

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Magnetic resonance imaging (MRI) is commonly used to study brain tumors. Tumor-related white matter change is usually detected at late stage when the mass effect or prominent edema is present [12345]. Because gliomas initially spread along the white matter without causing noticeable changes in routine MRI, tumor extent can be larger than shown by MRI [1234678]. This observation is supported by histopathology [48]. Information about whether the tumor has invaded to white matter tract could have significant implication for the planning of surgical procedures or radiaotherapy. Diffusion tensor imaging (DTI) may detect white matter abnormalities before they are evident by routine MRI, therefore may be useful for the early detection of brain tumors [1235910111213]. The object of this study is to assess change of parameters of DTI for the early detection of tumor-related white matter changes.
MATERIALS AND METHODS
Subjects
Between 2005 and 2008, 26 patients whose gliomas were within 2 cm from the posterior limb of the internal capsule (IC) were tested. Patients, whose MRI was obtained before steroids medication and before surgery, were selected to reduce the effect of steroid [1415]. The tumor was removed as completely as possible in all patients. Five had World Health Organization (WHO) grade II gliomas, 12 had grade III, and 9 had grade IV. The fluid attenuation inversion recovery (FLAIR) 3.0 T MRI (General Electric VH/i, Milwaukee, WI, USA) showed a high signal change in the IC (HSIC) in 9 patients with grade III or IV gliomas. Patients were reclassified according to the grade of tumor and presence or absence of HSIC:WHO grade II [gliomas II, early stage], grade III or IV without HSIC [gliomas III/IV (-), covert stage] and grade III or IV with HSIC [gliomas III/IV (+), overt stage]. This order is considered to reflect the increase in the severity of the changes caused by the tumor (Table 1, Figs. 1, 2, and 3). After operation, patients were treated with chemotherapy and/or radiotherapy. Tumor progression along pyramidal tract could be evaluated by follow-up MRI in 16 patients at 40±18 months, but follow-up MRIs were not available in the other patients. Fifteen neurologically healthy right-handed normal adults (7 male and 8 female at the age of 33.9±2.6 years) were the control subjects. Informed consent was obtained from all subjects. Handedness was determined using the Edinburg handedness inventory [16]. All subjects scored less than -80 on the Edinburg handedness inventory indicated strong right-handedness. Values of normal subjects were compared with values from patients' groups. This study was approved by the Institutional Review Board at our hospital (H0806-041-243).
Diffusion tensor imaging protocol
DTI was acquired using a 3.0 T MR scanner (General Electric VH/i, Milwaukee, WI, USA) with a conventional head gradient coil. We used a single-shot spin-echo echo planar imaging sequence. The B-factor was set at 1,000 sec/mm2. The acquisition parameters were: field of view=240 mm, matrix=256×256, slice thickness/gap=3.5 mm/0 mm, total slice number=38, repetition time/echo time=10,000 ms/90 ms, and scan average=1. To estimate the intensity and direction of the diffusion anisotropy, MRI with 25 noncollinear diffusion gradients without diffusion gradients were acquired. From 26 diffusion-weighted images, we obtained six diffusion tensor components, namely, Dxx, Dyy, Dzz, Dxy, Dxz, and Dyz, using multiple linear equations. We determined the direction of the fiber tracts from Vmax, i.e., an eigenvector maximum eigenvalues of three eigenvectors obtained by the eigen-decomposition of the diffusion tensor.
Data processing
We performed two data processing procedures. First, the digital images from all subjects were stored as digital imaging and communications in medicine (DICOM) files using the picture archiving and communication system. The DICOM files were converted for analysis using the MRIcro program (version 1.40, University of South Carolina, Columbia, SC, USA, www.mricro.com). Second, tractographic analysis was performed using the DTIstudio (Johns Hopkins University, Baltimore, MD, USA, www.mristudio.org) program. The advanced fast marching tractography algorithm in this program was used to follow the fiber tracts [17]. The tracts were defined to begin where the fractional anisotropy (FA) was greater than 0.1 and traced until they reached voxels with an FA of less than 0.1 or turned at an angle greater than 70 degrees [18].
