

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Pigmented villonodular synovitis (PVNS) is a benign proliferative disease of the synovial membrane with an uncertain etiology. This tumor is characterized by the presence of inflammation and hemosiderin deposition in the synovium. PVNS commonly involves the large appendicular joints, but the axial skeletal system is rarely involved20,22,34,44,47). After the first reported case of PVNS involving the spine at 198029), only a few cases have been reported in the English-language literature. The etiology, natural history, and treatment of PVNS remain unclear. We present a case of PVNS and review the pertinent literature.
CASE REPORT
A 38-year-old man had complained of an 8-month history of lower back pain and pain in both legs. His symptoms became particularly apparent after an exercise session one month prior to presentation when he noticed that claudication developed after a long walk. He had no antecedent trauma history. An initial neurological examination demonstrated full and symmetric muscle strength in the lower extremities. Sensation was intact to all modalities, and reflexes were symmetrical and nonpathological.
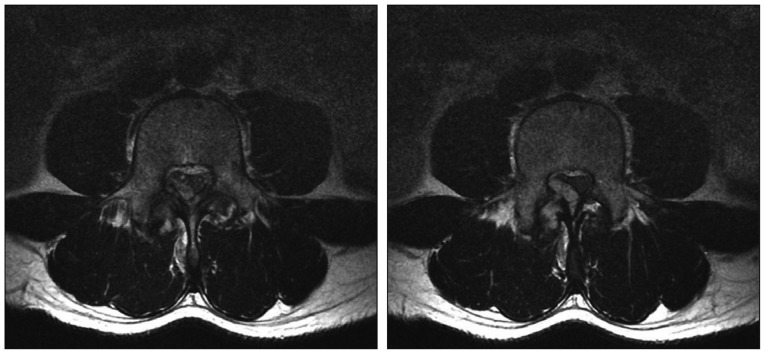
Plain radiographs of the lumbar spine revealed spondylolisthesis at L4-5. Magnetic resonance imaging (MRI) revealed a well-circumscribed 1.4-cm soft tissue mass in the region of the right lamina of L4 (Fig. 1, 2). This lesion originated from the right superior articular process of the L4 vertebra with extension to the spinal canal, forming an extradural mass that compressed the thecal sac.
A midline incision and L3-4 partial hemilaminectomy with a right approach was performed to resect the mass. The ligamentum flavum was thickened with inflammatory changes. After removing the ligamentum flavum, a yellowish-dark colored mass attached to the thecal sac was noted. Gross total removal was performed without any damage to the surrounding tissues.
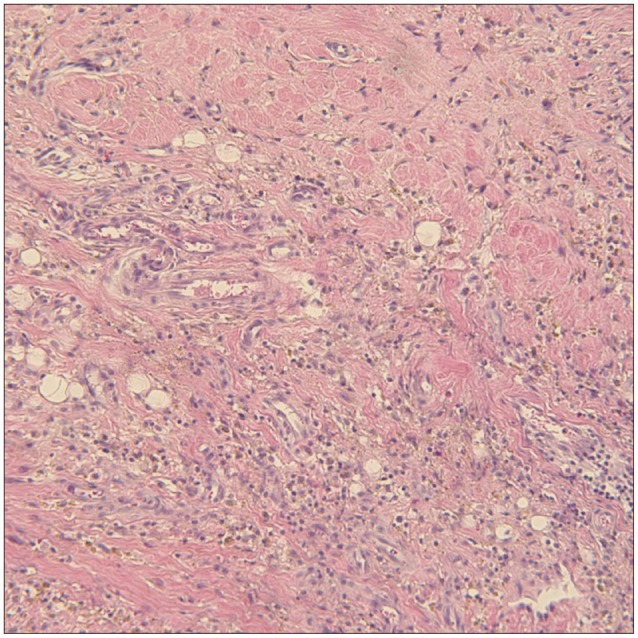
A histopathologic examination revealed a tumor composed of thick-walled blood vessels with extensive fibrosis and inflamed granulation tissue, and synovial hyperplasia with accumulation of hemosiderin-laden macrophages (Fig. 3). A diagnosis of PVNS was made.
The patient tolerated surgery well and made an uneventful recovery. The pain in the lower back and both legs improved significantly immediately after surgery, although there was some residual pain in the left calf. Follow-up contrast enhanced MRI per-formed 1 month after surgery revealed the absence of any residual mass (Fig. 4). No recurrence of symptoms was observed over the next 2 years.
