

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The process of brain injury disability evaluation (DE) requires retrospective assessment involving the severities of brain injuries at the initial stage, the process and outcome of medical treatments, and the association between objective medical data and self-reported vague and multiple symptoms. Objective data can easily be obtained from the former two evaluations. However, vague reports of symptoms, such as Post-Concussion Syndrome (PCS) after a traumatic brain injury (TBI), are not reliable and may be debatable, particularly in the context of medico-legal or compensation issues1). The DE of mild TBI patients is particularly complicated, and in the absence of medical records associated with mild TBI, related symptoms of PCS are reported frequently.
Brain injury occurs along a continuum of severity. Injuries with a loss of consciousness of less than 30 minutes, Glasgow Coma Scale (GCS)24) scores of 13 or greater, Post Traumatic Amnesia of no more than 24 hours, and other neurological signs are usually considered consistent with mild TBI6). The acute condition in mild TBI displays a cluster of neurocognitive dysfunctions, such as attention deficits, impaired verbal retrieval, and forgetfulness. Other problems, most notably headaches, dizziness, irritability, drowsiness, sleep disturbance, and fatigability are also very common sequelae. Many studies have reported that two-thirds of persons who sustained mild TBI return to their premorbid occupations and perform their usual activities within the first three to six months after an accident12). However, a significant group of patients may report PCS, which comprises a constellation of symptoms in the physical, cognitive, and emotional domains that persist for weeks, months, and even years after a mild TBI diagnosis20). Strictly applied, the term "mild TBI" refers to the initial injury severity and it should not be interpreted unequivocally as suggesting mild outcome severity. It may be more accurate to describe PCS as a commonly co-occurring symptom rather than as a syndromal sequela of TBI1). Although there is uncertainty over how and why mild TBI leads to PCS, what is clear is that the acute indicators of injury severity, and concomitant neurocognitive dysfunction, may be important considerations in understanding later presentation of PCS symptoms27).
Figures on the annual incidence of mild TBI are extremely elusive, because of the practices, procedures, and priorities inherent to the medical examination of physical injuries. Obvious signs of gross injuries direct the treating professional's attention to life- and health-threatening conditions, resulting in a de facto lack of emphasis on injuries to the head that are not readily apparent. In addition, the symptoms of a head injury can easily be overlooked and attributed to an emotional reaction to the situation16). In this condition, the true effects of mild TBI or PCS are newly developed symptoms because of the adjustment difficulties that occur after a physical injury and/or a psychiatric symptom for compensation.
Among PCS symptoms, twelve months after an injury, 31% of patients reported a psychiatric disorder, and 22% developed a psychiatric disorder that they had not experienced before. Functional impairment, rather than mild TBI, was associated with psychiatric illness. Although it is understandable that patients with psychiatric disorders may want to seek compensation, there is a possibility that this may contribute to patients reporting the presence of a psychiatric illness3). Non-organic factors, including pre-morbid personality traits and post-injury psychological reactions to disability and trauma, are also implicated in the generation and maintenance of a post-TBI psychiatric disorder. There is insufficient evidence to fully determine the role that the neuropathological consequences of TBI play in the development of post-TBI psychiatric disorders19) and other studies have concluded that neuropsychological test results coupled with self-reported symptoms should not be taken as the primary source of evidence for mild TBI, and prolonged cognitive impairment after an injury is not unique to brain trauma18).
DE is a scientific and medical decision-making process, but a scientist must engage in fair, impartial and public decision-making and accept the legal responsibility pertaining thereunto21). An evaluation of neurocognitive dysfunction in patients with MTBI is more objective than an evaluation of emotional or psychiatric symptoms using formal, officially approved, and published standard tests. However, emotional or psychiatric evaluations are dependent on a subjective interview, self-rating inventory, and a projective test; these may lead to scientific argument and disagreement, and could cause other complications.
Furthermore, neurocognitive dysfunctional symptoms and emotional or psychiatric symptoms are interrelated to each other. We therefore investigated how in a DE situation, the neuropsychological performance of patients with mild TBI and psychopathological characteristics are interrelated, and assessed which variable was most influential in the psychopathological characteristics associated with neuropsychological performance among patients with mild TBI.