Tractography
We used the 'two ROIs method' to trace the pyramidal tract [19]. All processing was performed by one image analyzer (CHK) [20]. We located the first region of interest (ROI) at the posterior limb of the IC from a color-coded FA map. The second ROI was located on the cerebral peduncle and those fibers that passed through both ROIs were selected. The FA and apparent diffusion coefficients (ADC) were calculated from each whole pyramidal tract.
Statistical analysis
The Kruskal-Wallis and Mann-Whitney U test were used to compare the two hemispheres and groups. A p-value of less than 0.05 (two-sided) was considered to be statistically significant. All analyses were performed using commercially available software (SPSS version 12.0, SPSS Inc, Chicago, IL, USA). The post hoc analysis was performed using Bonferroni's method.
RESULTS
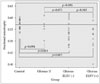
There was no difference in FA or ADC between the two hemispheres in normal subjects (p>0.05, Kruskal-Wallis test) (Table 2). We used left-side values to simplify comparisons. In early stage (gliomas II), FA was the same as control subjects, whereas ADC was higher than control subjects (p=0.694 and 0.001, respectively, Mann-Whitney U test) (Table 3, Figs 1, 4, and 5). FA was lower in the covert stage [gliomas III/IV (-)] and overt stage [gliomas III/IV (+)] (p=0.003×10-1 and 0.003, respectively, Mann-Whitney U test) (Table 3, Figs 2, 3, 4, and 5). ADC was higher in both covert and overt stages than in control subjects (p=0.002 and 0.004×10-2, respectively, Mann-Whitney U test) (Table 3, Figs. 2, 3, 4, 5). ADC was higher in the presence of HSIC (p=0.031) (Table 3, Fig. 5), whereas there was no difference in FA values (p=0.943) (Table 3, Fig. 4) between gliomas III/IV (-) and gliomas III/IV (+). Horizontal line in Figs. 4, 5 indicated mean FA and ADC values of normal subject (FA=0.57 and ADC=2.33×10-3). Among the 16 patients, who underwent MRI follow-up, tumor progression along pyramidal tract was observed in 2 patients; cerebral peduncle in Patient 1, and coronal radiata in Patient 9.
DISCUSSION
Stage of tumor-related white matter change
We attempted to determine whether DTI detects tumor-related white matter changes earlier than routine MRI. We classified the severity of the white matter change as early, covert and overt stages. Although this classification seems arbitrary, we suggest that it reflects the severity of tumor-related change in white matter [123467]. We believe that this is the first study linking white matter structure with the severity of changes caused by gliomas. However, without histological confirmation, our classification just suggested a possible severity of change in white matter caused by the tumor.
It has been reported that in untreated brain glioblastoma, the extent of tumor is well correlated with MRI finding and tumor cell extended to the white matte change [4]. Usually, tumor cell is known to be exist to high signal change in FLAIR MRI and this is corresponded to overt stage [gliomas III/IV (+)] in the present study [4]. We divided high-grade gliomas according to the presence of high signal change in white matter. All selected gliomas were within 2 cm from the IC and may have the potential to infiltrate IC [24212223]. Glioma cell may exist in white matter although there was no high signal change in FLAIR MRI [covert stage, gliomas III/IV (-)].
We evaluate the status of white matter by change of ADC and FA values. The Change of FA value was known to be correlated with tumor cell density [242526]. This result is supported by histological comparison study with DTI [2]. Gliomas III/IV (-) and (+) showed that FA was lowered than control and this may be interpreted as tumor cell infiltration [12391011121326]. There was no difference in FA between Gliomas III/IV (-) and (+) and this may imply that tumor cell may exist even though there was no signal change in FLAIR MRI. The difference between gliomas III/IV (-) and gliomas III/IV (+) was increased ADC values and this may be explained as further edematous change after tumor infiltration [12391011121326]. At an early stage, there was an increase in ADC without change of FA. Even though many report support that FA change is correlated with tumor cell infiltration by histological confirmation, there is limited data about solitary ADC change [13262728]. The detection of tumor infiltration by ADC has been demonstrated in several studies comparing malignant gliomas with other noninfiltrating tumors and ADC change was considered to reflect tumor infiltration [13262728]. However, ADC change is usually interpreted as tumor infiltration when accompanied by FA change [13262728]. Moreover, there is report which showed no change of ADC or FA in low-grade glioma [7]. ADC could be changed in edematous situation and there is also individual variation [28293031]. With small number of patients, differentiation between tumor infiltration, edema and individual variation was not possible. Without histological confirmation, we could not interpret ADC change as tumor infiltration and the term 'tumor-related white matter change' would be reasonable expression.
