

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The development of neurosurgical treatments has greatly improved recovery rates for patients with subarachnoid hemorrhage (SAH), and recent studies have focused on the management of neurological defects due to ischemic complications secondary to treatment for SAH. Cerebral vasospasm in ruptured SAH is an ischemic neurological complication observed four to nine days after hemorrhage in about 70% of cases13). Medical treatment including triple H (i.e., hypertension, hypervolemia, hemodilution), balloon angioplasty, and intra-arterial (IA) papaverine injections have been developed to prevent this complication2,9,26). Unfortunately, the effects of triple H are limited, and though balloon angioplasty has a continuous dilating effect on narrowed vessels, the procedure site is limited to proximal vessels, and the performer must be skilled and experienced14,24).
Papaverine, verapamil, and nimodipine are used for IA injections. The effects of these drugs are temporary, but they can be applied to narrow or distal vessels. Direct injection of papaverine into the cerebral arteries generally produces favorable results in diffuse cerebral vasospasm and distal microvascular dilation, but its effects are momentary, requiring continuous treatment6,15,17). Papaverine is also associated with a considerable number of adverse effects2,3,10).
Several studies have examined the effectiveness of IA nimodipine injection for the treatment of cerebral vasospasms, with two early studies reporting conflicting results. Böker et al.2) concluded that selective IA nimodipine was effective, while Grotenhuis et al.10) considered it ineffective. More recently, two studies have shown that IA nimodipine improves the clinical state and blood vessel diameter of patients who do not respond to other treatments1,11).
The purpose of this study was to determine the effectiveness of IA nimodipine injection in patients who experienced cerebral vasospasm after aneurysm clipping for ruptured SAH by examining changes in prognosis and blood vessel diameter in angiography before and after IA nimodipine injection.
MATERIALS AND METHODS
Among the patients at our hospital who underwent aneurysm clipping for ruptured cerebral aneurysms between March 2009 and April 2011, we enrolled 29 patients who received IA nimodipine after subsequently presenting with symptoms of delayed cerebral ischemia associated with vasospasm. The diagnosis of delayed cerebral ischemia was based on an aggravated level of consciousness and changes in neurological symptoms. For each patient, we determined the Hunt-Hess (H-H) grade and World Federation of Neurosurgeons (WFNS) SAH grade at hospitalization; the Glasgow Coma Scale (GCS) score before and after nimodipine injection; and the Glasgow Outcome Scale (GOS) score at discharge. In addition, Fisher grades were determined using brain computed tomography (CT) images to classify the degree of SAH for each patient. The transcranial Doppler (TCD) velocities of the middle cerebral arteries before and after angioplasty were measured, as well as the time interval between SAH and vasospasm, and the time interval between surgery and vasospasm.
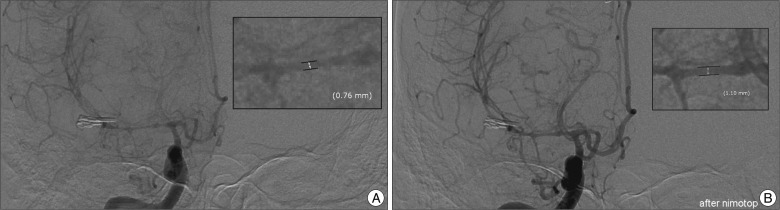
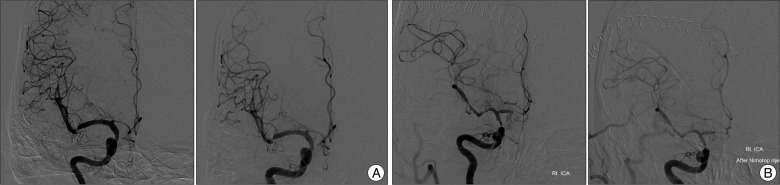
Cerebral angiography was performed when cerebral vasospasm was suspected. Angiographic vasospasm, known as a focal or generalized reduction of cerebral arterial caliber on conventional cerebral angiogram5), was measured in the narrowest region using caliper of the Picture Archiving and Communication System. Blood vessel diameters before and after nimodipine injection were measured on the 2-D image (Fig. 1), and the same individual (Kim) took all measurements to reduce bias. The treatment effects of nimodipine were assessed through angiographic changes in blood vessel diameter and improvements in neurological symptoms after the procedure. The level of vasodilation in the angiography results; middle cerebral arterial blood flow velocity changes before and after IA injection during TCD; and GCS scores before and after the procedure were compared to assess any improvement in symptoms.
