

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Aneurysmal subarachnoid hemorrhage (SAH) during pregnancy is quite rare, ranging from 0.01% to 0.05%, however, it is the third leading cause of maternal death from non-obstetric causes accounting for 5% to 12% of total mortality2,3). Due to high maternal mortality, management of an aneurysmal SAH in a pregnant patient should be the same as that for non-pregnant women22). In treatment of an aneurysmal SAH during pregnancy, the question of which treatment is optimal among surgical clipping and endovascular coiling is considered. And in the case of an endovascular approach, how to minimize radiation exposure to the mother and fetus is of the greatest importance. Some cases of successful endovascular treatment of a ruptured intracranial aneurysm in pregnant patients and good maternal and fetal outcome have recently been reported6,9,15,17,21).
We report on a case of a pregnant woman who presented with an aneurysmal SAH from a ruptured posterior inferior cerebellar artery (PICA) aneurysm which was treated safely by endovascular coiling with minimal radiation exposure. This case study reported the shortest gestational period (16 weeks) and it is the first report on an aneurysmal rupture that arose from PICA treated with endovascular coil embolization.
CASE REPORT
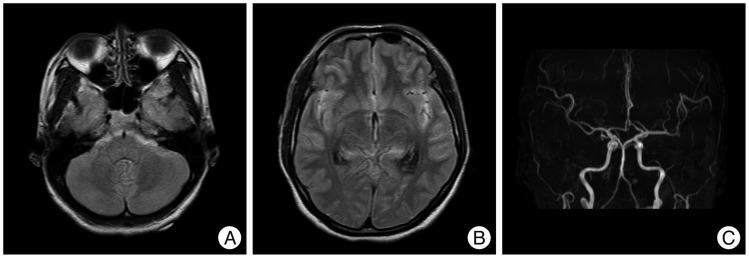
A 34-year-old woman in the 16th gestational week of her pregnancy presented to our hospital with a drowsy level of consciousness after experiencing a general tonic-clonic type seizure for 1 minute (Hunt-Hess grade 3). A brain magnetic resonance (MR) image examination showed a SAH with high signal intensity on the prepontine cistern, and both sylvian fissures on fluid attenuated inversion recovery image and MR angiography showed an aneurysm of the left PICA (Fig. 1).
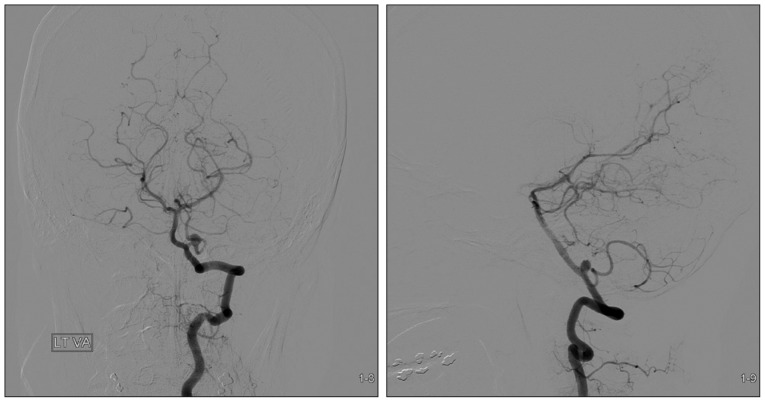
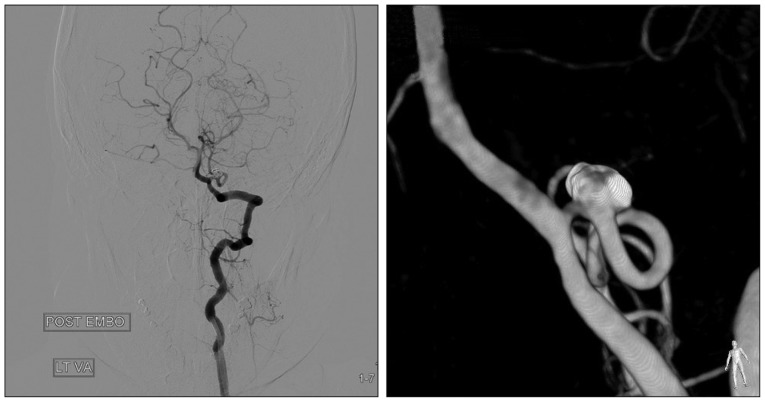
After shielding patient's lower abdomen with double-layered lead apron, cerebral digital subtraction angiography (DSA) was performed immediately. The patient's abdomen was shielded both anteriorly and posteriorly with double thickness of 0.5 mm lead aprons. Only the left vertebral artery angiogram demonstrated a sacular aneurysm of the neck measuring 4.08 mm, height 4.11 mm, and width 6.08 mm at the anterior medullary segment of the left PICA (Fig. 2). We decided on endovascular treatment because of the shape and location of the aneurysm and the patient's extraordinary situation, which was more suitable for endovascular embolization with coiling than the surgical obliteration. Using a double microcatheter technique, the aneurysm was totally occluded using five coils (total coil length was 16 cm; coil packing density was 18%). An angiogram revealed intact distal PICA flow and no residual sac (Fig. 3). Total dose area product (DAP) was 171370 mGycm2, air kerma (AK) was 1442 mGycm2 and total radiation time was 19 minutes 2 seconds (including both diagnostic and therapeutic DSA). The patient was transferred to the neurosurgical intensive care unit with no newly developed neurologic deficit and recovered from postictal mental deterioration. We did not use prophylactic anticonvulsants after coil embolization. She was discharged with no neurologic deficit and delivered a healthy baby by cesarean section at the 38th week of gestation due to premature rupture of membrane.
