

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Stenotrophomonas maltophilia (S. maltophilia) is a non-fermentative, gram-negative bacillus that has assumed an increasingly important role as a nosocomial pathogen in immune compromised patients [1]. Treatment of S. maltophilia infections is also complicated by the fact that isolates are resistant to many broad-spectrum agents [2]. Ophthalmologic syndromes, including conjunctivitis, keratitis, dacrocystitis and pre-septal cellulitis, may be caused by S. maltophilia [3]. S. maltophilia keratitis is associated with very poor prognoses because of its resistance to many broad-spectrum antibiotics [4]. We describe a case of S. maltophilia keratitis that was effectively treated with topical moxifloxacin (fourth-generation fluoroquinolone) monotherapy.
Case Report
A 70-year-old male presented to our hospital (Department of Ophthalmology, Sahm Yook Medical Center, Seoul, Korea) with a three-day history of left eye pain and decreased vision. He had a long history of diabetes mellitus that was controlled with oral anti-hyperglycemic agents. The patient suffered from bilateral proliferative diabetic retinopathy and had undergone pan retinal photocoagulation several times since March 1995. At age 60 he had undergone phacoemulsifications with intraocular lens implantation for the treatment of senile cataracts in both eyes.
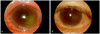
On presentation, the patient's visual acuity was hand motion in the left eye. Slit lamp examination revealed a heavily edematous cornea and a round 3.7 × 5.0 mm dense central stromal infiltrate with an overlying epithelial defect (Fig. 1). Anterior chamber cells 3+ and ciliary injection were also observed.
After scrapings were collected from the lesion for smears and cultures, the patient was treated hourly with 0.5% moxifloxacin and 0.5% tobramycin. Four days after the initiation of treatment, heavy growth of S. maltophilia was observed in culture. The isolated bacteria were sensitive to ciprofloxacin, sulfamethoxazole-trimethoprim, levofloxacin, and moxifloxacin, but were resistant to all aminoglycosides and B-lactams (Table 1). According to the results of susceptibility tests, topical 0.5% moxifloxacin was given every hour and 0.5% tobramycin was stopped.
The patient's corneal epithelium healed in two weeks after the initiation of treatment. After the epithelium had healed, moxifloxacin was administered four times per day. The corneal infiltrate resolved within four weeks. However, mild opacity remained in the posterior stroma (Fig. 1). The patient's best corrected visual acuity improved from hand motion to 20 / 25. His infectious keratitis was controlled and had not recurred at the one-year follow-up examination.
Discussion
S. maltophilia is a motile, non-fermentative, oxidase-negative, aerobic, Gram-negative bacillus that is widespread in the environment [5]. It is an opportunistic pathogen believed to have limited pathogenicity unless it is associated with nosocomial infections of immune compromised patients [6]. S. maltophilia is a seldom-reported pathogen in lens care systems or ocular infections [7]. However, reports of postoperative and post-traumatic S. maltophilia ocular infections are increasing [8]. The reasons underlying this emergence are complex, but may be related to the improved laboratory isolation techniques and enhanced reporting. Treatment of S. maltophilia infections is complicated by the fact that isolates are often resistant to many broad-spectrum antibiotic agents [2].
You et al. [4] reported the treatment results and prognoses of 10 cases of S. maltophilia keratitis in 2007 after one time applications of levofloxacin ophthalmic solution as a first line treatment of choice before culture results. They then added fortified tobramycin and cefazolin if corneal ulcers were large and centrally located of the cornea. Patients also underwent surgical treatment when there was no response to medication. The final visual acuity in three cases that had no co-infections was worse than hand motion.
Fourth-generation fluoroquinolones (moxifloxacin and gatifloxacin) show an enhanced spectrum of activity against Gram-positive bacteria and comparable activity to second- and third-generation fluoroquinolones (ciprofloxacin and levofloxacin) against Gram-negative bacteria [9]. New ocular antibiotic formulations with improved potency, such as moxifloxacin ophthalmic solution 0.5% (Vigamox®; Alcon Laboratories, Fort Worth, TX, USA) or gatifloxacin ophthalmic solution 0.3% (Zymar®; Allergan, Irvine, CA, USA) are currently available and have been shown to inhibit growth of organisms resistant to second- and third-generation fluoroquinolones [10]. Several in vitro susceptibility studies, demonstrate that moxifloxacin is more active than earlier generation fluoroquinolones (ciprofloxacin, ofloxacin, and levofloxacin), especially against S. maltophilia [9]. For these reasons, we chose moxifloxacin monotherapy for treatment of S. maltophilia keratitis, even though antibiotic sensitivity was equal for both levofloxacin and moxifloxacin.
In conclusion, we report the case of a patient who was diagnosed with S. maltophilia keratitis and effectively treated with moxifloxacin monotherapy. Unlike most previously-reported cases, which had poor prognoses, in our patient moxifloxacin monotherapy led to a good visual outcome.

 XML Download
XML Download