Patients have received intravenous nimodipine injection after being diagnosed with SAH. Also, patients who were diagnosed with vasospasm based on angiographic features received additional IA nimodipine injection if they did not respond to the combination treatment of triple H and intravenous nimodipine. A dose of 5-15 mL nimodipine was prepared after dilution with 15-45 mL physiologic saline. Slow continuous infusion of the solution was achieved at a rate of 2 mL/min using an electric pump (nimodipine 0.1 mL/min). The dose of nimodipine infused intra-arterially was 1-3 mg per treated vessel. All 29 patients who had a lesion suspicious for vasospasm received a single IA nimodipine injection.
Data were analyzed with SPSS statistical software (version 12.0 for Windows; SPSS Inc., Chicago, IL, USA). Regression analyses were performed, for which we report R-Square values, t-values, and p-values. p-values <0.05 were considered statistically significant.
RESULTS
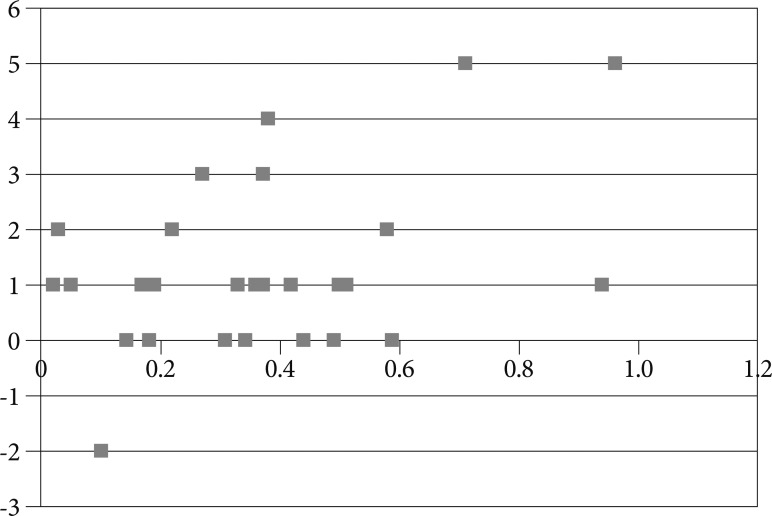
The 29 enrolled patients included 14 men and 15 women with an average age of 50.8 years (range, 32 to 64). At hospitalization, 7 patients had an H-H score of I; 7 patients had a score of II; 13 patients had a score of III; and 2 patients had a score of IV. The GCS scores at hospitalization ranged from 6-15 points. As determined by the brain CT scans, the radiologic grades for the amount of hemorrhage included 5 patients in Fisher group II; 13 patients in Fisher group III; and 11 patients in Fisher group IV. All patients received intravenous nimodipine injection after surgery. Triple H treatment and CT scans were performed when patients showed neurological deterioration in order to rule out other complications. When vasospasm was confirmed, angiography was performed. Patients received IA nimodipine injection when vasospasm was suspected based on angiographic features. The degree to which the cerebral arteries were dilated was determined through angiography after the IA nimodipine injection. The clinical improvement after IA nimodipine injection was assessed with the GCS to determine whether clinical symptoms improved within 96 hours. The spasms were graded as mild when the arterial narrowing was <25%; moderate when the arterial narrowing was 25-50%; and severe when the narrowing was >50%. The initial angiogram, which did not show any obvious vasospasm, was used as a reference by which the pre- and post-treatment angiograms were compared. Based on the degree of arterial narrowing observed in angiography, we determined that 5 patients had moderate spasms and 24 patients had severe spasms. The GCS scores before cerebral angiography ranged from 9 to 15, while the GCS scores after cerebral angiography and IA nimodipine injection ranged from 10 to 15. The GCS scores increased by two or more points for 8 patients; by one point for 13 patients; and were unchanged for the remaining 8 patients. The GCS scores after injection were either improved or identical to the GCS scores before injection, except in one patient. The GCS score for this patient decreased from 12 to 10, even though the vessel diameter increased by 0.1 mm (16%). The percentage of increase in diameter was 40% or more in eight patients; 30-40% in one patient; 20-30% in eight patients; 10-20% in eight patients; and less than 10% in four patients (Fig. 2). Regression analysis indicated that the change in GCS score after nimodipine injection was positively associated with the change in blood vessel diameter after injection; the power of the regression equation was 17.2% and the t value was 2.37 (p=0.025) (Fig. 3). A greater increase in diameter after nimodipine injection can be considered a relevant measure of clinical improvement, so it may be associated with the GCS score. However, regression analysis indicated that the GCS score at hospitalization was not significantly associated with the change in diameter after IA nimodipine injection (t=1.701; p=0.1).
