studies to support KT as part of the IgG4-related sclerosing disease spectrum. IgG4 occupies less than 6 percent of the total IgG fraction in the serum of normal subjects [11]. IgG4-related diseases are characterized by high levels of IgG, infiltration of IgG4 plasma cells, sclerotic changes, and good response to steroid treatment. Already well-known sclerosing diseases, including autoimmune pancreatitis, sclerosing cholangitis, and retroperitoneal fibrosis, share similar features of elevated levels of serum IgG4 and IgG4 plasma cell infiltration [12]. A study by Kitagawa et al. [5] has found that IgG4-positive plasma cells, which are distributed at low rates in sialolithiasis and Sjogren's syndrome, abundantly infiltrate the salivary glands of KT patients. The study divides chronic sclerosing sialadenitis into 2 types. In the localized type, the disease is associated with only the salivary glands. In the systemic type, on the other hand, extrasalivary glands, such as lacrimal glands, the pancreas or gall bladder can be affected along with the salivary glands. A study by Cheuk et al. [6] states that chronic sclerosing dacryoadenitis could be included in the spectrum of IgG4-related sclerosing disease, the finding of which was revealed by the immunohistochemistry of lacrimal glands. A study by Lee et al. [9] documents a case of the simultaneous occurrence of IgG4-related chronic sclerosing dacryoadenitis and chronic sclerosing sialadenitis. Both diagnoses were established through immunohistochemical staining. In Korea, a study by Kwon et al. [13] has reported two cases of IgG4-related sclerosing dacryoadenitis without the involvement of other organs. According to the above-mentioned studies of several investigators, chronic sclerosing sialadenitis and dacryoadenitis are also IgG4-related sclerosing diseases in line with other systemic sclerosing diseases.
In the present case, typical histological findings of KT were presented and T-cells were mainly located in the ducts, acini, and interfollicular spaces in lacrimal glandular tissue. Rich infiltrations of IgG4-positive plasma cells on immunostaining were consistent with the findings of recent studies. While only the level of serum IgG was elevated, its subclasses were not measured. According to the results of lacrimal gland biopsy, we assumed that previous histological findings of the submandibular glands that were insufficient to lead to diagnosis definitely were associated with KT. Lastly, even though a biopsy of extraocular muscles was not performed, CT and MRI demonstrated the hypertrophy of extraocular muscles. Therefore, a combination of histological, immunologic and image findings confirmed a case of unusual involvement of IgG4-related sclerosing disease in the lacrimal and submandibular glands, as well as extraocular muscles simultaneously. By Kitagawa's classification [5], our case can be included as a systemic type of chronic sclerosing sialadenitis. Generally this disease shows good response to steroid treatment. However, if the disease recurs frequently, as in our case, low-dose steroid or immunosuppressive treatment may be needed long-term [14].
Generally, KT involves one of the submandibular glands exclusively. However, there are some recent reports of multiple involvements of salivary glands or lacrimal glands together [7-9]. The present case indicates that IgG4-related sclerosing sialadenitis, previously called KT, can appear in the lacrimal and submandibular glands, and extraocular muscles simultaneously. This case also supports the previous idea that KT may be developed through active local inflammation by lymphocytes and IgG4-positive plasma cells based on immunohistochemical studies. Differential diagnosis of IgG4-related sclerosing sialadenitis is very important because of how difficult it is to correctly diagnose, especially when it comes to differentiating it from MALT lymphoma in the early course of disease. Another issue is that IgG4-related sclerosing disease is known as a totally benign inflammatory disease, however, some case reports have shown the potential for lymphoma to arise in scenarios of chronic sclerosing dacryoadenitis [15-18]. Whether or not close follow-up for recognizing lymphoma is necessary is a controversial subject. As in our case, however, regular follow-up visits are prudent for monitoring recurrence.

 XML Download
XML Download