MATERIALS AND METHODS
Subject selection, classification, and verification procedures
A total of 1245 patients, with ages ranging from 18 to 80 years old, and who received hospital or ambulant treatment for a brain injury from July 1998 to May 2010 were recruited. After excluding patients who had a neurological abnormality before their brain injury, a secondary head trauma, psychiatric disease, mental retardation, or a history of a chronic disease in the preceding six months, as well as those who did not complete the neuropsychological tests due to serious brain damage, 725 participants remained. Of these, 219 disability evaluation participants with mild brain injury (GCS score 13-15) were selected. These participants were classified into three group, based on their psychopathological characteristics via a two-step cluster analysis using validity and clinical scales taken from the Minnesota Multiphasic Personality Inventory (MMPI)9) and the Symptom Checklist-90-revised (SCL-90-R)9).
Classification method of participations was based on an objective statistical classification method for excluding subjective selecting bias by researchers, and then for validating classification processes, classified groups were compared with each other on used variables for the classification. In two-step clustering, to make large problems tractable, in the first step, cases are assigned to "preclusters." In the second step, preclusters are clustered using the hierarchical clustering algorithm. This method has advantage that researcher can specify the number of clusters you want or let the algorithm decide based on preselected criteria15). As results, participants were classified to 3 groups, and there were 59 patients (26.9%) in group 1, 95 patients (43.4%) in group 2, and 65 patients (29.7%) in group 3, and statistical characteristics of classifying variables at MMPI and SCL-90-R among 3 groups were described at results.