DISCUSSION
The World Health Organization classification defines diffuse PVNS as a diffuse-type giant cell tumor that differentiates from a giant cell tumor of the tendon sheath and localized PVNS19). The nomenclature that describes a synovial-type giant cell tumor reflects the uncertain pathogenesis and various clinical manifestations : tenosynovitis, diffuse type PVNS, xanthomatous giant cell tumor, histiocytic giant cell tumor, xanthoma, benign synovialoma, hemorrhagic villous arthritis, and localized or diffuse pigmented villonodular synovitis. Among them, most synovial-type giant cell tumors of the spine published to date have been called pigmented villonodular synositis.
Furlong et al.20) reported 15 cases of a synovial-type giant cell tumor of the vertebral column. Eight cases displayed a diffuse growth pattern, and only one showed typical PVNS morphology. One case of the remaining seven cases was a localized pattern and six cases were an intermediate growth pattern that was difficult to subclassify. Most reports of synovial-type giant cell tumors have excluded a description of the pathological subtype, perhaps because the pathological subtype of PVNS is not related to the surgical plan for spinal PVNS cases, unlike cases involving the appendicular joints. Appendicular tenosynovial giant cell tumors are typically a diffuse type that displays a higher recurrence rate than that of the localized type. However, the small number of reported cases involving the spine and lack of information on subtype hinders typing.
The etiology of PVNS remains controversial. To date, hyperplasia, local metabolic disturbance, recurrent hemorrhage, and trauma have been mentioned as possible etiologic factors, while the inflammatory reaction and neoplasm are less clear and contentious2,21,23,50). The reason for the confusion concerning the causative factor of inflammation is that the cells involved are usually inflammatory cells, such as polyclonal CD8 positive T cells32,37), whereas the presence of trisomy 7 and clonal DNA rearrangements represent the neoplasm1,3,41).
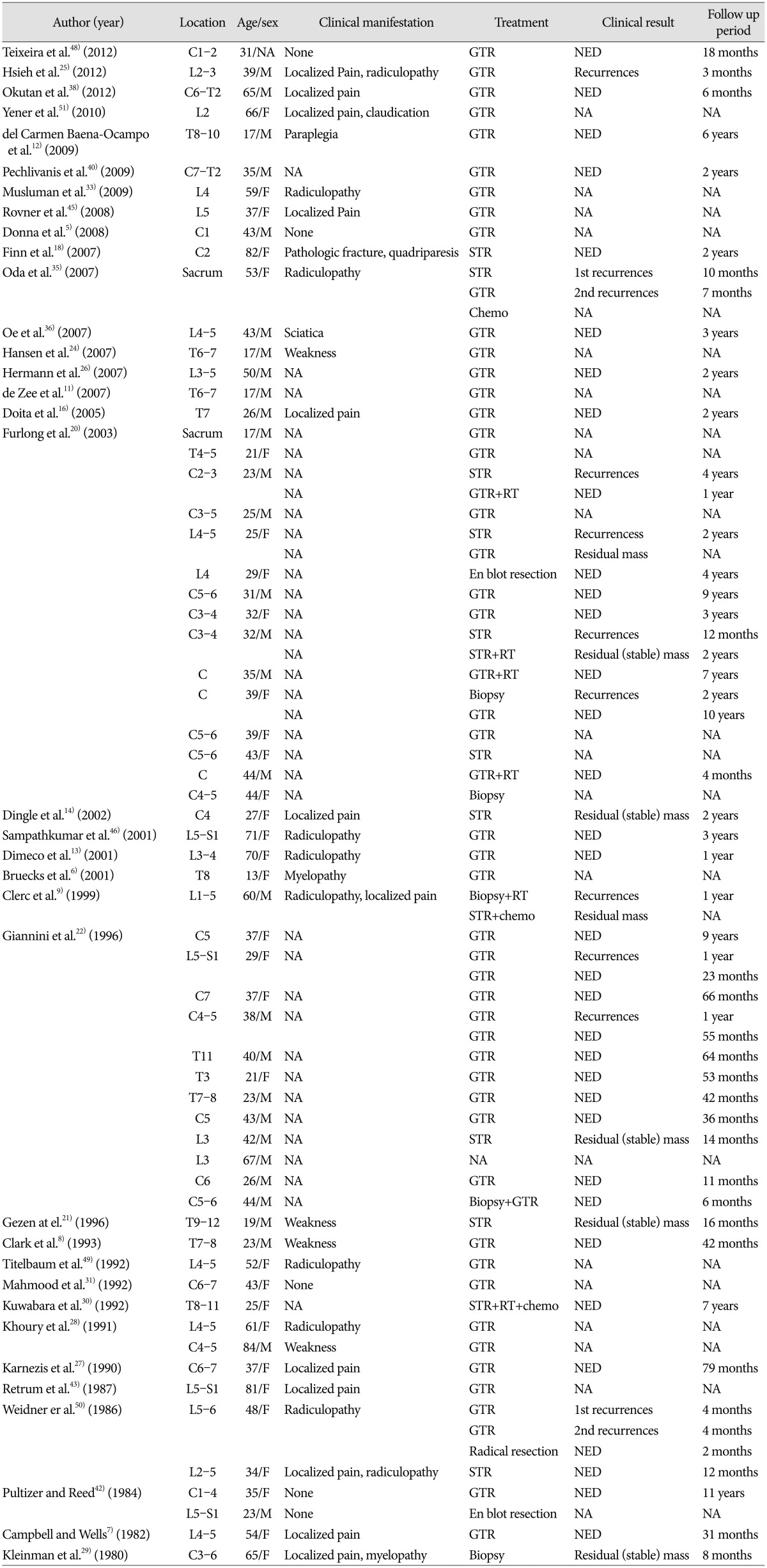
We reviewed 63 cases of spinal PVNS reported in the English literature (Table 1). Median patient age was 37 years (range, 13-84 years), and males were younger (35 years) than females (39 years). Twenty-eight cases (44.4%) were identified in the cervical spine, 12 cases (19%) in the thoracic spine and 21 cases (33.3%) in the lumbar spine. As the lesion origin facet joint mostly contains synovium, spinal PVNS is typically located in the posterior element20). Rare cases have been reported in which spinal PVNS arose from the atlantoaxial or atlantooccipital joints, which are a tendon sheath or synovial membrane containing joints, and not a facet joint5,18,20). Additionally, spinal PVNS involving anterior spinal structures has been reported22,42). It is thought to arise from synovial membranes of the vertebral column accessory joints. Pain localized to the spinal region is the most common symptom. As PVNS tends to arise from the posterior elements, it is often accompanied by radicular pain or myelopathic deficits6,20).
