

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Anterior cervical discectomy and fusion (ACDF) has become a standard operative procedure for degenerative disc disease associated with radiculopathy or myelopathy10). Both ACDF and anterior cervical corpectomy and fusion with the plating method are well-known surgical treatments in patients with two level anterior cervical disc diseases. Two level ACDF methods can also be subdivided into several different methods including ACDF using tricortical autograft and plate fixation (ACDF-AP), ACDF using stand-alone cage (ACDF-CA), and ACDF using cage and plate fixation (ACDF-CP).
Several authors have suggested that there are advantages with iliac autografts and plating. ACDF with anterior plating provides lesser graft complications and higher fusion rates than ACDF without plating4,5,20,22). Fusion rates for, unplated two levels ACDF were reported to be about 50 to 80%, while plated two levels ACDF had 94 to 100% fusion rates. However, autografts are associated with significant donor-site morbidity. Acute pain, artery or nerve injuries, hematomas, fractures, infections are serious postoperative concerns and about 15% of patients complain of chronic donor site pain (>3 months)14,16,17).
In order to reduce iliac autograft related complications, several types of cervical interbody fusion cages, which have been developed
since the 1990s, are used widely in clinical practice. Many authors have suggested that ACDF-CA can provide immediate stability, increased disc and foraminal height, and solid fusion with few complications3,9,11,19,21). Cages, which have good structural strength, are made up of biocompatible materials such as Carbon, polyetheretherketone, and Titanium. Cages can be filled with cancellous autografts, allografts, demineralized bone matrix and bone morphogenic protein. However, stand alone cage fusion has also been reported to have some disadvantages. A significant reduction of segmental height, a loss of segmental lordosis, kyphotic deformity, and cage migration are well known complications1,2,6,7). Therefore, by combining the advantages of cage and anterior cervical plate, ACDF-CP has been recently performed.
The anterior cervical corpectomy and plate fixation (ACCF) is also an effective surgical treatment options for two level anterior cervical fusions. Between ACCF and ACDF with anterior cervical plating procedures, some controversies still existed with respect to graft collapse, postoperative cervical lordosis, and fusion rate12,13). Fraser and Härtl5) suggested that because corpectomy had only two graft-host interfaces, it has a higher fusion rate than two levels ACDF without plating. Wang et al.22) reported that there was no significant difference in the fusion rate between two level ACDF and ACCF.
The purpose of this study was to evaluate the radiographic results of four different anterior fusion methods in two-level cervical disc disease : ACDF-AP, ACDF-CP, ACDF-CA, and ACCF. There are few studies that have compared radiographic parameters such as fusion and subsidence rate, global cervical lordosis (GCL), cervical range of motion (ROM), fused segmental angle (FSA), fused segmental height (FSH) and instrument-and graft-related complications5).
MATERIALS AND METHODS
Patient population
We retrospectively reviewed the simple X-rays of 70 patients with two level cervical disc diseases who had anterior cervical fusion surgery at our hospital between 2006 and 2010. All patients had symptoms of neural compression at two adjacent segments that were refractory to conservative treatment. All patients were followed for a minimum of 6 months after the surgery.
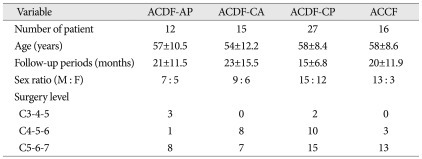
The operative levels were classified into C3-4-5, C4-5-6, C5-6-7 and number of included patients were 5, 33 and 43 consecutively. The number of patient of each group was 12 for ACDF-AP, 27 for ACDF-CP, 15 for ACDF-CA, and 16 for ACCF. Mean follow-up period and the mean age were 21 months, 57 years in ACDF-AP, 15 months, 58 years in ACDF-CP, 23 months, 54 years in ACDF-CA, and 20 months, 58 years in ACCF. Serial preoperative, postoperative and final follow-up simple X-rays and computed tomography (CT) scans were evaluated for radiological evaluation. GCL (C2-C7 Cobb's angle), cervical ROM, FSA and FSH at the operated segment were measured and analyzed. Graft- and instrument-related complications were also evaluated. The preoperative demographic data for each group are presented in Table 1.
