

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Effective pain control in surgical procedures still remains a challenge for all dental professionals. The optimum profoundness of anesthesia is limited in the mandible area [1]. Wong [2] revealed in his systematic review that inferior alveolar nerve block injection (IANBI) has a success rate of only 69%. Thus, there is a 15% to 20% failure rate associated with IANBI technique. Several patient-related idiosyncrasies contribute to IANBI failure, including the complicated anatomical distribution of the nerve, and the thickness of the cortical plate of the mandible and the zygomatic process bone, which can also prevent the diffusion of the anesthetic agent, leading to failure of the anesthesia [2].
1. Intraosseous injection
Intraosseous injection (IOI) is an alternative anesthetic injection technique in which the needle is inserted directly into the cancellous bone. It was first described around a hundred years ago. It is considered an effective technique to achieve profound anesthesia without lips and cheek tissue numbness. Previous review articles showed that IOI has an anesthesia success range of 40–100%. The technique is recommended in extremely painful conditions, when most regional blocks have failed to control the pain. However, the use of IOI technique may provoke root damage of the adjacent teeth, fracture of the drill, and overheating during the perforation of the cortical plate that could cause osteonecrosis as a postoperative complication [34].
The IOI is an alternative choice when performing dental treatments. It has been reported that IOI can be used as an additional injection method to cover the failure of IANBI. Several studies in cases of irreversible pulpitis claim a success rate of 71% to 98% [56789]. Besides its effectiveness, IOI requires less anesthetic volume than the conventional IANBI technique.
2. Computer-Assisted intraosseous injection (CAIOI)
CAIOI is a type of the machine recently introduce in the field of dentistry to attempt a more advantageous type of inferior alveolar nerve block. The system works in one of two ways:
Quicksleeper® (Dental Hi-tec, Cholet, France) is a one-step IOI machine for CAIOI. This computer-controlled local anesthesia delivery system (CCLAD) is designed to be a pen-grasp like injection syringe that fully monitors the speed of diffusion and the volume of the anesthetic agent into the cortical bone by means of a Bluetooth pedal. CCLAD have been utilized for pain control in several kinds of dental procedures including endodontic treatment of irreversible pulpitis, periodontal surgery, surgical removal of mandibular third molar, dental implant surgery and dental procedures in pediatric patients.
It has been reported that this type of IOI has an 87% success rate, versus to 60% of conventional IANBI. Additionally, it was shown that this type of IOI produces a shorter duration of anesthesia than the conventional IANBI technique, an effect that is desirable [10]. However, a major drawback is that the device is not recommended for long duration anesthesia for dental treatments such as mandibular third molar removal [111213].
3. Quicksleeper®
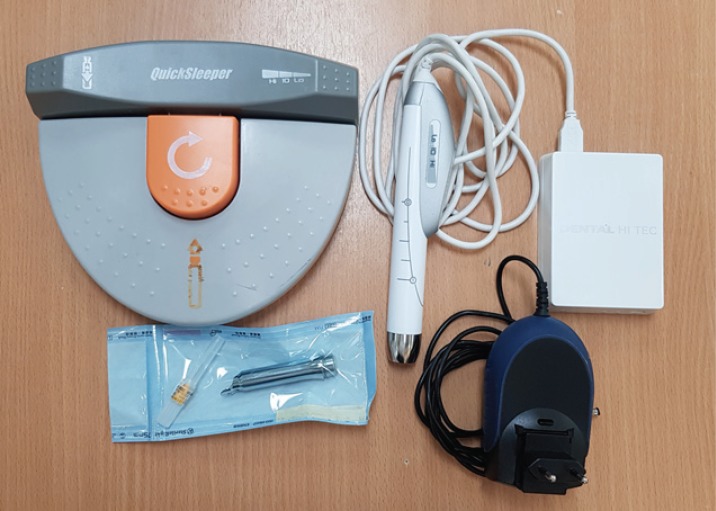
According to instruction manual from Dental Hi-tec, Quicksleeper® is on its 5th generation (Fig. 1). The machine has a rotary motor in the handpiece, and the control system is in the control box. The dentist can use a pedal to send signal via Bluetooth to the main control box, so that the handpiece can be used for drilling and administering anesthetic injection into the intra-bony space or cancellous bone. The local anesthetic will spread into the bone. After the use of this machine for injection there is a maximized efficiency of anesthesia, especially in cases of mandible third molar operation. The machine can be used to achieve an efficient inferior alveolar nerve block in the retromandibular area behind the mandibular third molar. Both patients and dentists report satisfaction with its effectiveness in anesthesia.