DISCUSSION
SAH from an intracranial aneurysm during pregnancy is a rare occurrence, affecting only 0.01% to 0.05% of the population2,3). The risk for recurrent bleeding during the remainder of pregnancy in patients with an untreated aneurysm is 33% to 50%16,19), with a maternal mortality rate of 50% to 68%1,2,16). In an analysis of 118 pregnant patients with an aneurysmal SAH, Dias and Sekhar3) reported an association of surgical treatment of a ruptured aneurysm with significantly lower maternal and fetal mortality rates than conservative treatment. Thus, management of an aneurysmal SAH in pregnant patients should be the same as in patients who are not pregnant4,8,11,20).
The treatment modality is determined by the location of the aneurysm, patient's condition, status of the fetus and surgical experience of the institute. Surgery of PICA aneurysmal SAH is still challenging because it was located in front of the brain stem and surrounded by the lower cranial nerves14). In spite of these technically difficulties, clinical outcome of surgery of PICA aneurysm was good in experienced hands13). But proximal PICA aneurysmal SAH is very rare and it could be a very difficult operation in less experienced surgeons. In these situations, surgical clipping may bring more poor result than coil embolization, especially in pregnancy patient. Higher risk of operation with excessive intraoperative blood loss, excessive mechanical ventilatory pressure and longer operation time could cause failure of controlling blood pressure and maintaining euvolemia, followed by decrease of uterine blood flow and transplacental oxygenation of the fetus9). In the other hand, use of endovascular techniques for treatment of aneurysms has been increasingly reported in pregnant patients, with good outcomes in both the mother and fetus6,15,18). In particular, in cases of posterior circulation aneurysms or unclippable lesions, endovascular coil embolization could be a better treatment method than surgery. International subarachnoid aneurysm trial also reported surgical clipping was relatively risky than endovascular coiling in the treatment of posterior circulation aneurysm10).
However, the endovascular treatment is based on angiography, and it has an inherent disadvantage. Angiography during pregnancy has the potential risk of fetal abnormalities resulting from radiation exposure. However, radiation effects are highly dependent on the amount of radiation absorbed and on the stage of fetal development at the time of radiation exposure5). The probability of radiation damage increases with increasing absorbed dose. Radiation risk is the highest during organogenesis and the early fetal period, somewhat lower in the second trimester, and the lowest in the third trimester5). During embryogenesis (first two weeks of pregnancy), radiation damage may result in the death of the embryo. During organogenesis (weeks 2 through 7 of gestation), radiation damage may result in congenital abnormalities in the surviving fetus5). The fetal period (week 8 until birth) is characterized by growth and development of the fetus5). Radiation risk during the fetal period includes growth retardation with microcephaly, retardation due to neuron depletion, and development of childhood cancer5). During the period from eight to 25 weeks, the central nervous system (CNS) is particularly sensitive to radiation, with the greatest sensitivity at eight to 15 weeks after conception5). The CNS is less sensitive to these effects at 16 to 25 weeks of gestational age and rather resistant after that5).
Possible hazards of X-ray exposure during pregnancy have been evaluated by the International Commission on Radiation Protection (ICRP). However, there was no specific dosimetric result during cerebral angiography with regard to exposure of the fetus5). According to the reference, fetal doses in excess of approximately 100 mGy may result in a verifiable decrease of intelligence quotient at eight to 15 weeks gestation5). During the same period, fetal doses in the range of 1000 mGy (1 Gy) result in a high probability of severe mental retardation5).