Surgical procedures
We performed anterior cervical approach to gain access to the cervical spine. The operated level was defined with fluoroscopic control in supine position. After removing a portion of the anterior longitudinal ligament and intervertebral disc, we used the Caspar dilator to expand the interval between adjacent vertebral bodies by approximately 2 to 3 mm. The subchondral bone was exposed by removing osteophyte, remaining intervertebral disc, and the cartilaginous endplates of the upper and lower vertebral bodies. In case of ACCF, we performed subtotal corpectomy to removal of a 15 to 19 mm anterior midline trough in the vertebral body down to the posterior longitudinal ligament or dura, with removal of the cephalad and caudad discs15). The lateral extent of decompression is limited by the transverse foramen, which houses the vertebral artery. For subjects requiring spinal decompression, a portion of the posterior longitudinal ligament was also removed using microscope. Using lateral plain radiographs, we determined the cage size, the insertion angle of screws, and the angle of lordosis of the metal plates. For the segments to be fused, cervical lordosis was maintained by placing a cage (Fijit®, Rabea®, Solis®, mesh). In the cases with plate augmentation, we used anterior cervical plate (Atlantis® or ABC®). Bone graft was acquired via a 3 cm skin incision on the anterior superior iliac spine. We harvested sufficient block bone or cancellous bone to fill in the cage. In case of ACDF-CP, we used cancellous dried allograft to fill in the cage.
Radiologic parameters and evaluation
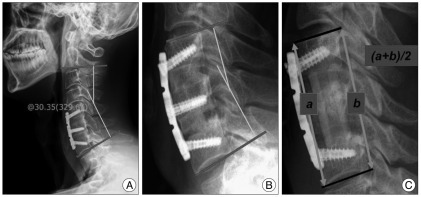
We reviewed lateral views of simple X-rays in flexed, extended and neutral position before surgery, 2 weeks after surgery, 6 months after surgery, and final follow-up after surgery. Fusion was defined as presence of trabecular bone bridging on simple X-ray or 3 dimensions-CT and no radiolucency between graft and adjacent vertebral body, and no motion at the fused segment. Subsidence was identified as cage or graft migration of 3 mm or more into the adjacent vertebral body on simple lateral X-ray18). This means the loss of FSH more than 3 mm. GCL was defined as the angle subtended by a line drawn parallel to the inferior endplate of the C2 vertebral body and a line drawn parallel to the inferior endplate of C7 vertebral body. FSA was defined as the angle between the lines drawn parallel to the cranial endplate of the cranial vertebra of fused segment and the caudal endplate of the caudal vertebra of fused segment. FSH was determined as the mean value of anterior and posterior vertebral body heights at the fused segments (Fig. 1). Cervical ROM was defined as difference value between GCL in extension neck position and GCL in flexed position.
RESULTS
At the last follow-up, the fusion rates in ACCF were achieved 100%. However, one patient (8%) in ACDF-AP, one patient (4%) in ACDF-CP, and 4 patients (25%) in ACDF-CA were failed fusion. In spite of relatively long follow-up time, the pseudarthrosis rate was 25% in ACDF-CA. There were no instrument-related complications in each group. The rate of subsidence more than 3 mm was 16% (2 patients) in ACDF-AP, 33% (5 patients) in ACDF-CA, 11% (3 patients) in ACDF-CP and 20% (3 patients) in ACCF.
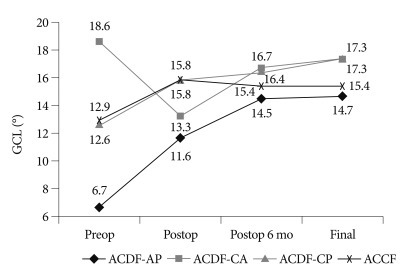
The mean CGL (C2-C7 lateral Cobb angle) was decreased in ACDF-CA (from 18.6±10.0 to 17.3±9.8°) at final follow-up and the others were increased (from 6.7±14.0 to 14.7±8.2° in ACDF-AP, 12.6±9.8 to 17.3±7.6° in ACDF-CP, and 12.9±9.8 to 15.7±8.6° in ACCF) (Fig. 2, independent t-test, p=0.043).
