

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cervical epidural steroid injections are frequently used in the conservative management of neck pain, cervical radiculitis, and cervical radiculopathy51023). Success rate of subjective pain improvement was reported as 64-76%2326). However, although these injections are usually well tolerated, a variety of side effects have been reported. The incidence rate of complication has been reported to low and it mainly occurred in the cause of traumatic injury of the spinal nerve, dural puncture and infections19). Mild common side effects are facial flushing and generalized erythema, dyspnea, nausea, vomiting, dizziness, hypotension, and transient neck stiffness5691020). However, Transforaminal cervical epidural steroid injection have a potential hazard of fatal vascular injury because of the presence of a vessel that communicates with the anterior spinal artery in the posterior aspect of the foramen.
Many recent studies reported the devastated severe complication of spinal cord vascular injury, which can result in infarction, anterior spinal artery syndrome and even death24). Spinal subdural hematoma following cervical epidural steroid injection is a rare spinal vascular injury causing compression of the spinal cord. We report a rare catastrophic case of quadriparetic sequela after cervical epidural block.
CASE REPORT
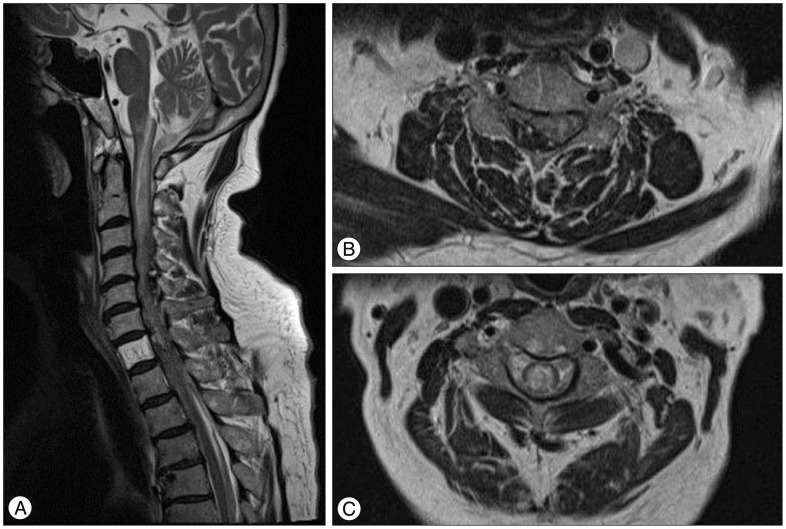
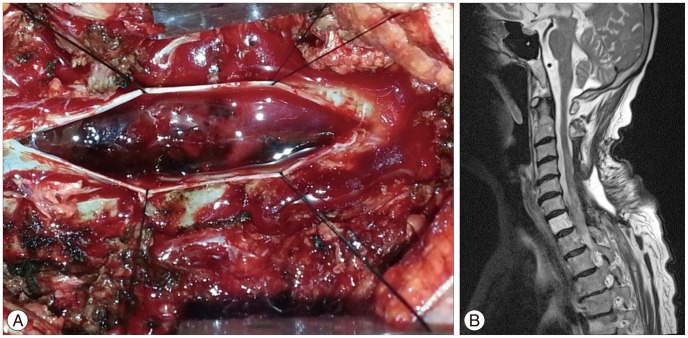
A 70-year-old female patient was transferred to our institute emergency room for acute progressive quadriparesis. The past initial cervical magnetic resonance imagings (MRI) which were checked 2 months ago showed just multiple degenerative changes without any compressive spinal cord lesion. She has been treated with cervical epidural steroid injection for neck pain in local clinic about 5 hours before hospital arrival. After cervical injection, suddenly neurological symptoms occurred and became worse progressively. At the initial neurological examination in our hospital, her mentation was awake and alert. Her pupils were both 2 mm sized and normally reacted to the brightness of light. However, she was unable to move bilateral lower extremities voluntarily at all in response to painful stimuli. Motor grade of upper extremities were 2/5 on right side and 3/5 on left side. Her all senses (pain, temperature, light touch, vibration) was decreased beneath C4-5 level. Cervical MR images showed a mottled mixed signal intensity of nodular lesions in right side of intradural and extramedullary space at level from C3 to C7 and a high intensity of spinal cord with bulging contour of spinal cord that means a spinal cord injury (Fig. 1). We planned to perform emergency operation for decompression and hematoma removal. We performed cervical laminectomy on C3-6 and evacuated hematoma via intradural approach (Fig. 2A). After emergent operation, she needed intensive care to cure bradycardia, hypotension and respiratory function for 3 weeks. Unfortunately she began a late course of motor recuperation. 3 months later, postoperative MR images showed all subdural hematoma was removed and spinal cord compressive lesion was not detected any more (Fig. 2B). Her neurological symptoms improved to motor grade 3 of lower extremities and ambulating with a wheeled walker. A physical examination showed motor strength in right upper extremities of 3/5 and left upper extremities of 4-5. Currently, she was transferred to the rehabilitation department.