The WFNS grade was 1 point in 14 patients; 2 points in 6 patients; 3 points in 7 patients; and 5 points in 2 patients. Regression analysis indicated that the H-H grade at hospitalization was positively correlated with the WFNS grade (p=0.001); the power of the regression equation was 57%, and the t-value was 5.978. Likewise, the Fisher grade at hospitalization was positively associated with the WFNS grade (p=0.002); the power of the regression equation was 30% and the t-value was 3.428.
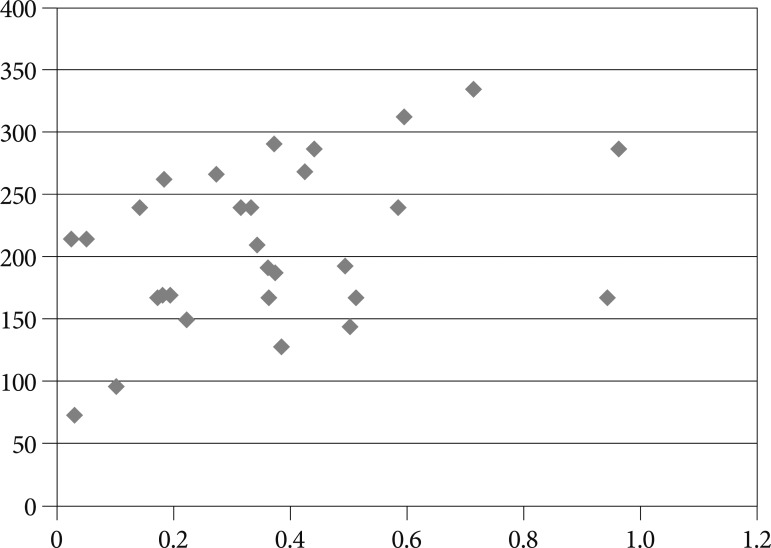
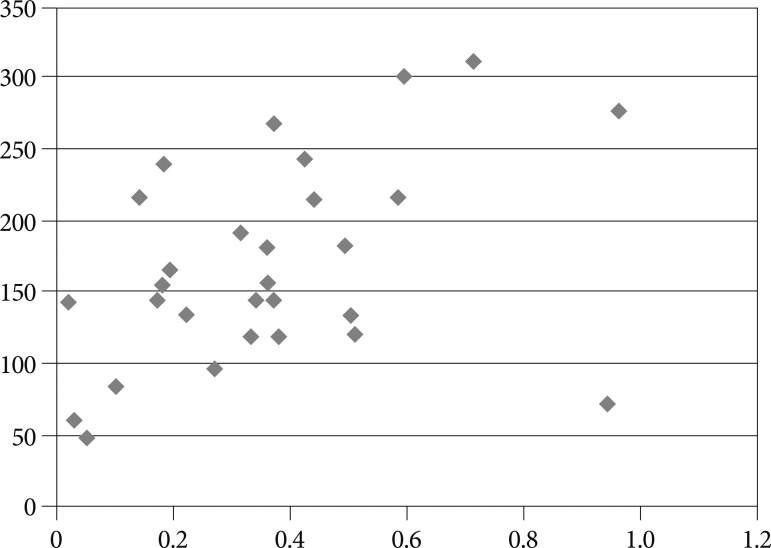
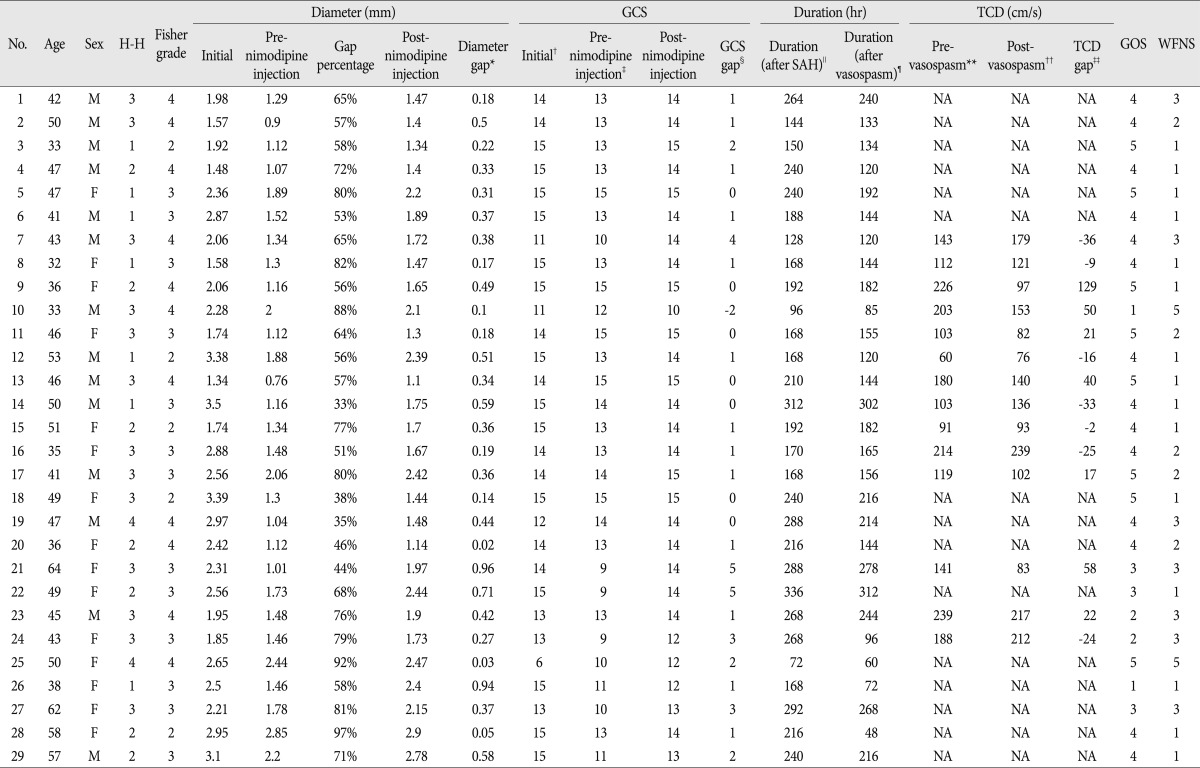
The average time interval from SAH to the occurrence of cerebral vasospasm was 8.75 days, while the time interval from aneurysm clipping to cerebral vasospasm was 6.87 days. The time interval from SAH to cerebral vasospasm was positively correlated with the change in blood vessel diameter after IA nimodipine injection (regression equation power=14.8%; t=2.163; p=0.040). Likewise, the time interval from aneurysm clipping to cerebral vasospasm was positively correlated with the change in blood vessel diameter after IA nimodipine injection (regression equation power=17.8%; t=0.2422; p=0.022). Thus, as the time interval increased between SAH or clipping and vasospasm, the blood vessel diameters increased more after IA nimodipine injection (Fig. 4, 5). The patients who received TCD were included in a regression analysis examining the relationship between changes in TCD velocity and blood vessel diameter. The t value was 0.796 (p=0.441). With regards to the final treatment results, 8 patients had a GOS score of 5; 14 patients had a score of 4; 3 patients had a score of 3; 2 patients had a score of 2; and 2 patients had a score of 1. The H-H grade was not significantly correlated with the GOS scores of patients at hospitalization (regression analysis, t=-0.048, p=0.962), and the Fisher grade was not significantly correlated with the GOS scores of patients at hospitalization (regression analysis, t=-0.673, p=0.507). The GOS score was negatively correlated with the change in blood vessel diameter after IA nimodipine injection, though this difference was not statistically significant (regression analysis, t=-1.947, p=0.062). Table 1 summarizes the clinical data of 29 cases treated with intra-arterial nimodipine injection.