Materials
Korean Wechsler Adult Intelligence Scale (K-WAIS)25,28)
The K-WAIS is psychometric instrument that assesses the potential ability to perform a useful behavior for a certain purpose based on standardized questions and tasks.
Korean Memory Assessment Scale (K-MAS)10,26)
The MAS is a comprehensive, standardized memory assessment battery, which is designed to fulfill ordinary clinical assessment needs in a manner that is suitable for various kinds of clinical situations and demands12).
Symptom Checklist-90-revised (SCL-90-R)4,7)
The SCL-90-R is a self-report symptom inventory. It can be used as a primary tool to recognize persons who are in need of professional help. It also has the capability of covering a patient's general symptoms.
Minnesota Multiphasic Personality Inventory (MMPI)9)
The MMPI is an instrument that objectively measures abnormal behavior. Its primary purpose is for psychiatric diagnostic classification but it is also widely used to assess the mental functioning and personality of patients with brain damage.
Statistical analysis
We performed data processing from the chart reviews using SPSS (MS Windows Release 19.0). Post hoc analyses included frequency analysis (χ2 and Fisher exact tests), two-step cluster analysis, mean difference analysis (one-way ANOVA), and post hoc test (Bonferroni method). Correlational analysis and stepwise multiple regression analysis was used for analyzing relationship psychopathologic characteristics and cognitive function among the clustered mild TBI groups. We considered results to be significant at the p<0.05 level.