Smaïl-Faugeron et al. conducted a randomized controlled trial study to compare IOI done with Quicksleeper® and infiltrations done with traditional syringes in pediatric patients. The result showed that the use of the Quicksleeper® system provided good results for dental practitioners. It required less pressure and a lower amount of anesthetic agent. The study also stated Quicksleeper® generated less pain and less anxiety than conventional anesthesia techniques, which is beneficial when dealing with the health care of children and adolescent patients [14].
Kiattavorncharoen et al. [12] studied the use of CAIOI in third molar surgery in 2013 in a split-mouth study, using a previous generation Quicksleeper®. They injected at the interdental papillary bone of the first and second molar by using 4% articaine as their local anesthetic. The outcome of the study showed that one-third of the patients required additional anesthesia during the surgical procedure. However, it also showed that the pain intensity was significantly different during the injection.
The present study ais to evaluate the effectiveness of 4% articaine HCl applied by IOI using Quicksleeper® injection at the retromolar area compared to the conventional nerve block injection method used in mandibular third molar surgery. The Quicksleeper® technique has not been used in this specific location before.
METHODS
1. Patients and methods
This study was authorized by Committee for Ethics of Research in Human Beings of the Dentistry and Pharmacy Mahidol University Institutional Review Board, Protocol No. MU-DT/PY-IRB 2018/008. All patients were informed thoroughly about the study. All patients signed informed consents before the interventions.
The study cohort consisted of 25 patients (10 males and 15 females, mean age 21 years). The patients were randomly allocated to use the local anesthetic injection techniques by a simple randomizing method. Each patient underwent two different surgical appointments of bilateral mandibular impacted third molar removal and a 4-week washout period was allowed in each case.
The patients were injected with a different technique at each appointment. One side was injected using conventional IANBI, the other side was injected using CAIOI with the Quicksleeper® device (Dental Hi-tec, Cholet, France).
2. Patient selection
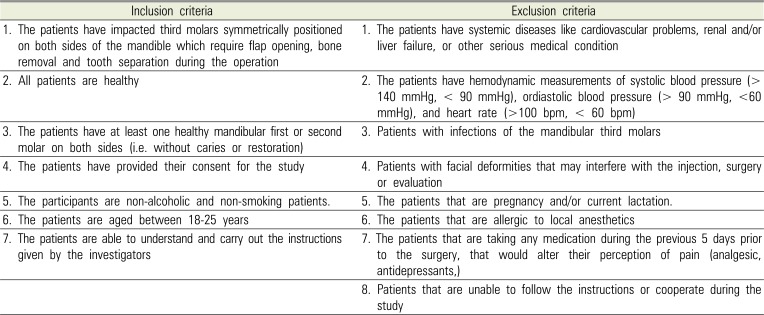
Table 1 showed the inclusion and exclusion criteria for patient selections, and the patients were allowed to withdraw their participation in the study at any time of their own will.
3. Technical procedure
3.1 Pre-operatory period
An electric pulp tester was used on the mandibular second molar before the injection with Quicksleeper® to identify the efficacy of the anesthesia. Pre-operative hemodynamic measurements were also recorded as baseline.
3.2 Injection techniques (Fig. 2)
The Quicksleeper® device was used to inject in the retromolar trigone area. The device was set up and the injections were performed following the manufacturer's instructions. ADHT 27G-16 mm was used (DHT needles are compatible with Quicksleeper®). CAIOI was performed in three steps.
1) The first step is to injection on the mucosa area. The angulation of the needle is almost parallel to the buccal mucosa, ensuring a minimum depth of penetration, avoiding the periosteum. Only a small amount of anesthetic solution is used to prevent tissue necrosis.
2) The second step is transcortical perforation. The handpiece is pointed to the inferior border of the ramus. Then, the needle is set at a right angle to the cortical bone (perpendicular to the floor) in the bony depression at the middle of the external oblique line on the buccal side of the mandible.
3) The last step is the infusion of the anesthetic solution into the cortical bone. In the second surgical appointment, a standard IANBI technique was used.
3.3 Surgical procedure
A standard surgical technique for mandibular third molar surgery was used. The steps included flap elevation, buccal bone removal, odontectomy, tooth elevation and wound closure. Hemodynamic measurements at each step of the surgical procedure were recorded. If the participant felt sensitivity or pain during the operation, additional local anesthetic was administered. The total volumes of the local anesthetic used were recorded.
3.4 Post-operative management
All patients were required to complete a form for evaluation of the duration of anesthesia and postoperative complications. Following surgery, each patient was prescribed the following medications: amoxicillin (500 mg) 1 tablet 4 times a day for 5 days, if the patient is allergy to amoxicillin, clindamycin (300 mg) 1 tablet three times a day for 5 days. The pain medication recommended was ibuprofen (400 mg), 1 tablet three times a day or paracetamol (500 mg) 1 tablet every 4 hours if necessary.