The follow-up image
We assumed that FA and ADC changes may reflect white matte change and these changes may be correlated with tumor cell infiltration [12391011121326]. However, without histological data of our subjects, these were just assumption and follow-up image was used for interpretation. In the present study, even though change of ADC and FA were prominent, there was no progression of tumor in most cases. Tumor progression was detected only in one patient with Glioma II and one with Glioma III/IV (-). This result may be interpreted as no tumor infiltration in most cases. However, we should think about following factors. First, ADC and FA could be changed in both edematous situation and tumor infiltration [28293031]. Although some authors suggested that DTI may differentiate edematous change from tumor infiltration, this result was not conclusive [22930313233]. Lunsford et al. [34] reported that 'Tumor boundaries extended beyond the computed tomography or MRI margin in 4/4 of glioblastoma, 1/3 of anaplastic astrocytoma and 1/6 of astrocytoma' with stereotactic biopsy. Our case may include both edematous change and tumor infiltration in case of gliomas II or gliomas III/IV (-) [28]. However, even in cases of gliomas III/IV (+), which is regarded as definite tumor infiltration, the progression was not detected. Second explanation is the effect of adjuvant therapy. Most patients underwent adjuvant therapy such as radiotherapy or chemotherapy. This may halt progression of tumor, even though there was tumor infiltration in the pyramidal tract. However, without histological confirmation, these were just assumption.
The threshold of FA
Because tractography only shows a portion of the intact fibers, it may under- or over-estimates fiber status [3335]. A DTI study of gliomas suggested that an FA threshold of 0.15 is reasonable [33]. However, another study used the threshold of 0.12 to detect fibers that were not detected with a threshold of 0.14 [36]. These findings imply that parameter of DTI may change according to threshold of FA. We used the FA threshold of 0.1 to include as many potential fibers passing through IC as possible [33]. Our threshold is somewhat arbitrary in the absence of agreement on the appropriate threshold for detecting all fibers [35]. False positives may result from increasing the sensitivity. Further larger studies with histological verification are required to determine the practical threshold for FA.
Limitations of study
We have demonstrated the possibility of using DTI for the early detection of glioma-related changes in white matter. This might be clinically useful in assessing tumor progression following treatment. However, there are several limitations in this study. First, we examined a relatively small number of patients and there may be inborn individual variation. Second, we did not classified according to age and there may be age effect, although there is one report that showed no change of diffusion anisotropy with age [37]. The most significant drawback in our study is the lack of histological evidence. If this finding was verified with pathologic examination, this might be clinically useful in assessing or predicting tumor progression. Because the link between increased ADC and tumor infiltration was not histologically verified, there is the possibility that the increase in ADC merely reflects vasogenic edema without tumor infiltration [4212228]. At present, discrimination tumor infiltration from vasogenic edema with DTI is not accurate [28]. Finally, we could not verify tumor progression, because observation without adjuvant therapy was impossible. Despite these limitations, our results suggest that DTI (especially ADC) may be an useful tool for the early detection of tumor related white matter change. However, this result is a preliminary one and to apply in clinical practice, a study of a larger number of patients with histological confirmation is required.
In conclusions, DTI detected changes in white matter that appeared to be normal in routine MRI. ADC changed earlier than FA, indicating that ADC may be a better parameter for the early detection of white matter change. However, more cases should followed-up to corroborate clinical significance.






 XML Download
XML Download