

 PDF
PDF ePub
ePub Citation
Citation Print
Print


It is widely known that central corneal thickness (CCT) affects the measurement of intraocular pressure (IOP) by Goldmann applanation tonometry (GAT).1 This is because IOP measured by GAT is calculated according to the modified Imbert-Pick law with the assumption that the CCT is 550 µm.1 In a recent study of Zhang and colleagues,2 the mean±SD of CCT in Chinese adults was 556±33.1 µm (median: 553 µm, range: 429-688 µm). When this wide range of CCT is considered, a tonometer minimally affected by CCT is of clinical importance.
The dynamic contour tonometer (DCT; Pascal®; Swiss Microtechnology AG, Port, Switzerland) is a device that may measure IOP relatively independently of CCT. The DCT sets a hypothetical corneal contour that is achieved when the pressures on the two sides of the cornea are equal. The force distribution needed to gently fit the corneal surface to that hypothetical contour counterbalances the force distribution generated by the IOP. Hence, a pressure sensor centrally and concavely embedded into the tonometer tip precisely measures the transcorneal pressure of the eye.3
Although a few studies have compared IOP measured by DCT with IOP measured by GAT, it remains unclear whether either measurement is affected by CCT. Kaufmann et al.4 and Schneider et al.5 reported that IOP measured by DCT was not significantly affected by CCT. Kotecha and co-workers6 concluded that DCT was less affected by CCT than was GAT. However, Doyle and Lachkar,7 in a study which included 75 eyes, concluded that DCT permitted accurate assessment of true IOP in eyes with thin and structurally normal corneas, but had no advantage over GAT in eyes with thick corneas. Thus, this study was intended to compare IOPs measured by DCT with those obtained using GAT, and investigate the association of IOP data with CCT in a considerably large number of eyes.
Materials and Methods
This prospective single-center study assessed 451 eyes of 233 subjects (mean±SD age: 54.9±13.8 years) recruited from the glaucoma clinic at the Asan Medical Center, Seoul, Korea, from October 2005 to September 2006. All subjects were referred from primary eye care clinics upon suspicion of glaucoma.
Each subject was initially seen by one of our glaucoma specialists (J.C. or C.H.L.) and underwent IOP measurements by GAT and DCT. After one drop of 0.25% solution of sodium fluorescein in combination with Alcaine® (proparacaine chloride; 5 mg/mL; Alcon, Fort Worth, TX) was instilled into the lower conjunctival fornix, IOP measurement was performed with GAT and DCT sequentially 5 minutes apart. GAT was performed according to the guidelines of the Eye Care Technology Forum.8 DCT was measured with a Pascal tonometer mounted on a slit-lamp. DCT shows IOP as a digital numeric outcome. Thus, prior knowledge of the GAT value would not influence the DCT result, which made it unnecessary to mask the examiner to the results of the two IOP measurements. IOP measurement with DCT was repeated if the quality score was greater than 2.
Next, CCT measurements using ultrasonic pachymetry (Pachette2® pachymetry; DGH Technology Inc.; Exton, PA) were performed. The examiner thus measured IOP independent of CCT. Corneal thickness was measured three times within the pupil margin, and care was taken not to dent the cornea with the pachymetry tip. Values were accepted if the standard deviation of each measurement was within 5.0 µm. An average of three measurements was obtained for data analysis.
Patients were enrolled if the IOP was below 30 mmHg, and the corneal surface was smooth and regular so that GAT could be used. As marked astigmatism of more than four diopters can result in erroneous GAT measurements, such patients were excluded.9 Patients under 20 years of age were excluded because of restlessness during IOP measurements which might lead to unreliable IOP data.
All participants gave an informed consent. All procedures conformed to the Declaration of Helsinki and the study was approved by the Ethics Committee of the Asan Medical Center at the University of Ulsan, Korea.
IOPs measured by GAT, and DCT, were tested for association using the Pearson correlation. Next, subjects were divided into three groups according to CCT measurements using 520 µm and 550 µm as cut-off values, and similar number of eyes were allocated to each group: a thin cornea group (group A, CCT<520 µm, n=146), a normal cornea group (group B, 520 µm ≤ CT ≤550 µm, n=163), and a thick cornea group (group C, CCT>550 µm, n=142).
The effect of CCT on IOP measurement was tested by mixed effect model accounting for clustering of eyes within subject, gender and age. One eye (left eye) was incorporated into multivariate regression model for validation of those findings determined by mixed effect model. After CCT was conformed to be a statistically significant parameter based on multivariate regression model, Pearson correlation analysis was further performed to obtain coefficient (R). SAS® (SAS Institute Inc., Cary, NC) version 9.1 and SPSS® (SPSS Inc., Chicago, IL) version 11.5 was employed for statistical analysis.
Results
