

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In primary angle-closure glaucoma (PACG), the cause of elevated tension is closure of the anterior chamber angle where the trabecular meshwork resides, and the angle closure can be by either appositional or synechial mechanism. When the iris has become permanently adherent to the trabecular meshwork, aqueous outflow can be obstructed chronically.1 Two patterns have been suggested concerning the mode of development of PAS (peripheral anterior synechiae): peripheral iris is first adherent to Schwalbe's line after which PAS extends toward the angle recess, and peripheral iris first attaches to the angle recess after which PAS extends toward Schwalbe's line.2,3 Gorin mentioned that the former mode of closure occurs during an acute attack, while the latter mainly occurs in chronic forms of PACG.2 While PAS develops with prolonged or recurrent acute attacks, its mode and mechanism may differ from synechial closure in the chronic form of PACG that begins slowly from the periphery toward Schwalbe's line.2,4
Several studies have demonstrated a possible relationship between the extent of angle closure by PAS and the failure of iridotomy to control intraocular pressure (IOP) or to prevent progression of glaucoma.5-7 Once glaucomatous optic neuropathy associated with synechial angle closure occurs, iridotomy alone is relatively ineffective in controlling IOP.8 Therefore, it may be that the more extensive the PAS, the more chronic the disease process in PACG patients. Therefore, the chronicity of PACG is expected to correlate with the severity of visual field defects, and in this paper we have evaluated the relationship between PAS and visual field defects in PACG.
MATERIALS AND METHODS
Seventy-three eyes of 64 consecutive Asian patients with PACG that were examined at the glaucoma clinic at the Korea University Hospital between 1998 and 2000 were reviewed. In this study, we excluded patients with congenital anomaly, neovascularization on irides, and secondary angle-closure glaucoma (ACG) due to chronic anterior uveitis. The subjects that were included in this study fulfilled the following criteria: (1) closed angle by gonioscopic examination, (2) visual acuity greater than 20/70 at the time of visual field examinations, and (3) reliable visual field. Usually, only one eye of each patient was included in our study. However, when both eyes of a patient were eligible but strikingly different in the extent of PAS and the severity of visual fields, we included both eyes in our analysis.9,10
We classified PACG into: (1) angle-closure suspect with occludable angle and normal IOP without glaucomatous optic disc changes; (2) angle-closure hypertension with closed angle and high IOP but without demonstrable optic nerve and visual field changes; (3) chronic ACG with closed angle, elevated IOP, and optic nerve and visual field changes; and, (4) acute ACG with closed angle, high IOP, and secondary ocular pain and hyperemia.11 In this study, we included only the eyes with angle-closure hypertension, chronic ACG, and acute ACG. We excluded angle-closure suspects in this study because of the lack of any major component of glaucoma.
Gonioscopic examination was performed by one of the authors (YYK) using a Goldmann contact lens and a slit-lamp biomicroscope. Indentation (compression) gonioscopy12 was also performed using a Zeiss gonio lens. In each patient, gonioscopy was performed on presentation or repeated after the clarity of the cornea was restored through intensive medical therapy. Closed angle was confirmed and a distinction was made when the trabecular meshwork was occluded either by appositional or synechial closure. PAS was considered present when the adhesion reached to the midtrabecular meshwork upon indentation (compression) gonioscopy. The circumferential occlusion by PAS was graded between 0 and 360 degrees.