RESULTS
Demographic and clinical factors of participants
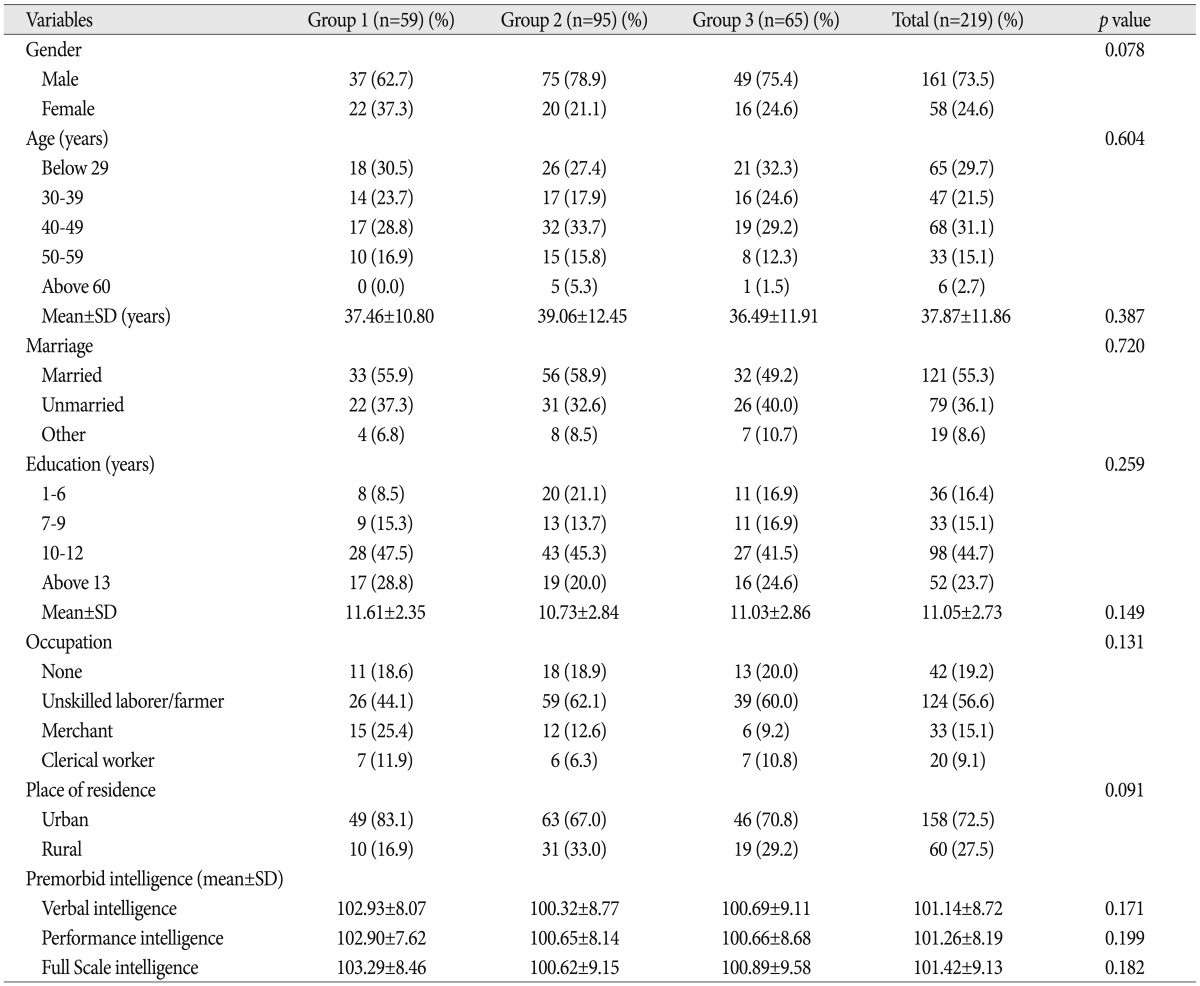
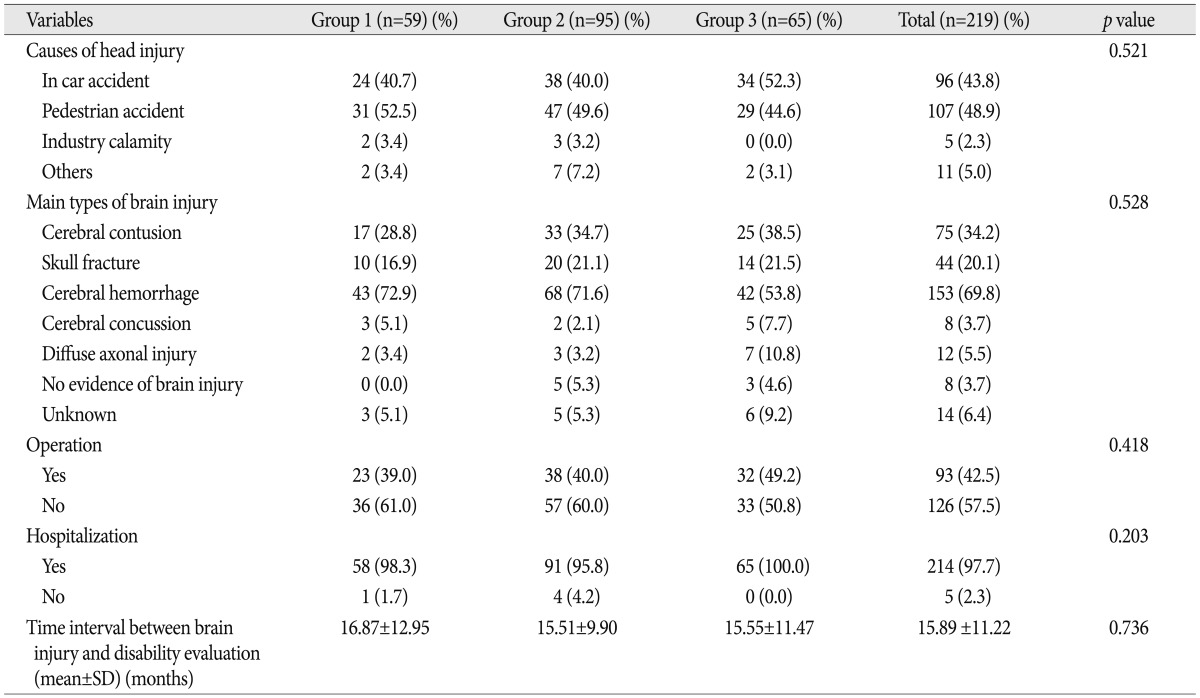
The demographic characteristics of the TBI subjects are presented in Table 1. The TBI subjects were predominantly male (n=161, 73.5%) with a mean age of 37.87±11.86 years. The majority were married (n=121, 55.3%), had an average formal education length of 11.05±2.73 years, and resided in an urban area (n=158, 72.5%). Occupational status at the time of injury was as follows: unskilled laborer/farmer (n=124, 56.6%); unemployed (n=42, 19.2%); merchant (n=33, 15.1%); and clerical worker (n=20, 9.1%). There were no statistically significant differences between the groups in the distributions of these demographic characteristics or in estimates of premorbid intelligence. The clinical characteristics of the total and classified 3 TBI groups are presented in Table 2. The causes of TBI were traffic accident while in a vehicle (n=96, 43.8%), traffic accident as a pedestrian (n=107, 48.9%), industry calamity (n=5, 2.3%), and violence by others, self-injury, and other (n=11, 5.0%). The types of head trauma were cerebral hemorrhage (n=153, 69.8%), cerebral contusion (n=75, 34.2%), skull fracture (n=44, 20.1%), unknown (n=14, 6.4%), diffuse axonal injury (n=12, 5.5%), cerebral concussion, and no evidence of brain injury (n=8, 3.7%). Surgery on brain injury was performed in 42.5% (n=93) of the patients, and 97.7% (n=214) were hospitalized. Time interval between brain injury and disability evaluation was 15.89±11.22 months.