Data on patient demographic and background variables for all subjects and for each group classified by corneal thickness are shown in Table 1. All patients were Korean, and 184 (40.8%) eyes were of men whereas 267 (59.2%) were of women. The mean (±SD) of age was 54.9±13.8 years (range, 21-82 years). IOP measured by DCT was significantly higher than IOP measured by GAT (14.8±3.7 mmHg versus 16.9±3.4 mmHg; p<0.001; paired t-test). There were no significant differences in age, gender, spherical equivalent and visual field mean deviation (MD) among group A, B, C (p=0.419, p=0.575, p=0.163, p=0.214 for age, gender, spherical equivalent, and mean deviation, respectively; one-way ANOVA, chi-square test).
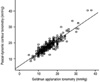
Figure 1 depicted statistically significant correlations between IOPs measured by GAT and DCT (R=0.853, p<0.001, Pearson correlation analysis). Figure 2 showed that both IOP measurements had significant correlations with CCT (GAT; R=0.330, p<0.001), (DCT; R=0.271, p<0.001). IOP measured by GAT was associated with CCT in groups B and C whereas IOP measured by DCT in group C only (Table 2). Table 3 showed the effect of CCT on IOP measurement using multivariate regression in left eye. Pearson correlation coefficients (R) were assessed when IOP measurements were influenced by CCT.
Discussion
Many studies have discussed the influence of CCT on IOP as measured by GAT. No general consensus has been reached regarding the correction factor that should be used for adjusting IOP measured in this way.1 According to Ehlers and colleagues, the average error is 0.7 mmHg per 10 µm.10 In a more recent study, however, Wolfs and co-workers suggested smaller values, as little as 0.19 mmHg per 10 µm, should be used to correct GAT values.11 There is thus agreement that CCT influences IOP measurement, but different correction factors have been proposed. This suggested the need for a tonometry mode that would yield correct data independent of CCT, and DCT was developed for that purpose.
Theoretically, IOP measured by DCT should not be affected by CCT. In this study, however, IOP measured by DCT was significantly affected by CCT in the thick cornea group (p<0.001). Despite this finding, DCT was not significantly affected by CCT in groups with thin and normal corneal thickness. Lesser impact of CCT and a good correlation between DCT and GAT measurements increase the clinical value of DCT. These results agreed with those of other studies in smaller series.4-77 Doyle and Lachkar calculated that IOP measured by GAT was underestimated by 0.7 mmHg for every 10 µm of CCT below 520 µm, and overestimated by 0.2 mmHg for every 10 µm of CCT over 580 µm; these data support the idea that DCT is more accurate than GAT when used on thin or normal corneas.7 The cited study used 75 eyes, but we examined 451 eyes. Doyle and Lachkar considered that there was much greater variability in data from the two tonometers when used on thick corneas, and added that this result was unexpected and difficult of explanation.7 Similarly, we cannot offer a conclusive reason for our result that CCT influences IOP measured by DCT. It is possible that other unknown corneal factors other than CCT, such as hysteresis, might affect the measurement of IOP by DCT. Corneal thickness per se may not be the direct cause of high IOP. Instead, if eyes with thick corneas tend to have different corneal biomechanical properties that are difficult to quantify, CCT can be mistaken for the cause of high IOP although the real cause lies with biomechanical property such as hysteresis. However, data from this study, is not sufficient to explain the findings in the thick cornea group and this is one of limitation of our study.
Another limitation of this study is the arbitrary cut-off values of CCT used for dividing patients into groups. The three groups were intended to represent thin, normal, and thick cornea groups. However, there is no consensus on classification of corneas as thin, normal, or thick. Goldmann and Schmidt used 520 µm as an average corneal thickness in their work with the modified Imbert-Fick law.1,12 In other studies, the mean values were 537 to 554 µm in normal subjects.1,11,13 In addition, CCT varies with race; an average of 531 µm in one African-American population, a mean of 547 µm in Latinos, and an average of 552 µm in Japanese and Caucasians.1,14-18 Considering these findings, we divided our subjects into three groups using 520 µm and 550 µm as cut-off values, resulting in similar number of eyes allocated to each group.
A third limitation of this study is the lack of normal control group. We could not collect data from normal control group, thus further study which includes normal population can be of value to complement the limitation of this study.
In conclusion, we found that IOP measured by DCT correlates well with IOP measured by GAT. IOPs obtained by DCT are less dependent on, but not totally independent of CCT, compared to those measured by GAT, especially when the corneal thickness is normal or thin. These findings indicate that DCT measure can be less affected by CCT than that of GAT in patients who have normal or thin corneas.




 XML Download
XML Download