There were no adverse effects, such as prolonged hypotension, worsening vasospasm, bradycardia, rash, or diarrhea, associated with IA nimodipine injection. The GCS score for one patient decreased after IA nimodipine injection. This patient had a hemorrhage on the post-operative brain CT that was not present prior to aneurysm clipping. The hemorrhage on the follow-up CT scan became larger after IA nimodipine injection.
DISCUSSION
Previous studies have suggested that nimodipine has direct neuron-protective effects, such as defending against oxidizing substances that impede the mitochondria within neurons; enhancing reactivation of carbon dioxide and oxygen metabolism in brain cells; and reducing brain tissue damage due to calcium overload during cerebrovascular reperfusion16,18,21,23). Intravenous nimodipine injection after SAH has been reported to reduce symptoms of secondary delayed cerebral ischemia and improve prognosis. However, the mediating factors responsible for the effects of nimodipine have yet to be clarified. The rate of vasospasm-related permanent disability is estimated to be about 10% to 20%4,22).
For symptomatic vasospasm refractory to hemodynamic therapy, endovascular strategies such as balloon angioplasty7) and IA spasmolysis with papaverine12) or nimodipine1) have been recommended. Balloon angioplasty is effective, but the procedure is limited to proximal vessel segments. It is also associated with significant risk and requires an experienced endovascular surgeon19,24). As determined by TCD analysis, IA papaverine can reverse angiographic vasospasm and reduce blood flow rates8,12), but clinical trials have failed to demonstrate an effect of IA papaverine on outcome20), most likely because the effects of papaverine are limited to only a few hours27). Unfortunately, the complications of balloon angioplasty and IA papaverine injection are on the rise as more patients with severe vasospasm undergo these procedures2,3,10).
In our study, the effects of IA nimodipine injection were assessed based on vessel extensibility in angiography and improvement in clinical symptoms. Among the 29 patients with symptomatic vasospasm, 24 (82%) demonstrated at least a 10% improvement in vessel extensibility. Likewise, GCS scores increased in 21 patients, remained the same in 7 patients, and decreased in 1 patient. Most patients showed vasospasm improvements on angiography performed immediately after IA nimo-dipine injection. However, there was one case in which the GCS score decreased even though vasodilation was clearly observed after nimodipine injection. It is possible that hemorrhage extension was responsible for the neurological deterioration of this patient.
The degree of brain tissue damage due to ischemia is related not only to the intensity of ischemia but also to its duration. In this study, as the time interval between SAH and vasospasm increased, the degree of improvement in blood vessel diameter also increased. Similar results were obtained for the time from surgery to vasospasm and the increase in blood vessel diameter in angiography. These results suggest that the effects of nimodipine increase when vasospasm occurs later in time relative to SAH or surgery.
We performed cerebral angiography when patients had clinical symptoms of delayed cerebral ischemia, even when there were no definite intracranial lesions on the brain CT scans; or if vasospasm was suspected despite active triple H treatment performed when the mean blood flow velocity of the middle cerebral artery was enhanced in TCD. Nimodipine was injected when vasospasm was confirmed by cerebral angiography. In the TCD performed after nimodipine injection, 7 of the 14 patients who received TCD before and after nimodipine injection experienced a decrease in blood flow velocity. Although vasodilation in angiography and clinical symptom improvements were observed, there was no obvious decrease in blood flow velocity in TCD. A number of previous studies have also indicated that the changes observed with TCD after nimodipine injection are unrelated to the radiological or clinical symptom improvements20,25,27).
