

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Radiation retinopathy gradually progresses for a given period of time after irradiation in oculi or cranium, and results in various lesions of the retina and the retinal vessels such as microaneurysm, telangiectasia, capillary non-perfusion, vascular obstruction, vascular leaking, perivascular inflammation, papilledema, hard exudates, and neovascularization. It finally gives rise to neovascular glaucoma, retinal new vessel, tractional retinal detachment and vitreous hemorrhage at late stage.1-4 It is difficult to presume the exact incidence of radiation retinopathy, but it is reported that radiation retinopathy is rarely induced 6 months before or 3 years after radiation therapy.5 As the dose of total radiation increases, the possibility of developing radiation retinopathy also increases, and at the same radiation dose, the frequency of radiation retinopathy increases in the closer eye.6 In this case, radiation retinopathy occurred in the left eye despite the radiation therapy to the right frontal area. We report this case in which the contralateral eye radiation retinopathy developed sparing the ipsilateral eye.
Case Report
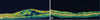
A 37-year-old female visited with a complaint of gradually decreased visual acuity. At the first ophthalmological examination, the corrected best visual acuities in the right eye and the left eye were 1.0 and 0.4 respectively. Slit lamp examination revealed that there was no specific finding in the anterior segment, and the funduscopic finding of both eyes showed that cotton wool spots, macular edema and vascular tortuosity were present around the optic disc in the left eye (Fig. 2A), but the right eyes was unremarkable except the suspected cotton wool spots near superotemporal arcade (Fig. 2C). Fluorescein angiography revealed microaneurysms and macular edema in the left eye (Fig. 2B), and right eye showed minimal microaneurysms without macular edema (Fig. 2D). We found that the thickness of macula was increased when measured by optical coherent tomography (Fig. 3A). Past medical history included modified radical mastectomy for right breast cancer 5 years ago. She had no medical history of diabetes, hypertension and systemic vascular disease and no evidence of abnormalities in laboratory finding.
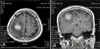
One year before this visit, she was confirmed to have metastatic tumor on her right frontal lobe shown on MRI (Fig. 1) which was taken after a sudden convulsion. And she had received radiation therapy of fractionated external irradiation to the whole brain (3,000 cGy/10fraction) for 2 weeks and local boost irradiation (1,200 cGy) After that, she was transferred to another hospital for gamma knife surgery on that lesion. Total dose of gamma knife surgery on the tumor bed was 40 Gy and the amount of irradiation for each eye was 0.2 Gy.
Immediate intravitreal TA injection was performed for macular edema and two weeks later, the visual acuity was improved to 0.6. But the visual acuity was decreased to 0.3 again 3 months later, so we performed intravitreal TA injection again. Three months after the second injection, the fundus examination and optical coherent tomography revealed that retinal thickness was improved and the corrected best visual acuity was 0.5.
Discussion
Radiation therapy is a useful treatment option for malignant or benign tumor, and it is an important treatment for head and neck cancer. However, there are various side effects of radiation therapy including blepharitis, keratoconjunctivitis, corneal epithelial atrophy, cataract, etc. But it is reported that complication appears slowly at posterior segment such as the optic nerve as compared to anterior segment after radiation therapy.3,7
Radiation retinopathy is microangiopathy that is developed several months or several years after radiation therapy, accompanying with occlusion of retinal vessels and change of permeability.5 In 1933, Stallard8 reported radiation retinopathy for the first time, and Seong et al.9 reported a case of radiation retinopathy for the first time in Korea followed by several reports on cases.
It is reported that the higher the total exposed radiation dose and the higher the fraction dose, the higher frequency of development of radiation retinopathy.1 In general, 35 Gy is the highest limit of safe radiation dose,10 and there is little chance of causing radiation retinopathy with lesser radiation dose than that.6,11-13 It is reported that there is a 50% chance of developing radiation retinopathy with a dose of 60 Gy and 85-90% chance with a dose of 70-80 Gy.10,14 Parsons et al.12 reported that the danger of radiation retinopathy is higher in the higher radiation dose exposed per a time, and the radiation dose should not exceed 1.8-1.9 Gy per a time. Furthermore, the nearer the eye is to the irradiation site, the more radiation retinopathy develops. According to Amoaku et al.,6 after performing radiation therapy, radiation retinopathy develop in ocular or periorbital area with 85.7% chance, in paranasal sinus with 45.4% chance, in nasopharynx with 36.4% chance and in cranium with 3.1% chance. Although the higher amount of total radiation dose and increased fraction dose, the higher chance of developing radiation retinopathy gets, there is a discrepancy among reporters about threshold of radiation dose that causes radiation retinopathy. Merriam et al.10 reported that it is safe within 35 Gy of radiation dose, while they reported that radiation retinopathy can be developed with lesser amount of radiation dose in another report. Peterson et al.15 performed radiation therapy with a dose of 20 Gy to 242 people and 30 Gy to 69 people, and reported that there was no occurrence of radiation retinopathy during the follow-up period. And some report that radiation retinopathy was not developed to a patient who was exposed to 25-45 Gy of radiation dose.12,16
It is also reported that the development of radiation retinopathy can be quickened when accompanying chemotherapy that makes retinal vasculature be easily damaged by radiation and increases the risk of radiation retinopathy.5,7 It is also reported that existing abnormal vascular disease such as diabetic retinopathy, works as a risk factor for the development of radiation retinopathy. According to Gass,17 diabetic retinopathy can be aggravated in the retina where radiation therapy was performed, and Brown et al.5 reported that macular injury was induced to one person among 20 people who have diabetes.
In general, the nearer to irradiation site, the frequency of developing radiation retinopathy increases, but in this case, total dose of external beam radiation was 30 Gy and local booster irradiation dose on tumor bed was 12 Gy which are lower doses to induce radiation retinopathy. We could not find radiation retinopathy in the right eye despite the large dose of brachytherapy given to the right eye. Rather, radiation retinopathy was developed only in the left eye where the lesser amount of radiation was exposed. This patient does not have diabetes, but was being treated with chemotherapy as well as radiation therapy. Despite of the effects of comparatively small amount of radiation, radiation retinopathy was induced in the left eye that can be explained by several reports that said radiation retinopathy can be induced with little amount of radiation when accompanying chemotherapy.5,7,17
Laser photocoagulation is a widely used and approved treatment for macular edema caused by radiation retinopathy,18-20 but in this case, we performed injection of intravitreal triamcinolone acetonide for the treatment of macular edema resulting in decreased retinal thickness and improved the visual acuity. Cortcosteroids have been used for the treatment of cystoids macular edema as a mechanism that includes inhibition of arachidonic acid pathway, downregulation of vascular endothelial growth factor and reduction of blood-retinal barrier breakdown.21-23 After 3 months of observation additional intravitreal triamcinolone acetonide injection was performed because of recurrence of macular edema, and that decreased retinal thickness and improved the visual acuity. After 5 months of observation, there was no recurrence of CME and the vision remains stable.
From this case, we conclude that careful radiation blocking is also required on the opposite side of irradiation site, considering that radiation retinopathy can be developed with a little amount of radiation if combined with chemotherapy, at the site away from irradiation site. This case also demonstrates that careful observation is needed for both eyes when performing fundus examination, and the injection of intravitreal triamcinolone acetonide is an effective treatment for cystoid macular edema when radiation retinopathy has developed.

 XML Download
XML Download