The pathological findings of PVNS in the appendicular skeleton and spine are similar28). However, PVNS of the spine often exhibits less pigmentation than that in the appendicular joint39). The histological appearance is characterized by a proliferation of synovial cells and includes lipid and hemosiderin-laden macrophages, multinucleated giant cells, mixed round cell infiltration, mononuclear polyhedral cells of fibrohistiocytic origin, and stromal and fibroblast cell proliferation4,10). Diffuse-type PVNS has greater vascularity, a greater number of hemosiderin-laden macrophages, and a typically villous pattern, which is often absent in localized PVNS34).
The best choice of diagnosis for PVNS is magnetic resonance imaging (MRI). MRI shows the mass as mixed signal intensity on T2-weighted images due to hemosiderin deposition and can reveal the extent of the lesion, bony erosion, and invasion. Differential diagnoses includes primary bone lesion, mesenchymal neoplasm and extradural masses, such as osteoblastoma, fibrohistiocytic tumor, schwannoma, hemangiopericytoma, tendinous xanthoma, and hypertrophic synovitis22).
The treatment goal for patients with PVNS is gross total excision of the mass with functional preservation and lowering of recurrence rate20). The local recurrence rate of spinal PVNS is 18-25% for all spinal cases22). It is similar with the rate of appendicular PVNS reported in different studies (0-50%)14,17,23,34). Various treatments for PVNS include surgery, radiation therapy, radioisotope infusions, and chemotherapy8,21,22,33,48). Surgical excision with the aim of gross total resection is accepted as the treatment of choice. However, after surgery, evidence is lacking concerning the need for adjuvant treatment to lower the recurrence rate as well as the standard protocol for recurrent PVNS. The extent of resection is currently the only known influence on recurrence rate20,22). Among the 63 cases we reviewed, only four of 46 patients (8.7%) who underwent gross total resection recurred, whereas four of 10 patients (40%) who underwent subtotal resection recurred (Table 1). Three patients received adjuvant chemotherapy and six patients received radiotherapy (RT). No recurrence was found for patients who received adjuvant chemotherapy, but one patient who received RT recurred. The efficacy of the treatment is unclear because there were an insufficient number of patients who received chemotherapy or RT. Therefore, surgical resection remains the treatment of choice for PVNS, unless chemotherapy or RT is a treatment option.
CONCLUSION
PVNS involving the spine is rare. The recommended method for treating spinal PVNS is gross total removal. No consensus has been reached regarding the efficacy of chemotherapy or RT as adjuvant treatment, because only a few cases have been presented. Therefore, surgical resection should be considered the first treatment for PVNS. More case studies of spinal PVNS are needed to clarify treatment following surgery.


 XML Download
XML Download