Comparisons of the psychopathological characteristics between cluster groups
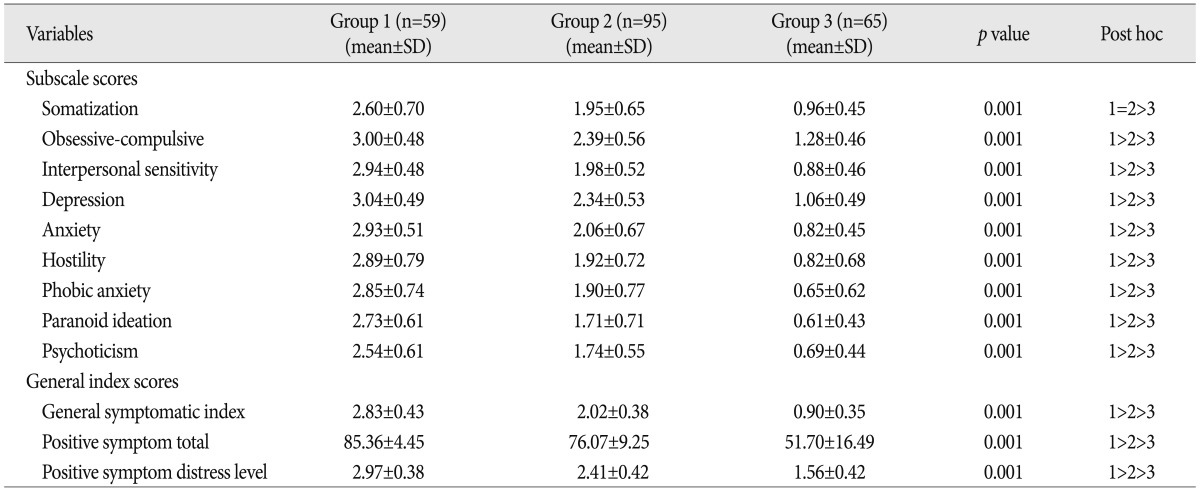
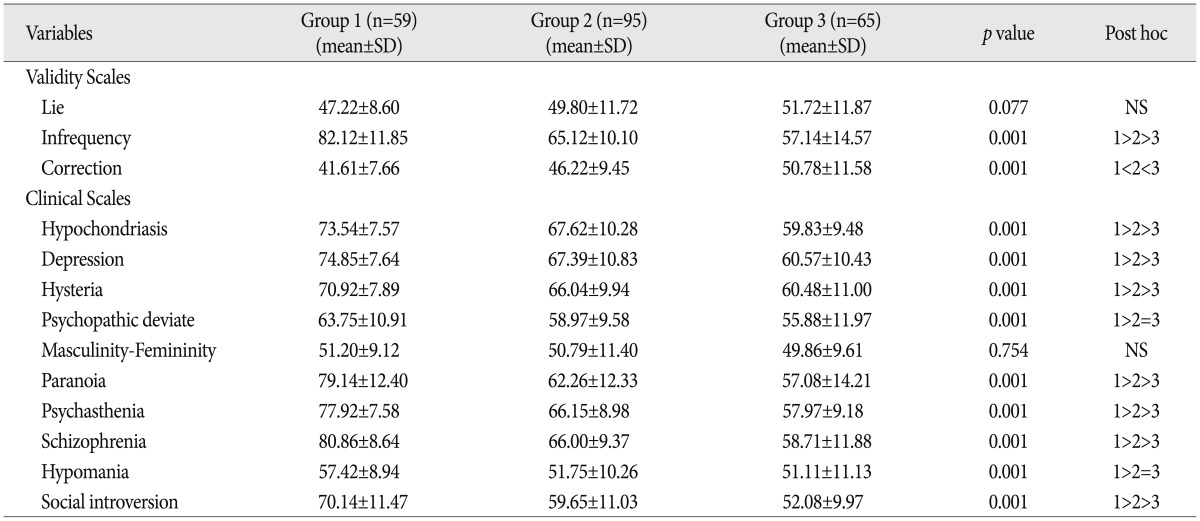
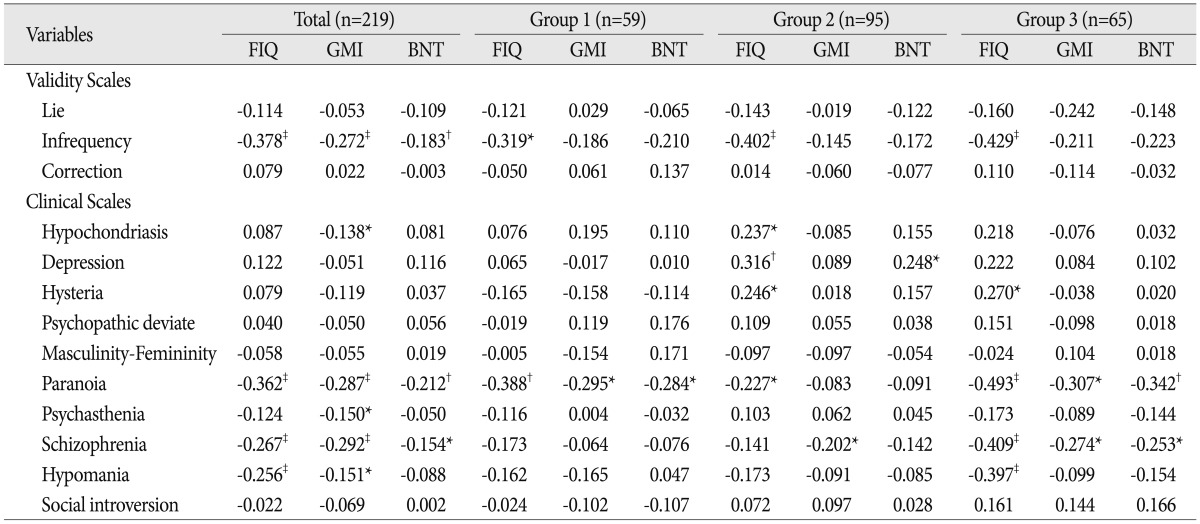
Table 3, 4 display summaries of the psychopathological characteristics of the cluster mild TBI groups. In SCL-90-R score analyses, there were significant differences between groups in all of the subscale and the general index scores. In post hoc tests, Group 1 was significantly higher than the other groups and Group 2 was significantly higher than Group 3 on all subscale scores except for Somatization, and General index scores (p<0.05). On the other hand, Group 1 and Group 2 were significantly higher than Group 3 in Somatization in MMPI score analyses. On the Validity scales, there were significant differences between the three groups in Infrequency (p<0.01) and Correction (p<0.01), but not for Lie. There were significant differences between the three groups on the clinical scales except for Masculinity-Femininity. In post hoc tests, Group 1 was significantly higher than the other groups and Group 2 was significantly higher than Groups 3 on Infrequency (p<0.05). In Correction, on the other hand, Group 1 was significantly lower than the other groups and Group 2 was significantly lower than Group 3 (p<0.05). In Hypochondriasis, Depression, Hysteria, Paranoia, Psychasthenia, Schizophrenia, and Social introversion among clinical scales, Group 1 was significantly higher than the other groups and Group 2 was significantly higher than Group 3 (p< 0.05). On the other hand, only Group 1 was significantly higher than the other groups in Psychopathic deviate and Hypomania (p<0.05).