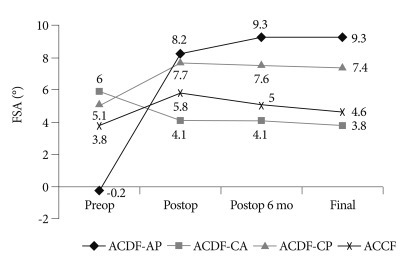
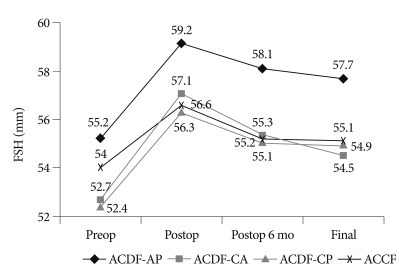
The mean FSA was increased in ACDF-AP, ACDF-CP and ACCF except for ACDF-CA (Fig. 3, independent t-test, p=0.023). The mean FSH after operation was slightly decreased in ACDF-CP (from 52.4±3.7 to 54.9±4.2 mm), ACDF-AP (from 55.2±3.1 to 57.7±2.5 mm), and ACCF (from 54.0±2.9 to 55.1±3.9 mm) except for ACDF-CA (from 52.7±4.0 to 54.5±3.0 mm) at the final follow-up (Fig. 4).
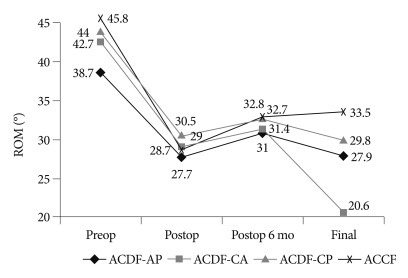
The mean ROMs in groups were significantly decreased at the postoperative, but during follow-up period, the value of ACDF-CA group was rapidly decreased (42.7±12.7 to 20.6±13.8°). The other groups showed no significant differences (Fig. 5).
The complications were analyzed and reviewed : graft-related complications were developed in 2 patients in ACDF-AP, 5 patients in ACDF-CA, 3 patients in ACDF-CP, 3 patients in ACCF groups. Screw loosening, plate fracture, cage subsidence and migration were not identified.
DISCUSSION
In patients with two level cervical disc diseases, the most commonly performed anterior procedures have been two level ACDF or ACCF. In terms of fusion rate, Fraser and Härtl5) reported that fusion rates were 79.9% for stand-alone ACDF, 94.6% for ACDF with plating, 95.9% for corpectomy, and 92.9% for corpectomy with plate placement (p=0.0001) in two level cervical disc disease. There was no significant difference in fusion rates between two level ACDF and ACCF in their results. Song et al.18) have argued that the fusion rates were 66.7% in two level ACDF-CA, 95.5% in two level ACDF-CP. Also, fusion time was significantly delayed in two level ACDF-CA in comparison with ACDF-CP. Another suggested that non-union rates for two-level ACDF-CA may be as high as 25%22). Hwang et al.8) reported that the fusion rates in ACDF-CP and ACCF groups were achieved 100% in two level degenerative disc disease. In this study, the fusion rates in ACCF were achieved 100%. However, one patient (8%) in ACDF-AP, one patient (4%) in ACDF-CP, and 4 patients (25%) in ACDF-CA were regarded as failed fusion. Our results of bony fusion were very similar to other papers5,8,12,18). In our data, in spite of mean follow-up times in ACDF-CA (12±5.1 months) and ACCF (14±7.6 months) was little short, the complete bony fusion rates confirmed by 3 dimensional CT were much higher than ACDF-CA.
Park et al.13) have reported that graft subsidence and loss of cervical lordosis appeared to occur mainly during the first 6 weeks after surgery, and there was no significant difference between two-level ACDF-CP and ACCF. Song et al.18) defined cage subsidence, as a disc height discrepancy of greater than 3 mm, that occurred in 32.3% of two level ACDF-CA and in 9.7% of two level ACDF-CP. Our data of subsidence rate were also higher in ACDF-CA (33%) or ACCF (20%) than in ACDF-AP (16%) or ACDF-CP (11%). Lower fusion rates and higher subsidence rate in ACDF-CA highly suggests that two level stand-alone cage fusion is not sufficient condition for successful bony fusion even though autologous iliac bone is used, and additional anterior cervical plate fixation might increase fusion rate in two level cervical disc disease.