Generally, it is difficult to approach lesions in the distal area with balloon angioplasty; this procedure is also technically difficult and associated with significant risks. Papaverine injection within the cerebral artery is reported to cause temporary neurological defects and crystal emboli1). However, such complications from IA nimodipine injection have not been reported. Known complications of nimodipine include prolonged hypotension, worsening vasospasm, bradycardia, rash, and diarrhea1), but none were observed in this study. Instead, the neurological status of one patient deteriorated after nimodipine injection, even though cerebral angiograms showed an increase in the patient's blood vessel diameter. Increased hemorrhagic contusion may explain the deterioration. It is unclear whether IA nimodipine injection could increase the size of the pre-existed hemorrhage. There has been no study showing a direct relationship between the increase of hemorrhage and IA nimodipine injection. Additional studies through a larger number of cases are required.
Several previous studies have examined the effectiveness of IA nimodipine injection, though conflicting results were reported in earlier work. Böker et al.2) concluded that IA nimodipine injection was an effective treatment for vasospasm after SAH, but Grotenhuis et al.10) reported that it was ineffective. More recent research by Biondi et al.1) and Hui and Lau11) indicates that IA nimodipine injection effectively dilates the blood vessels of patients with vasospasms that do not respond to other treatments. Thus, our results are consistent with most previous research.
Previous studies have examined whether clinical symptoms improve after IA nimodipine injection for vasospasm and whether improvements are evident on angiography. However, our study is the first to examine the relationship between the time to vasospasm and the effectiveness of IA nimodipine injection. Clinical symptom improvements were assessed with the GCS, and vessel diameter changes were measured by angiography. Interestingly, the recovery by IA nimodipine injection appeared to more improve when the time interval between SAH and vasospasm was longer. Thus, we concluded that the effects of nimodipine were better when the spasm occurred later in time relative to SAH and surgery. Although there has been no study reporting the clinical relevance of interval from the development of SAH to vasospasm and IA nimodipine injection up to this date, our results indicate that the time intervals may be helpful in predicting the patient prognosis after IA nimodipine injection.
Our study has some limitations. The sample size was relatively small, which could have led to statistical misinterpretation. We did not compare the results for patients undergoing IA nimodipine injection with those of a control group who were only treated with triple H and intravenous nimodipine. Due to the absence of a distinct control group, it is not clear whether the changes in GCS scores after IA nimodipine injection is due to a natural course or from nimodipine effects. Thus, further study that includes a control group would be necessary. In addition, we did not perform continuous TCD monitoring during the period of vasospasm before and after nimodipine injection, so it is possible that we underestimated the improvement after IA nimodipine since we only utilized TCD at one point in time. Another limitation of this study is that the patient group could not be selected consistently with H-H grade and Fisher grades since there were a small number of cases. This should be supplemented afterwards. Also, a long term follow-up was not performed since data was collected quite recently. Finally, a variety of factors could influence the outcomes of IA nimodipine injection, such as a patient's underlying disease or smoking status, so future studies should enroll a diverse subject population and utilize multivariate analyses to investigate this possibility.
CONCLUSION
In this study, patients who received IA nimodipine injection for cerebral vasospasm after ruptured SAH demonstrated improvements in blood vessel diameter and clinical symptoms in angiography. We also found a significant positive correlation between the degree of blood vessel expansion and the improvement in clinical symptoms. However, vasodilation and changes in TCD velocity were not significantly correlated. The time interval between SAH and vasospasm was significantly positively correlated with the degree of vasodilation after IA nimodipine injection. Likewise, the time interval between surgery and vasospasm was significantly positively correlated with the degree of vasodilation after injection. Our findings suggest that IA nimodipine injection for vasospasm after SAH is a safe and effective method to improve clinical outcomes, even though we did not observe a definite change in blood flow velocity in TCD.
Dispute still remains over the effects of IA nimodipine injection. In this study, we were able to suggest the positive correlation between nimodipine injection and changes in vessel diameter. However, additional studies regarding the limitations mentioned above and a large-scale study on IA nimodipine injection would be required. Nevertheless, IA nimodipine injection should be considered when intractable vasospasm develops despite rigorous conservative management.
 XML Download
XML Download