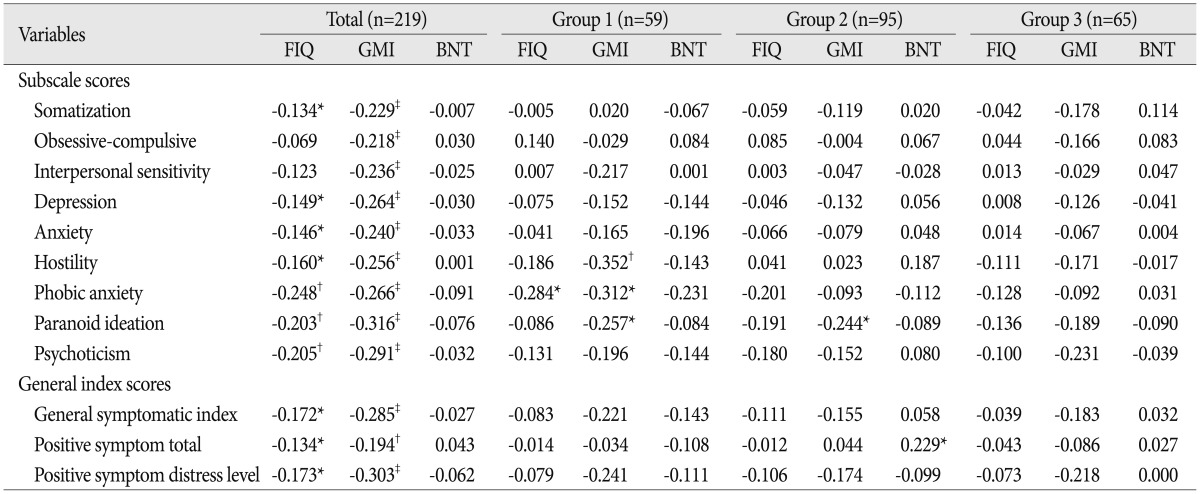
The relationship between psychopathologic characteristics and intelligence and cognitive functions
Table 5, 6 show summaries of correlational analysis and step-wise multiple regression analysis results between psychopathologic characteristics in SCL-90-R and the intelligence and cognitive functions. All of the mild TBI patients showed a significant relationship between subscale scores and almost all cognitive function scores, including full scale intelligence quotient (FIQ) and general memory index (GMI). However, the degree of significant correlation was below 0.4 and percentile scores on the K-BNT did not showed any significant relationship. FIQ variance was explained 9.3% by Phobic anxiety (ΔR2=0.061, p<0.001), Obsessive-compulsive (ΔR2=0.027, p<0.01), and Psychotism (ΔR2=0.018, p<0.05) whereas GMI was explained 10.0% by Paranoid ideation (R2=0.100, p<0.001).
FIQ variance in Group 1 was explained 8.1% by Phobic anxiety (R2=0.081, p<0.05) and GMI was explained 12.4% by Hostility (R2=0.124, p<0.01). In Group 2, variance in GMI was explained 5.9% by Paranoid ideation (R2=0.059, p<0.05) and BNT was explained 9.5% by Positive symptom total (ΔR2=0.053, p<0.05) and Phobic anxiety (ΔR2=0.042, p<0.05). Group 3 showed no significant relationships between psychopathological characteristics and cognitive function on the SCL-90-R subscales.
