

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Metastatic neoplasms of the orbit and periorbit are very rare, estimated to account for 1-13% of all reported orbital tumors [1]. A literature search revealed that there have been only four reported cases of orbital metastasis from esophageal tumors [2-5]. In two of these cases, the metastases originated from squamous cell carcinomas of the esophagus, and in the others, the metastases originated from esophageal adenocarcinomas. If such tumors grow rapidly, they may undergo necrosis, as the rate of tumor angiogenesis cannot keep pace with the rapidly expanding mass. Here, we report a rare case of an orbital metastasis from a squamous cell carcinoma of the esophagus, mimicking a periorbital abscess in a patient with no previously known history of malignancy.
Case Report
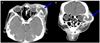
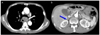
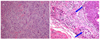
A 61-year-old man presented with a rapidly expanding left periorbital mass which he had first noticed one month prior to presentation (Fig. 1). The mass was firm with a pus-like discharge draining spontaneously from its center. The patient was ill-appearing and complained of dyspepsia and weight loss. He also complained of ocular pain and headaches. His past medical history was otherwise unremarkable. He was admitted for evaluation and treatment. His vision was 6/12 in both eyes; the intraocular pressures were 22 mmHg in the right eye and 30 mmHg in the left eye. Slit lamp examination revealed marked chemosis and injection of the left eye. There was no diplopia or limitation in duction. An orbital CT scan revealed a well-defined 4.2 cm×3.5 cm lesion in the left orbital and periorbital areas. There was no evidence of bone erosion (Fig. 2). Biopsies of the mass and conjunctiva were consistent with squamous cell carcinoma (Fig. 3). We referred the patient to the Department of Hemato-oncology, where a systemic workup revealed a primary esophageal carcinoma, a tracheoesophageal fistula, a lung metastasis, and a right adrenal gland metastasis (Fig. 4). The patient was treated conservatively, but he expired after one month of treatment.
Discussion
In contrast to intraocular metastases, orbital metastases are a rare manifestation of systemic malignancies; such orbital metastases account for only 1-13% of all orbital tumors [1]. However, the precise incidence of these lesions is difficult to estimate. The incidence of orbital metastases has increased in recent years because improvements in treatment modalities and diagnostic tools have resulted in improved survival in cancer patients. Occult cases have been reported: autopsy reports have revealed that 10-30% of breast cancer patients develop detectable ocular and orbital metastases [6].
Most orbital metastases arise from carcinomas, with lung, breast, and prostate being the most common primary sites [7]. Gastrointestinal carcinomas are the source of 6-7% of all orbital metastases. The majority of these carcinomas arise in the stomach, ileum, or colon. Our literature search revealed only four reported cases of orbital metastases originating from esophageal tumors [8,9]. Orbital metastases usually occur during the advanced stage of cancer, although there is no known history of cancer in 19-25% of patients. Ophthalmologic symptoms may be preceded by systemic symptoms, especially if the primary site is the lung, gastrointestinal tract, thyroid, or kidney [2,10].
The most common manifestations of orbital metastases are diplopia, exophthalmos, inflammation, decreased visual acuity, pain, chemosis, and eyelid swelling, depending on the site affected. The symptoms usually occur acutely and progress rapidly, over the course of weeks to months [2,9].
The aim in treating orbital metastases is to relieve discomfort. Surgical removal of the mass is not recommended. Regardless of the primary tumor type, prognosis is poor, because patients with orbital metastases are usually at an advanced stage of the disease. In one report, the mean survival time was 7.4 months. In another report [11], the median survival time was 1.3 years, and the two-year survival rate is 27%. The survival duration was not significantly different among patients with different types of primary neoplasms [12].
In our patient, ocular symptoms were the initial manifestation of an unknown primary carcinoma. The rapid growth of the metastatic cancer led to tumor necrosis and the clinical appearance of a periorbital abscess. Prompt surgical biopsy enabled confirmation of a squamous cell carcinoma, and subsequent systemic evaluation revealed primary esophageal squamous cell carcinoma with multiple metastases. Orbital and periorbital metastases can present atypically, and clinicians should be cognizant of this fact so that patients can be diagnosed in a timely manner. Biopsy is needed to confirm the diagnosis.

 XML Download
XML Download