About GCL, Oh et al.12) have published study finding concerned lordotic curvature, for although cervical lordosis in the two level ACDF-CP from 20.5° to 23.4°, it decreased in the ACCF from 17.3° to 14.6°. Park et al.13) have reported that mean loss of cervical lordosis was 5.3° in the ACCF and 3.9° in the two level ACDF-CP. Cobb's angles measured between C2 and C7 as well as at the fused segment were statistically similar in both groups. In our study, the values of GCL in two levels ACDF-CP were increased from postoperative to final follow-up values. However, ACCF had decreased from postoperative to final follow-up values. Also, the values of GCL in two levels ACDF-AP and ACDF-CA showed significant difference in our study.
In the viewpoint of FSA, Song et al.18) reported that the average lordotic angle of fused segments were changed from preoperatively to immediately postoperatively in two level ACDF-CA from 2.9° to 7.2°, in two level ACDF-CP from 1.6° to 11.4°. Then, at final follow-up, the mean FSA in ACDF-CA was 0.8°, which in ACDF-CP was 5.5°. Segmental kyphotic deformity of fusion level or index level developed in 42.1% of two level ACDF-CA and 10% of two level ACDF-CP. Oh et al.12) suggested that the values of FSA were statistically similar between ACCF and two level ACDF-CP. Our data of FSA in two level ACDF-AP, ACDF-CP and ACCF were increased but the value of ACDF-CA was decreased at the final follow-up. The values of ACDF-CP and ACDF-AP groups were significantly increased than those of ACDF-CA and ACCF groups at the final follow-up. These results suggest that anterior cervical plating maintains segmental and overall cervical lordosis.
With regard to FSH, Song et al.18) reported that the degree of disc height change of the fused segment, postoperative immediately compared to preoperative, was +1.9 mm in two level ACDF-CA and +4.7 mm in two level ACDF-CP. At final follow-up, it decreased 3.8 mm in ACDF-CA and 3.0 mm in ACDF-CP.
Oh et al.12) suggested that the FSH in the ACCF was significantly smaller than in the two level ACDF-CP. Park et al.13) reported that the FSH were significantly increased at the post operative period and slowly decreased as time passed. But, there were statistically similar between ACCF and two level ACDF-CP. The values of FSH in our study, all groups were significantly increased at the postoperative period, but the mean value of ACDF-CA was rapidly decreased during the follow-up. The others were no significant differences.
In terms of ROM, Oh et al.12) reported that total and segmental ROMs showed no significant intergroup differences. The values of ROM in our study, all groups were significantly decreased at the postoperative, and mild increased at postoperative 6 months. But during follow-up period, the value of ACDF-CA was rapidly decreased. The others showed no significant differences. Decreased values of ROM in ACDF-CA at the final follow-up are supposed to associated with increased neck discomfort and straightening of cervical curvature.
ACDF-CP demonstrated relatively high fusion rate (96%) and minimal height loss than other fusion procedures in two level cervical disc diseases. ACDF or ACCF with plating groups were better results than stand-alone cage fusion in terms of GCL, FSA and FSH.
There are some limitations in this study. Being a retrospective study, we were not able to perform direct comparison, because follow-up periods of each groups are different. Therefore, long-term follow-up studies are necessary, which we plan to pursue in the future.
CONCLUSION
The cage plating method (ACDF-CP) demonstrates a higher fusion rate and minimal loss of FSH than the other three fusion procedures in patients with two level cervical disc diseases. Our data also indicate that ACDF or ACCF with plating groups show better radiographic results than stand-alone cage fusion with respect to GCL, FSA, and FSH.
No donor site morbidity, no external rigid brace, and early return to work could be advantageous in cage filled with allograft and plating method. However, prospective long-term and large multicenter study for the acceptance with new standard ACDF method in two level ACDF surgery will be necessary.
 XML Download
XML Download