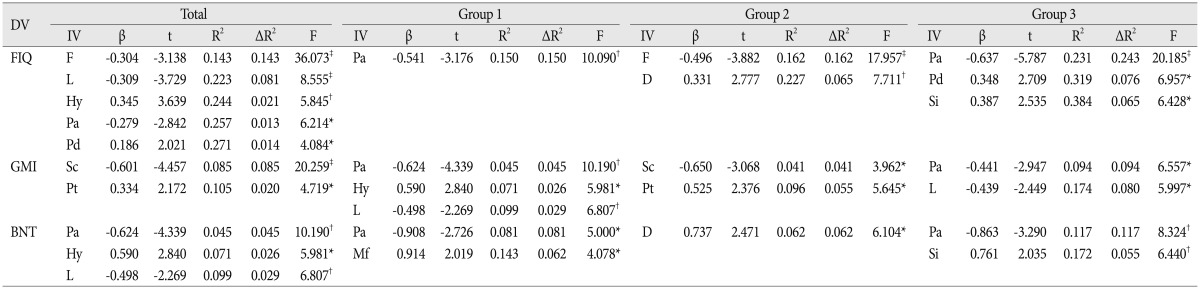
Table 7, 8 show summaries of correlational analysis and stepwise multiple regression analysis results between the psychopathologic characteristics of the MMPI and the intelligence and cognitive functions. All of the mild TBI patients showed a significant relationship between FIQ and some scales of the MMPI and variance in FIQ was explained 27.1% by Infrequency (ΔR2=0.143, p<0.001), lie (ΔR2=0.081, p<0.001), Hysteria (ΔR2=0.021, p<0.01), Paranoia (ΔR2=0.013, p<0.05) and Psychopathic deviate (ΔR2=0.014, p<0.05); GMI was explained 10.5% by Schizophrenia (ΔR2=0.085, p<0.001) and Psychasthenia (ΔR2=0.020, p<0.05), and BNT was explained 9.9% by Paranoia (ΔR2=0.045, p<0.01), Hysteria (ΔR2=0.026, p<0.05), and Lie (ΔR2=0.029, p<0.01).
Variance in FIQ in Group 1 was explained 15.0% by Paranoia (R2=0.150, p<0.01); GMI was explained 9.9% by Paranoia (ΔR2=0.045, p<0.01), Hysteria (ΔR2=0.026, p<0.05) and Lie (ΔR2=0.029, p<0.01), and BNT was explained 14.3% by Paranoia (ΔR2=0.081, p<0.05) and Masculinity-Femininity (ΔR2=0.062, p<0.05). In Group 2, a variance of FIQ was explained 22.70% by Infrequency (ΔR2=0.162, p<0.001) and Depression (ΔR2=0.065, p<0.01); GMI was explained 9.6% by Schizophrenia (ΔR2=0.041, p<0.05) and Psychasthenia (ΔR2=0.055, p<0.05), and BNT was explained 6.2% by Depression (R2=0.062, p<0.05). In Group 3, FIQ variance was explained 38.4% by Paranoia (ΔR2=0.243, p<0.001), Psychopathic deviate (ΔR2=0.076, p<0.05) and Social introversion (ΔR2=0.065, p<0.05); GMI was explained 17.4% by Paranoia (ΔR2=0.094, p<0.05) and Lie (ΔR2=0.080, p<0.05), and BNT was explained 17.2% by Paranoia (ΔR2=0.117, p<0.01) and Social introversion (ΔR2=0.055, p<0.01).
Comparisons of intelligence and cognitive functions between groups
Table 9 shows summaries of FIQ, GMI and BNT score analyses. There were significant differences between the three groups on GMI (p<0.01), but no significant differences on FIQ and BNT. In post hoc tests, Group 3 had significantly higher scores than Group 1 on the GMI.
DISCUSSION
The majority of cases that are encountered in the forensic arena are individuals who may have sustained TBIs. Within TBI, mild TBIs comprise well over half of all reported cases. Many of these injuries occur due to motor vehicle accidents, and the majority of patients with mild TBI are young men between the ages of 16 and 35 years21). In this study, the mean age of patients with mild TBI was 37.8 years and 92.9% of these subjects were involved in a traffic accident, either in a vehicle or as a pedestrian, and all the patients underwent DE to assess the compensation level needed for their injuries. Their ages are older than the above study would suggest, but younger than those in a study that included non-DE patients5), and almost all of them (80.8%) were employed. A younger age and a diagnosis of mild TBI may be causes of complicated PCS and issues related to malingering. Although younger age is a good prognostic factor in brain injury5), we consider that it may also be a psychogenic stress factor as the economic burden or responsibility is likely to fall on these patients as the head of a family. Almost all the patients with mild TBI in this study had external incentives to malinger and displayed definite or probable malingered neurocognitive dysfunction23). 40.3% of DE patients with mild and moderate brain injuries display typical or passive malingering patterns and behaviors, sometimes involving denial of symptoms and resistance to treatment22).