Recent modifications of angiographic techniques, such as abdominal shielding, limited fluoroscopy in proximity to the uterus, and the use of advanced imaging equipment can significantly limit the amount of radiation9). The abdomen should be shielded both anteriorly and posteriorly. The use of double thickness of 0.5 mm lead aprons, may reduce the received dose by more than 97%12). And, according to the report by Kuon et al.7), with optimized lead shielding, radiation exposure reduced to 0.8% of typical scatter entrance skin AK. In our case, total DAP of the procedure was 171370 mGycm2 and the AK was 1442 mGycm2. According to the previous reports, calculated expected value of the fetal dose was between 11.5 and 43.3 mGycm2. According to the ICRP, at exposure levels below 100 mGy, the radiation effect is so small that termination of pregnancy is not justified5). And, immediate post-procedural physical and ultrasound examinations of the fetus did not show any abnormalities. The patient was discharged after the procedures without any neurological complications. Close follow-up by her obstetrician confirmed the absence of deformities and she delivered a healthy baby at 38 weeks of pregnancy.
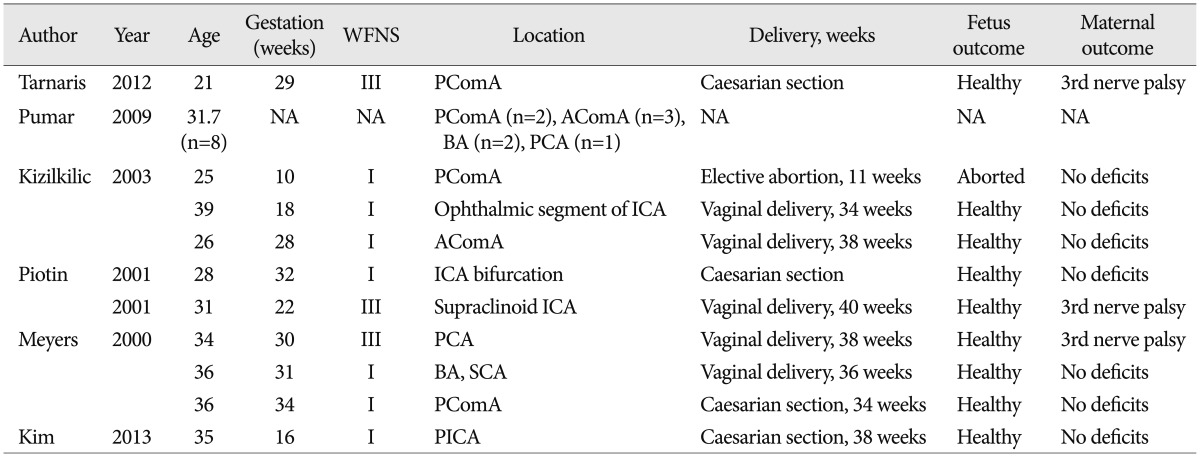
Several authors have reported successful endovascular treatment of a ruptured intracranial aneurysm, similar to our own (Table 1)6,9,15,17,21). The mean maternal age was 31.4 years (21-39, 31.4±4.3 years) and the mean gestation period was 25.0 weeks (10-34, 25.0±8.0 weeks). Posterior communicating artery was the most common site in five cases (5/18, 27.8%) and a posterior circulation aneurysm was found in five cases (27.8%). Third trimester was the most common in six cases (60%), and second trimester was the next in three cases (30%). Coil obliteration in the second trimester could be performed without procedure related complication and it has shown good results for both mother and fetus with optimized lead shielding and minimal radiation exposure. One first trimester fetus was electively aborted due to the risk of radiation. After obliteration of the aneurysm, the ratio of natural vaginal delivery and caesarean section were similar (vaginal delivery:caesarean section=4:5).
CONCLUSION
This case study reported the shortest gestational period (16 weeks) and it is the first report on an aneurysmal rupture arising from PICA treated with endovascular coil embolization. Our early experience and with other preliminary reports indicates that pregnant women (more than second trimester) can be treated successfully for a ruptured intracranial aneurysm using an endovascular approach. If the situation is expected to be associated with an increased fetal risk because the surgery takes a long time and the surgery has a highly morbidity, use of an appropriate technique for reduced radiation exposure to the fetus and limited alterations in maternal-fetal physiology, endovascular treatment could guarantee good results.
 XML Download
XML Download