Visual field tests were carried out after stabilization of IOP and visual acuity following appropriate medical treatments and lasers, but before surgical treatments such as trabeculectomy. All the eyes included in this study had reliable visual fields (fixation loss < 20%, false positive- or negative-responses < 33%), and pupil diameters of 3 mm or greater during the tests. A Humphrey Visual Field Analyzer (model 750, Humphrey Instruments, Inc, Dublin, California; C24-2 program) was used to perform visual field tests, and the visual field defects were graded as none (grade 0), minimal (grade 1), moderate (grade 2), and severe (grade 3). Grading of the visual field defects was based on the overall extent and also the proximity of defects to fixation using the classification system of Hodapp et al13 with some modifications. The three criteria for minimal (grade 1) defect were: (1) mean deviation (MD) < -6 dB, (2) less than 25% (14 points) of the points depressed below 5% level and less than 10 points below 1% level on pattern deviation plot, and (3) no point in the central 5 degrees with a sensitivity <15 dB. The four criteria for moderate (grade 2) defect were: (1) MD < -12 dB, (2) less than 50% (27 points) of the points depressed below 5% level and less than 20 points below 1% level on pattern deviation plot, (3) no point in the central 5 degrees with a sensitivity of 0 dB, and (4) only 1 hemifield with a point of sensitivity <15 dB within the central 5 degrees. The criterion for severe (grade 3) defect was any one of the following: (1) MD worse than - 12 dB, (2) more than 50% (27 points) of the points depressed below 5% level and more than 20 points below 1% level on pattern deviation plot, (3) any point in the central 5 degrees with a sensitivity of 0 dB, or (4) points within the central 5 degrees with sensitivity <15 dB in both hemifields.
The degree of associations between the severity of visual field defects and the extent of PAS and/or other variables was analyzed with Spearman's rank correlation test using StatView (version 5.0, SAS Institute, Inc.) program. The confidence interval (CI) of Spearman's correlation coefficient was calculated with Confidence Interval Analysis Program (version 1.2, Gardner MJ et al, the BMJ Publishing Group).
RESULTS
There was a female predominance in our total study population of 64 patients (49 females and 15 males). The mean age of the study subjects was 63.4 ± 8.2 years (mean ± SD; range, 47-81 years). Of the 73 eyes, 28 (38%) had acute ACG, 13 (18%) had angle-closure hypertension and 32 (44%) had chronic ACG. The mean IOP on presentation was 34.0 ± 18.8 mmHg (range, 8-80 mmHg) (Table 1).
Treatments included laser treatment (iridotomy alone, iridotomy and subsequent argon laser peripheral iridoplasty, or combined iridotomy and argon laser peripheral iridoplasty) in 27 (37%) eyes, laser treatment and subsequent medication in 24 (33%), trabeculectomy only in 9 (12%), combined glaucoma and cataract surgery in 3 (4%), laser treatment and subsequent trabeculectomy and medication in 1 (1%), trabeculectomy and subsequent medication in 3 (4%), cataract extraction only in 1 (1%), and medication only in 5 (7%).
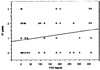
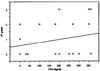
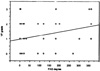
Spearman's correlation coefficient between the severity of visual field defects and the extent of PAS in all eyes (n = 73) was 0.348 (95% CI: 0.128~0.536, P = 0.003) (Fig. 1). When we divided the eyes into those with acute attacks (acute ACG eyes, n = 28) and without acute attacks (angle-closure hypertension and chronic ACG eyes, n = 45), Spearman's correlation coefficient was 0.338 (95% CI: -0.040~0.604, P = 0.079) (Fig. 2) in eyes with acute attacks (n = 28) and 0.377 (95% CI: 0.094~0.604, P = 0.012) (Fig. 3) in eyes without acute attacks (n = 45).
Both the correlation and statistical significance (Spearman's correlation coefficient = 0.439, P = 0.0006) for the patients' age in conjunction with PAS may be indicative of the importance of duration, as well as the extent of PAS, in relation to visual field defects, since the duration of PACG was not available. Other variables such as gender, systemic diseases (diabetes and systemic hypertension), presence of iris atrophy, and clinical typing by symptoms (acute, subacute and chronic) did not show any correlation with the degree of PAS or the severity of visual field damage. Nor did any of them significantly influence the correlation between the severity of visual field defect and the extent of PAS.
DISCUSSION
Our study demonstrated that the extent of PAS correlates with the severity of visual field defects in PACG. That is, a patient who has an extensive PAS occlusion along the angle usually has a greater severity of ACG, with respect to visual field defects, than a patient who has minimal PAS. In fact, the moderately strong, positive correlation between the extent of PAS and the severity of visual field defects (Spearman's correlation coefficient = 0.348) was unequivocally statistically significant (P = 0.003; 95% CI, 0.128~0.536) in our study population.