RESULTS
Table 2 shows the subjective onset, objective onset and latency of the anesthetic agent from both techniques. CAIOI provided faster subjective onset (35.40 ± 13.84 sec) than IANBI (65.60 ± 24.38 sec) (results are statistically significant. As for the objective onset, CAIOI provides faster objective onset (90.6 ± 45.21 sec) than IANBI (136.00 ± 66.99 sec), P < 0.001. Table 2 also shows the latency of the anesthetic agent from both techniques. The CAIOI (243.56 ± 38.02 sec) has shorter duration of action than IANBI (291.6 ± 40.28 sec) despite the fact that 4% articaine was used for both techniques (P < 0.001).
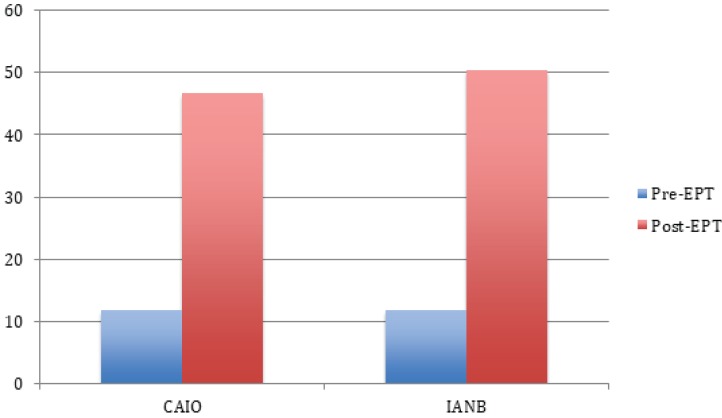
EPT testing showed very similar results for both techniques, both for pre-injection EPT and post-injection EPT (P > 0.05) (Fig. 3).
Patients reported feeling more comfortable receiving intraosseous injection with Quicksleeper® than IANBI with conventional syringe. Nonetheless, the data calculation does not show any significant differences between the two techniques (P > 0.05).
Even when additional anesthetic agent was required, patients reported less pain during the operation as shown in Table 3. The statistical analysis did not reveal any significant differences between pain reported from either type of injections (P = 0.408), or on the success rate of anesthesia for the mandibular third molar operation. IANBI had a higher success rate than CAIOI, (72% compared to 68%) but the difference is not statistically significant (P > 0.05) (Table 3).
DISCUSSION
In a previous study, Gonzales-Castro et al. concluded that the use of CCLAD gives patients more comfort and less anxiety during anesthetic administration [15], while failure of IANBI is the main reason for needing supplementary IOI injection.
Patients report immediate onset, as described in several studies by Daniel Dunbar et al. [16], Replogle et al. [17], Jensen et al. [18], Beneito-Brotons et al. [19] and Prohic et al. [20]. Further reviews show that IOI produces a desirable success rate and can be used as the primary injection technique to anesthetize mandibular molars.
We studied CAIOI versus IANBI, using a 5th generation Quicksleeper® with Bluetooth pedal for the CAIOI, an innovative technology.
Smaïl-Faugeron et al. performed a controlled trial study that compare pain induced by IOI with Quicksleeper versus infiltration with conventional syringes in pediatric patients. The result showed that the use of the Quicksleeper® system is significantly advantageous for dental practitioners. It required less pressure and a lower amount of anesthetic agent. Their study also indicated that Quicksleeper® induced less pain and less anxiety than the conventional anesthetic technique, and that is beneficial when treating children and adolescent patients that require their oral health care [14].
Similarly, in 2012 another study by Beneito-Brotons et al. on intraosseous anesthesia with CAIOI system versus conventional nerve block anesthesia showed that IOI with Quicksleeper® caused less discomfort than IANBI. It also proved that the onset of anesthesia on soft tissue was significantly faster with Quicksleeper® as it took 35–90 sec for patients to feel the numbness, which is different from the conventional IANBI method. In that study, 69.7% of patients preferred Quicksleeper® injection compared to 23.3% that chose the conventional IANBI technique when inquired [19].
Terrer et al. compared osteocentral (intraosseous) anesthesia and local regional block on inferior dental nerves in 39 patients. Twenty-one patients were anesthetized by CAIOI with Quicksleeper® and 19 patients were injected using IANBI. The time of anesthetic onset was 2.9 min for Quicksleeper® injection and 8.1 min for IANBI respectively. In that study, 18 of 21 patients could be treated immediately after Quicksleeper® injection, a success rate of 86% succeeded. Only five patients could undergo dental treatment after the first IANBI, while 11 patients required a second injection and two needed a third injection [21].
