

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Lymphoproliferative disease in the orbit has diverse clinical manifestations. The most substantial clinical issue is to recognize the lymphoproliferative diseases from the orbital inflammatory lesions. Initially, two conditions might have common disease manifestations including imaging studies.1
Nonspecific orbital inflammation varies clinical presentations according to pathologic characteristics and which part of the orbital tissue is involved. Although the disorder takes heterogeneous form of clinical symptoms, it is usually responsive to anti-inflammatory agents.2
Painful ophthalmoplegia can be resulted from inflammatory lesions in the orbital apex or cavernous sinus. We present a patient who had painful ophthalmoplegia unresponsive to corticosteroid treatment and was disclosed to have a peripheral T-cell lymphoma. To the best of our knowledge, this is the first case of peripheral T-cell lymphoma in the orbit in Korea.
Case Report
A 61-year-old woman presented with a 2-week history of headache and left eyeball pain. She had no specific medical history or systemic disease. Visual acuity was 20/20 in both eyes. Intraocular pressure was 12/15 mmHg. There was 2-mm of proptosis and complete ptosis in the left eye. Extraocular movement was markedly limited in all directions of gaze in the left eye (Fig. 1). Anterior and posterior segment examination showed no specific abnormalities except conjunctival injection of the left eye. She had no lymphadenopathy. CT scan of the orbit showed a subtle enlargement of extraocular muscles in the left orbit (Fig. 2A). Under the impression of nonspecific orbital inflammation, she was treated with oral prednisone with initial response.
Two months later, she revisited the clinic with exacerbated symptoms. Examination disclosed no light perception and 4-mm of proptosis of the left eye. Fundoscopy showed central retinal artery occlusion. Sensation of the V1 and V2 area was decreased. CT scan of the orbit revealed diffuse homogenous enlargement of extraocular muscles and a haziness of intraorbital fat in the left orbit (Fig. 2B, C). Anterior orbitotomy and incisional biopsy was performed for the inferior rectus muscle lesion.
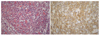
Histopathologically, atypical lymphoid infiltrates were present between scattered, degenerated muscular bundles. Atypical lymphocytes were small to medium sized with irregular nuclear outlines and inconspicuous nucleoli (Fig. 3A). They were strongly positive for T cell marker, UCHL-1, but negative for B cell marker, L26, immunohistochemically (Fig. 3B). Based on the histologic and immunophenotypic features, this tumor was consistent with peripheral T-cell lymphoma.
A metastatic workup, consisting of abdominal CT, lumbar puncture, and bone marrow biopsy was performed without any evidence of extraorbital tumor. The patient was recommended to be treated with chemotherapy and radiation therapy. However, she refused to take the treatment. The patient died of progression of the disease in a month.
Discussion
Malignant lymphomas arising in the orbit and ocular adnexa account for 8% of all extranodal lymphomas.3 Most orbital lymphomas are non-Hodgkin's B-cell lymphoma. Orbital T-cell lymphomas are exceptionally rare, with only a few case reports in the literature.4
The diagnosis relies on recognition of a characteristic histology with a leukemic growth pattern, lymphoid cells with intermediate nuclear size, fine chromatin, indistinct nucleoli, and frequent mitotic figures.5 Peripheral T-cell lymphomas are characterized by infiltrates of malignant cells whose immunophenotypes mimic mature T cells.6 A battery of monoclonal antibodies consist of Leu-22, UCHL-1, L-26, leukocyte common antigen and Ki-1.7 Leu-22 is more sensitive in detecting T-cell non-Hodgkin's lymphoma than is UCHL-1. However, UCHL-1 is more specific, in that it does not stain as many B-cell non-Hodgkin's lymphomas as does Leu-22. The L-26 is a pan B-cell marker and highly sensitive and specific for B-cell.8
At the time of diagnosis, peripheral lymphadenopathy is common and visceral involvement is unusual. Involvement of the orbit in T-cell lymphomas is commonly associated with a previously recognized systemic disease.9 More rarely, these lesions may have an initial systemic presentation as an orbital mass or may be limited to the orbit as in our case.10 Those orbital involvement include exophthalmos, a smooth or ulcerating conjunctival mass, lid edema, chemosis, or pain.11 It should be noticed that the inflammatory clinical signs can be associated with clinical manifestations by T-cell lymphoma as in our case.
Localized T-cell lymphoma in the orbit should be treated carefully with planned local radiation plus systemic chemotherapy. However, prognosis is poor once dissemination occurs, and long-term remissions, even with aggressive chemotherapy, are rare.11 Saga et al2 reported two patients with peripheral T-cell lymphoma involving the orbit secondarily from the testicular lymphoma. The patients received chemotherapy and local radiation, but died of progression of the disease. Leidenix et al7 reported the case of primary T-cell lymphoma confined to the orbit in a pediatric patient. The patient received surgical excision, systemic chemotherapy, and local radiation and died of dissemination of the disease. Hassan and Elner6 reported orbital peripheral T-cell lymphoma in a child who responded to local radiation and systemic chemotherapy. T-cell lymphoma is generally rapidly progressive and likely to have a high mortality despite aggressive treatment.
In conclusion, T-cell lymphoma in the orbit can present as painful ophthalmoplegia and take a rapid clinical course. The disease should be regarded as one of the differential diagnosis for painful ophthalmoplegia refractory to corticosteroid therapy.


 XML Download
XML Download