PACG is caused by insidious creeping angle closure in many of the Asian chronic PACG eyes.11,14,15 When we divided the study eyes into the two groups with and without acute attacks, in order to differentiate the chronic process of angle-closure from the acute mode of action, the correlation analysis remained statistically significant (Spearman's coefficient = 0.377, P = 0.012, 95% CI, 0.128~0.625) in eyes without acute attacks (chronic disease process). Interestingly, such a degree of correlation was not found in PACG with acute attacks (Spearman's correlation coefficient = 0.338, 95% CI -0.040~0.604, P = 0.079). Therefore, at least in chronic PACG, the extent of PAS does appear to correlate significantly with the severity of optic nerve damage and so serves as a useful parameter to gauge the severity of PACG with respect to glaucomatous optic nerve damage.
Acute ACG may supervene in chronic ACG patients, and patients with intermittent angle closure may progress to acute ACG.6 Moreover, chronic ACG patients may not notice the commencement of the disease if it is asymptomatic. Therefore, data on the duration of PACG was unavailable. In our study, we found a statistically significant correlation between patient age and PAS, and it may be indicative of the importance of duration, as well as the extent of PAS, in relation to visual field defects. On the other hand, we found no statistically significant correlation between PAS and visual field defect in eyes with acute attacks. During acute attacks, other variable factors such as degree of congestion, anterior chamber reaction, and magnitude of IOP elevation may influence the development of PAS.
Recently, the mechanisms and characteristics of angle closure (sagittally at a point) have undergone extensive study with ultrasound biomicroscopy.16-18 However, a real time circumferential view of angle closure still remains to be obtained. According to Chandler and Grant, the degree of elevation of IOP in PACG is directly proportional to the degree or the extent of angle closure in general.19 However, the level of tension may vary depending not only upon the extent of angle closure, but also on the efficiency of the remaining open angle. It is also difficult to evaluate the exact mechanism (synechial or appositional) of angle closure, and the rate and the magnitude of IOP elevation, at the time of the acute or subacute angle closure attack, especially during subacute or intermittent attacks. Furthermore, the duration, as well as the extent, of PAS is expected to be an important factor. Thus, the extent of PAS may not be the only variable to influence the IOP elevation or the severity of optic nerve damage in PACG. In addition, the status of uveoscleral outflow and the aqueous production capacity of the ciliary body (eye) may also be important variables. Thus, according to our study and for the reasons outlined above, whereas it is gratifying to be able to reveal a moderately strong and highly significant correlation between the extent of PAS and the severity of PACG, we should be cognizant of the probable importance of other variables.
In view of our findings, the presence of extensive PAS may even be considered sine qua non for chronic PACG since the extensive presence of PAS can validate a diagnosis of PACG. On the other hand, we should be aware that PAS was also found even in the eyes of PACG patients in the midst of an acute attack for the first time, although its subsequent correlation with visual field defects did not attain statistical significance (Fig. 2). Inoue et al also demonstrated that PAS could be seen in acute ACG and that it may be formed with a broad base during the acute attack.3 Moreover, PAS can develop within a week after shallow to flat anterior chamber following intraocular surgery.20
Perimetry is the standard psychophysical method for determining the extent of optic nerve damage in glaucoma evaluation. Although a considerable variation in their susceptibility to high IOP exists in monkeys with laser-induced ocular hypertension, significant field defects correlated with the magnitude of IOP increase, and the visual field defects progressed relentlessly to end-stage glaucoma.21 In this study, we adopted visual field severity, rather than cup-to-disc ratio, as a determinant of both the disease chronicity and the glaucomatous optic nerve damage.
A cross sectional study such as ours, however, has difficulty in establishing causal relationships from the data collected in a cross sectional time frame.22 To unequivocally establish the correlation between the extent of PAS and the severity of visual field defects, a longitudinal study may be preferable. However, due to ethical considerations, such a longitudinal study may not be feasible.
In conclusion, we evaluated the relationship between the extent of PAS and the severity of visual field defects in 73 eyes of 64 PACG patients with and without acute attacks, and found that the correlation between the two variables was unexpectedly strong, with a high statistical significance. Our results suggest that the extent of PAS may be regarded as a reliable indicator of the severity of glaucomatous optic nerve damage in PACG, and especially in chronic PACG.

 XML Download
XML Download