

 PDF
PDF ePub
ePub Citation
Citation Print
Print


This letter discusses the article2) entitled "Delayed unilateral soft palate palsy without vocal cord involvement after microvascular decompression for hemifacial spasm" recently published in J Korean Neurosurg Soc 53 : 364-367, 2013.
In order to prevent cranial nerve palsies during microvascular decompression for hemifacial spasm, it is important to avoid retracting the cerebellum from the internal to the external side. Instead, it should be retracted from the lower to the upper side to obtain the optimal exposure of lower cranial nerves and the facial nerve root exit zone (FNREZ). The author of this manuscript devised an arachnoid dissection technique to expose the lower cranial nerves and the FNREZ.
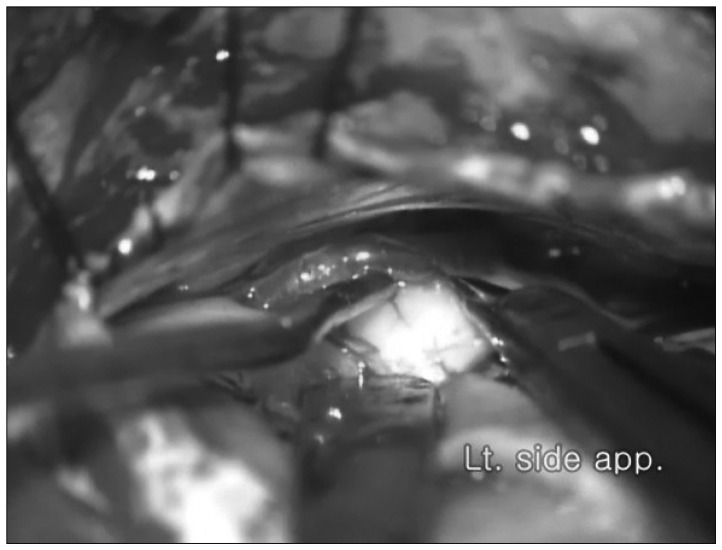
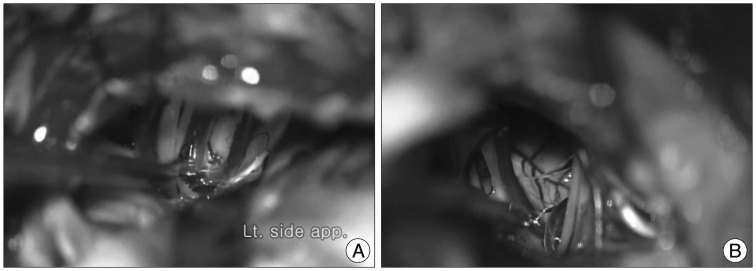
The retromastoid approach is most commonly conducted in the lateral decubitus position. The dura mater is incised along the sigmoid sinus, and the Cisterna magna is opened to drain the cerebrospinal fluid after careful retraction of the cerebellum from the lower to the upper side. The cerebellar cortical branches of the anterior inferior cerebellar artery (AICA), which is covered with an arachnoid membrane exterior to the lower cranial nerves, are exposed. Under the microscope, the outside of the arachnoid membrane is attached to the pia mater of the cerebellar cortical braches of AICA, which is dissected using an arachnoid knife and microscissors. At this point, the inner side of the arachnoid membrane of the cerebellar cortical braches of AICA should be preserved (Fig. 1). Next, the space between the cerebellar cortical braches of AICA and the cerebellar cortex is separated, and the sharp continuous arachnoid membrane dissection is extended towards the anterior and inferior end of lower cranial nerves modified by author's technique (Fig. 2)1). The cerebellar cortical branches of AICA are then retracted naturally towards the tentorium, and the choroid plexus, located in the lateral recess of the 4th ventricle, can be visualized. The offending artery and entire set of lower cranial nerves, facial nerves, including the FNREZ, can then be widely exposed (Fig. 3).
I think the significance of this arachnoid dissection procedures can prevent the lower cranial nerve palsies and also helpful to avoid cerebellar ischemia resulting from cerebellar cortical arterial compression/retraction during the operation.

 XML Download
XML Download