DISCUSSION
Injection of steroids into or adjacent to the spinal canal is performed on a regular basis at the lumbar, thoracic, and cervical levels. Cervical transforaminal epidural corticosteroid injections are generally considered to be safe and commonly recommended for the cervical radiculopathic pain by physicians. On the other hand, some articles reported a very low incidence of serious complications1).
It is not exactly known that the prevalence of these serious complications and the mechanisms8). Inadvertent intra-arterial injection is the most often-hypothesized mechanism and the injected particulate corticosteroids might cause embolus and infarction711). Rozin et al.24) reported the case of death after transforaminal epidural steroid injection and he confirmed the cause of death was the vertebral artery dissection. Scanlon et al.25) insisted that direct arterial damage leads to dissection or thrombosis, or that vessel puncture and needle-induced vasospasms create a downstream infarction. Hodges et al.13) reported two cases having permanent neurologic sequela after cervical dural puncture. Reitman and Watters22) reported one case of a subdural hematoma following a cervical epidural steroid injection. Acute quadriplegia occurred and progressively has been recovered partially after surgical decompression, but the patient was died by meningitis. However, these report did not specify the mechanism of hematoma development. Bose3) report one case with quadriparesis following cervical epidural steroid injection. He hypothesized the patients may have suffered a vascular event from a cervical epidural injection.
Huntoon1516) reported anterior spinal artery syndrome as a complication of transforaminal epidural steroid injections. He reported anatomy of the cervical intervertebral foramina that ascending cervical and deep cervical arteries anastomosing with the vertebral artery posterior to the spinal nerves. Vascular injury may be occurred by epidural injection cervical transforaminal due to the needle cannulating a segmental artery contributed by the ascending cervical artery.
In our case of quadriparesis, acute large amount of subdural hematoma occurred after cervical epidural transforaminal steroid injection. There is high probabilty of direct arterial damage by vessel puncture because branches of radicular artery can communicate with the anterior spinal artery in the posterior aspect of the foramen.
Generally, the radicular artery arise from the vertebral artery and the ascending cervical artery and accompany the spinal nerve and its roots to the spinal cord29). This radicular artery tended to enter the foramina just inferior to the exiting spinal nerve and follow a tortuous course along the inferior and anterior aspect of the spinal nerve until it penetrated the dura to join the anterior or posterior spinal artery14). During transforaminal injection, the vertebral artery injury can be avoided by keeping the needle over the posterior aspect of the foramen. However, these radicular arterial branches may arise variably from the vertebral and especially the posterior branch can lie anterior to the course of the needle insertion16). Usual maneuver that handle the needle tip to touch the superior articular process and then redirected to enter the dorsal midpoint of the foramen can cause the injury of posterior branch of radicular artery.
To avoid unintended intravascular injection, several methods such as aspiration for blood with a syringe, radio-opaque contrast injection have been introduced. However, these techniques were shown to miss more than 50% of vascular injections, because the vascular contrast patterns have a fleeting appearance and more often spread to epidural space simultaneously27). Careful observation of the dynamic flow of contrast under live fluoroscopic view is necessary and important. Live observation using digital subtraction angiography helps us to identify more exact vascular anatomical structures and improve detection of inadvertent vascular injections24). Anesthetic test doses before corticosteroid injection are used to identify vascular entry of medications undetected by other methods but can produce adverse outcomes including transient paresis or seizure172728). In addition, intravascular anesthetics can result in cardiovascular toxicity or even death1221).
We are suggesting the strategies of preventative vascular injury in the following manner : 1) the use of high-quality imaging guidance with contrast injection and possibly digital subtraction fluoroscopy, 2) the use of blunt/pencil point needles with side port to avoid sharp needle penetration and damage to critical vessels, 3) the use of local anesthetic test dosing before injection of particulate steroid, 4) the use of steroid spreading by diffusion into the foramen with keeping needle distance from foramen.
CONCLUSION
We report a rare case of a patient who experienced serious quadriparetic complication due subdural hematoma after cervical epidural injection. The cervical transforaminal epidural injection is effective to treat cervical radiculopathy. However, the radicular artery is vulnerable and it may cause severe complications such as embolous, infarction, dissection and even catastrophic hematoma.
 XML Download
XML Download