Cabasse et al. studied 39 children and adolescents treated for molar and incisor hypomineralization by using CAIOI with Quicksleeper® injection. Around 93.5% of the patients achieved full anesthesia. Failure was related to the density of the bone, when the needle could not penetrate into the spongy bone [22].
The study of Couderc et al. followed 25 patients who came for emergency treatment at the dental hospital. Most of the patients were diagnosed with pulpitis, either reversible or irreversible. The study followed those patients who fail to control the pain after the first attempt. The supplementary techniques used were intraosseous injection with Quicksleeper® or intraligamentary injection. That study reported that all patients who received additional injection with Quicksleeper® were able to complete the treatment and required less amount of anesthetic agent [23].
Chang and colleagues [24] conducted a study using CCLAD as the primary anesthesia technique in chronic periodontitis patients who required surgical debridement. The result indicated that the mean VAS pain score in patients treated with the CCLAD procedure was significant lower than the group that received conventional injection.
A case report study by Han et al. [25] and Kim et al. [26] showed that none of the patients that received a Quicksleeper® injection prior to their periodontal surgery claimed discomfort after the treatment despite undergoing multiple root planning on both the mandible and the maxilla.
A split-mouth study by Demir and Ataoglu [27] on surgical removal of impacted mandibular third molars reported that more than 60% of the patients showed high level of satisfaction after receiving injection with Quicksleeper®. They reported significantly less pain, less tissue numbness, and a faster onset of anesthesia.
In our study patients reported onset of numbness at 35.40 ± 13.84 sec in CAIOI and 65.60 ± 24.38 sec in IANBI (P < 0.05). The subjective onset in our study is longer than previously reported by Beneito-Brotons et al. in 2012 [19]. In that study, it took 0.48 ± 0.32 min, average 28 sec for patients to realize the numbness sensation after using Quicksleeper®. That subjective onset is significantly shorter than the one reported by Terrer et al. [21] (2.9 minutes). In another study, Kiattavorncharoen et al. [12] reported a subjective onset of 5.8 ± 3.5 min, and an objective onset was 14.6 ± 10.6 min, which are longer than in our current study. The reason for that may be the different injection point used, as they injected at the retromolar trigone area to perform mandibular third molar surgery. In that study the complete loss of numbness in the CAIOI group was at 243.56 ± 38.02 min compared to 291.6 ± 40.28 min for the IANBI group. In comparison, in the previous study by Kiattavorncharoen et al. [12], the soft tissue numbness was shorter than in this study. The different in onset might probably due to the density of the cortical bone in the mandible.
The profoundness of anesthesia has been the object of many discussions. It has been suggested that IOI is not suitable for longer duration of dental treatments such as mandibular third molar surgery. The EPT test after injection showed that the EPT value in the CAIOI group was lower than in the IANBI group but the P-value showed no statistical significance.
In our study, one-third of the cases where CAIOI was used required additional anesthesia during the operation. The requirement of additional anesthesia may result from inadequate effect of IOI. This explains why the hypersensitivity disappeared after an additional minimal amount of articaine was administered using a conventional syringe.
A study by Ozer did not show any significant difference between injections. In contrast, the previous study of Kiattavorncharoen et al. [12] used the previous generation Quicksleeper® and was injected at the interdental papillary bone of the first and second molar by using 4% articaine as their local anesthetic. They mentioned that the CAIOI produced less pain during injection that is parallel to this current result, which shows that IANBI causes discomfort during the needle insertion. However, all study outcomes showed less pain during injection in CAIOI versus IANBI but the differences do not reach statistical significance.
The success rate in this study was 68% in CAIOI group and 72% in IANBI group. The profoundness of anesthesia was sufficient in 32% of the case in CAIOI group, and 36% more cases could be completed with mild sensitivity if intra-pulpal injection was added. The result is similar to the study by Ozer et al. [13], which found that in 70% of the cases when CCLAD was used they were able to complete the surgical removal of third molar, even in those patients who feel sensitivity.
We conclude that the use of CAIOI with Quicksleeper® in mandibular third molar operation could provide faster onset of anesthesia, both subjective and objective, and shorter duration of action than IANBI with conventional syringe. The major drawback of this device is the lack of profoundness of anesthesia. The success rate in these two injections technique is 68% and 72% for CAIOI and IANBI respectively.
In conclusion CAIOI could be an alternative injection technique to perform the operation instead of IANBI with traditional syringe. The researcher recommends further studies to address the weaknesses of this study. Some of the caveats include that the researcher could not blind the patients, as there two different injection techniques despite having turned the Quicksleeper® on when injecting with the conventional syringe. The patients' experience, as well as their anxiety about the removal of the mandibular third molar might have a strong impact on the hemodynamic changes observed during this study.



 XML Download
XML Download