In this study, all of mild TBI patients showed a significant relationship between neurocognitive functions and subjective and/or objective psychopathic symptoms, but the degree of relationship was with the moderate range. Likewise, decrement or change of neurocognitive function was explained by psychopathologic symptoms related with psychotic symptoms indicated by an elevation of paranoia and schizophrenia scale scores on the MMPI, but neurotic symptoms as obsessive-compulsive, hypochondriac and depressive trends in mild TBI patient had a complementary function to decrements or impairments of neurocognitive function.
Our findings indicated that Group 1 showed a "faking-bad or crying-help" response tendency in the validity scales and severe psychopathological symptoms in the clinical scales of the MMPI and SCL-90-R, but they did not experience a severe intelligence decline compared to the other two groups except for their global memory abilities on the K-MAS. Severe and actual psychopathological problems can lead to a decrease in intelligence or intellectual efficacy, a deterioration of reality testing, premorbid adjustment problems, and depressed scores of comprehension abilities17). However, the mild TBI patients in this study had no psychiatric history, previous adjustment problems, severe TBI related objective physiological data resulting in personality change or impaired reality testing, and no full scale intelligence quotient decrement compared to the other two groups. This group is similar to DE patients in that both groups mainly simulate psychopathological symptoms using psychotic symptoms21). Furthermore, memory difficulties are common following head trauma of sufficient severity14), but attention span and immediate memory are relatively preserved in dementia due to head trauma11). The discrimination between malingered and head trauma profiles on the memory test rests on the tendency for head injured patients to do better and malingers to do more poorly on measures of attention relative to their performance on measures of memory13). Therefore, Group 1 showed malingered psychopathological symptoms as PCS, but they did not simulate cognitive decrement; they were inactive in terms of intelligence decrement or effortful malingering attempts. Group 2 showed fewer psychopathological symptoms than Group 1 but more than Group 3, respectively, but did not show cognitive decline compared to Group 3. In particular, Group 2 had showed lower scores of Psychopathic deviate and Hypomanic scales in MMPI than group 1, and did not showed significant difference with Group 3. A radical difference between Group 1 and Group 2 were not severity of psychopathologic symptoms, but behavioral or observable symptoms as impulse control or emotional instabilities, suggested. Group 3 displayed few psychopathological symptoms, but had lower cognitive function than the normal range. Scores of subscale at MMPI and SCL-90-R in Group 3 were approximately closed to an average score of normal population. It suggested that they never complained or experienced psychopathologic symptoms after mild TBI, or denied that symptoms. Some of patients with TBI denied concurrent psychiatric or psychopathological symptoms due to a false belief as that TBI is not curable injuries or an under-evaluation of status at self by lowered self-awareness ability21). In general psychiatric patients, decrements or impairments of some cognitive or neurocognitive functions are the main evidence of some psychiatric disorder in the diagnostic process. Most common neurotic disorders including depressive disorder and anxiety disorder cause psychomotor retardation, attention and concentration impairments, and multiple functional cognitive decrements. Furthermore, psychotic disorders such as schizophrenia cause severe cognitive decrements12). However, these results suggest that psychopathological symptoms are mainly related to global memory function, but that psychopathological symptoms are not directly related to cognitive decline, intelligence decline, or other domains. Furthermore, a real or a malingered and simulated decrement or impairment of neurocognitive function was related with psychotic symptoms, but neurotic symptoms were a positive complement to decrements or impairments of neurocognitive function.
CONCLUSION
In this study, we demonstrated a relationship between the neuropsychological performance of patients with mild TBI and their psychopathological characteristics assessed in the DE process. We examined the variables that influenced psychopathological characteristics in neuropsychological performance among patients with mild TBI via statistical clustering of the same characteristics in mild TBI. Certain patients with mild TBI displayed psychopathological symptoms, but these were not directly related to cognitive decrement, and psychopathology and cognitive decrement were discrete aspects in patients with mild TBI. Furthermore, the neurotic symptoms of mild TBI patients were a positive complements to decrements or impairments of neurocognitive functions, but psychotic symptoms had a negative effect on neurocognitive functions.


 XML Download
XML Download